Deprecated (16384): The ArrayAccess methods will be removed in 4.0.0.Use getParam(), getData() and getQuery() instead. - /home/brlfuser/public_html/src/Controller/ArtileDetailController.php, line: 150
You can disable deprecation warnings by setting `Error.errorLevel` to `E_ALL & ~E_USER_DEPRECATED` in your config/app.php. [CORE/src/Core/functions.php, line 311]
deprecationWarning - CORE/src/Core/functions.php, line 311
Cake\Http\ServerRequest::offsetGet() - CORE/src/Http/ServerRequest.php, line 2421
App\Controller\ArtileDetailController::index() - APP/Controller/ArtileDetailController.php, line 150
Cake\Controller\Controller::invokeAction() - CORE/src/Controller/Controller.php, line 610
Cake\Http\ActionDispatcher::_invoke() - CORE/src/Http/ActionDispatcher.php, line 120
Cake\Http\ActionDispatcher::dispatch() - CORE/src/Http/ActionDispatcher.php, line 94
Cake\Http\BaseApplication::__invoke() - CORE/src/Http/BaseApplication.php, line 235
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Routing\Middleware\RoutingMiddleware::__invoke() - CORE/src/Routing/Middleware/RoutingMiddleware.php, line 162
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Routing\Middleware\AssetMiddleware::__invoke() - CORE/src/Routing/Middleware/AssetMiddleware.php, line 97
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Error\Middleware\ErrorHandlerMiddleware::__invoke() - CORE/src/Error/Middleware/ErrorHandlerMiddleware.php, line 96
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Http\Runner::run() - CORE/src/Http/Runner.php, line 51
Cake\Http\Server::run() - CORE/src/Http/Server.php, line 98
Deprecated (16384): The ArrayAccess methods will be removed in 4.0.0.Use getParam(), getData() and getQuery() instead. - /home/brlfuser/public_html/src/Controller/ArtileDetailController.php, line: 151
You can disable deprecation warnings by setting `Error.errorLevel` to `E_ALL & ~E_USER_DEPRECATED` in your config/app.php. [CORE/src/Core/functions.php, line 311]
deprecationWarning - CORE/src/Core/functions.php, line 311
Cake\Http\ServerRequest::offsetGet() - CORE/src/Http/ServerRequest.php, line 2421
App\Controller\ArtileDetailController::index() - APP/Controller/ArtileDetailController.php, line 151
Cake\Controller\Controller::invokeAction() - CORE/src/Controller/Controller.php, line 610
Cake\Http\ActionDispatcher::_invoke() - CORE/src/Http/ActionDispatcher.php, line 120
Cake\Http\ActionDispatcher::dispatch() - CORE/src/Http/ActionDispatcher.php, line 94
Cake\Http\BaseApplication::__invoke() - CORE/src/Http/BaseApplication.php, line 235
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Routing\Middleware\RoutingMiddleware::__invoke() - CORE/src/Routing/Middleware/RoutingMiddleware.php, line 162
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Routing\Middleware\AssetMiddleware::__invoke() - CORE/src/Routing/Middleware/AssetMiddleware.php, line 97
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Error\Middleware\ErrorHandlerMiddleware::__invoke() - CORE/src/Error/Middleware/ErrorHandlerMiddleware.php, line 96
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Http\Runner::run() - CORE/src/Http/Runner.php, line 51
Cake\Http\Server::run() - CORE/src/Http/Server.php, line 98
Warning (512): Unable to emit headers. Headers sent in file=/home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php line=853 [CORE/src/Http/ResponseEmitter.php, line 48]
if (Configure::read('debug')) {
trigger_error($message, E_USER_WARNING);
} else {
$response = object(Cake\Http\Response) {
'status' => (int) 200,
'contentType' => 'text/html',
'headers' => [
'Content-Type' => [
[maximum depth reached]
]
],
'file' => null,
'fileRange' => [],
'cookies' => object(Cake\Http\Cookie\CookieCollection) {},
'cacheDirectives' => [],
'body' => '<!DOCTYPE html>
<!--[if lt IE 7 ]>
<html class="ie ie6" lang='en'> <![endif]-->
<!--[if IE 7 ]>
<html class="ie ie7" lang='en'> <![endif]-->
<!--[if IE 8 ]>
<html class="ie ie8" lang='en'> <![endif]-->
<!--[if (gte IE 9)|!(IE)]><!-->
<html lang='en'>
<!--<![endif]-->
<head><meta http-equiv="Content-Type" content="text/html; charset=utf-8">
<title>
LATEST NEWS UPDATES | 80% of medicines not covered by price control order -Rema Nagarajan </title>
<meta name="description" content="
-The Times of India
About 38 million people in India (which is more than Canada's population) fall below the poverty line every year due to healthcare expenses, of which 70% is on purchase of drugs. Yet, the much-awaited drug price control..."/>
<meta name="keywords" content="medicines,Health,Public Health"/>
<meta name="news_keywords" content="medicines,Health,Public Health">
<link rel="alternate" type="application/rss+xml" title="ROR" href="/ror.xml"/>
<link rel="alternate" type="application/rss+xml" title="RSS 2.0" href="/feeds/"/>
<link rel="stylesheet" href="/css/bootstrap.min.css?1697864993"/> <link rel="stylesheet" href="/css/style.css?v=1.1.2"/> <link rel="stylesheet" href="/css/style-inner.css?1577045210"/> <link rel="stylesheet" id="Oswald-css"
href="https://fonts.googleapis.com/css?family=Oswald%3Aregular%2C700&ver=3.8.1" type="text/css"
media="all">
<link rel="stylesheet" href="/css/jquery.modal.min.css?1578285302"/> <script src="/js/jquery-1.10.2.js?1575549704"></script> <script src="/js/jquery-migrate.min.js?1575549704"></script> <link rel="shortcut icon" href="/favicon.ico" title="Favicon">
<link rel="stylesheet" href="/css/jquery-ui.css?1580720609"/> <script src="/js/jquery-ui.js?1575549704"></script> <link rel="preload" as="style" href="https://www.im4change.org/css/custom.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery.modal.min.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery-ui.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/li-scroller.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<!-- <link rel="preload" as="style" href="https://www.im4change.org/css/style.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous"> -->
<link rel="preload" as="style" href="https://www.im4change.org/css/style-inner.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel='dns-prefetch' href="//im4change.org/css/custom.css" crossorigin >
<link rel="preload" as="script" href="https://www.im4change.org/js/bootstrap.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.li-scroller.1.0.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.modal.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.ui.totop.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-1.10.2.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-migrate.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-ui.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/setting.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/tie-scripts.js">
<!--[if IE]>
<script type="text/javascript">jQuery(document).ready(function () {
jQuery(".menu-item").has("ul").children("a").attr("aria-haspopup", "true");
});</script>
<![endif]-->
<!--[if lt IE 9]>
<script src="/js/html5.js"></script>
<script src="/js/selectivizr-min.js"></script>
<![endif]-->
<!--[if IE 8]>
<link rel="stylesheet" type="text/css" media="all" href="/css/ie8.css"/>
<![endif]-->
<meta property="og:title" content="LATEST NEWS UPDATES | 80% of medicines not covered by price control order -Rema Nagarajan" />
<meta property="og:url" content="https://im4change.in/latest-news-updates/80-of-medicines-not-covered-by-price-control-order-rema-nagarajan-23504.html" />
<meta property="og:type" content="article" />
<meta property="og:description" content="
-The Times of India
About 38 million people in India (which is more than Canada's population) fall below the poverty line every year due to healthcare expenses, of which 70% is on purchase of drugs. Yet, the much-awaited drug price control..." />
<meta property="og:image" content="" />
<meta property="fb:app_id" content="0" />
<meta name="viewport" content="width=device-width, initial-scale=1, maximum-scale=1, user-scalable=no">
<link rel="apple-touch-icon-precomposed" sizes="144x144" href="https://im4change.in/images/apple1.png">
<link rel="apple-touch-icon-precomposed" sizes="120x120" href="https://im4change.in/images/apple2.png">
<link rel="apple-touch-icon-precomposed" sizes="72x72" href="https://im4change.in/images/apple3.png">
<link rel="apple-touch-icon-precomposed" href="https://im4change.in/images/apple4.png">
<style>
.gsc-results-wrapper-overlay{
top: 38% !important;
height: 50% !important;
}
.gsc-search-button-v2{
border-color: #035588 !important;
background-color: #035588 !important;
}
.gsib_a{
height: 30px !important;
padding: 2px 8px 1px 6px !important;
}
.gsc-search-button-v2{
height: 41px !important;
}
input.gsc-input{
background: none !important;
}
@media only screen and (max-width: 600px) {
.gsc-results-wrapper-overlay{
top: 11% !important;
width: 87% !important;
left: 9% !important;
height: 43% !important;
}
.gsc-search-button-v2{
padding: 10px 10px !important;
}
.gsc-input-box{
height: 28px !important;
}
/* .gsib_a {
padding: 0px 9px 4px 9px !important;
}*/
}
@media only screen and (min-width: 1200px) and (max-width: 1920px) {
table.gsc-search-box{
width: 15% !important;
float: right !important;
margin-top: -118px !important;
}
.gsc-search-button-v2 {
padding: 6px !important;
}
}
</style>
<script>
$(function () {
$("#accordion").accordion({
event: "click hoverintent"
});
});
/*
* hoverIntent | Copyright 2011 Brian Cherne
* http://cherne.net/brian/resources/jquery.hoverIntent.html
* modified by the jQuery UI team
*/
$.event.special.hoverintent = {
setup: function () {
$(this).bind("mouseover", jQuery.event.special.hoverintent.handler);
},
teardown: function () {
$(this).unbind("mouseover", jQuery.event.special.hoverintent.handler);
},
handler: function (event) {
var currentX, currentY, timeout,
args = arguments,
target = $(event.target),
previousX = event.pageX,
previousY = event.pageY;
function track(event) {
currentX = event.pageX;
currentY = event.pageY;
}
;
function clear() {
target
.unbind("mousemove", track)
.unbind("mouseout", clear);
clearTimeout(timeout);
}
function handler() {
var prop,
orig = event;
if ((Math.abs(previousX - currentX) +
Math.abs(previousY - currentY)) < 7) {
clear();
event = $.Event("hoverintent");
for (prop in orig) {
if (!(prop in event)) {
event[prop] = orig[prop];
}
}
// Prevent accessing the original event since the new event
// is fired asynchronously and the old event is no longer
// usable (#6028)
delete event.originalEvent;
target.trigger(event);
} else {
previousX = currentX;
previousY = currentY;
timeout = setTimeout(handler, 100);
}
}
timeout = setTimeout(handler, 100);
target.bind({
mousemove: track,
mouseout: clear
});
}
};
</script>
<script type="text/javascript">
var _gaq = _gaq || [];
_gaq.push(['_setAccount', 'UA-472075-3']);
_gaq.push(['_trackPageview']);
(function () {
var ga = document.createElement('script');
ga.type = 'text/javascript';
ga.async = true;
ga.src = ('https:' == document.location.protocol ? 'https://ssl' : 'http://www') + '.google-analytics.com/ga.js';
var s = document.getElementsByTagName('script')[0];
s.parentNode.insertBefore(ga, s);
})();
</script>
<link rel="stylesheet" href="/css/custom.css?v=1.16"/> <script src="/js/jquery.ui.totop.js?1575549704"></script> <script src="/js/setting.js?1575549704"></script> <link rel="manifest" href="/manifest.json">
<meta name="theme-color" content="#616163" />
<meta name="apple-mobile-web-app-capable" content="yes">
<meta name="apple-mobile-web-app-status-bar-style" content="black">
<meta name="apple-mobile-web-app-title" content="im4change">
<link rel="apple-touch-icon" href="/icons/logo-192x192.png">
</head>
<body id="top" class="home inner blog">
<div class="background-cover"></div>
<div class="wrapper animated">
<header id="theme-header" class="header_inner" style="position: relative;">
<div class="logo inner_logo" style="left:20px !important">
<a title="Home" href="https://im4change.in/">
<img src="https://im4change.in/images/logo2.jpg?1582080632" class="logo_image" alt="im4change"/> </a>
</div>
<div class="langhindi" style="color: #000;display:none;"
href="https://im4change.in/">
<a class="more-link" href="https://im4change.in/">Home</a>
<a href="https://im4change.in/hindi/" class="langbutton ">हिन्दी</a>
</div>
<nav class="fade-in animated2" id="main-nav">
<div class="container">
<div class="main-menu">
<ul class="menu" id="menu-main">
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
style="left: -40px;"><a
target="_blank" href="https://im4change.in/">Home</a>
</li>
<li class="menu-item mega-menu menu-item-type-taxonomy mega-menu menu-item-object-category mega-menu menu-item-has-children parent-list"
style=" margin-left: -40px;"><a href="#">KNOWLEDGE GATEWAY <span class="sub-indicator"></span>
</a>
<div class="mega-menu-block background_menu" style="padding-top:25px;">
<div class="container">
<div class="mega-menu-content">
<div class="mega-menu-item">
<h3><b>Farm Crisis</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/farmers039-suicides-14.html"
class="left postionrel">Farm Suicides </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/unemployment-30.html"
class="left postionrel">Unemployment </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/rural-distress-70.html"
class="left postionrel">Rural distress </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/migration-34.html"
class="left postionrel">Migration </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/key-facts-72.html"
class="left postionrel">Key Facts </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/debt-trap-15.html"
class="left postionrel">Debt Trap </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Empowerment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/union-budget-73.html"
class="left postionrel">Union Budget And Other Economic Policies </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/forest-and-tribal-rights-61.html"
class="left postionrel">Forest and Tribal Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-education-60.html"
class="left postionrel">Right to Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-food-59.html"
class="left postionrel">Right to Food </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/displacement-3279.html"
class="left postionrel">Displacement </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-work-mg-nrega-39.html"
class="left postionrel">Right to Work (MG-NREGA) </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/gender-3280.html"
class="left postionrel">GENDER </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-information-58.html"
class="left postionrel">Right to Information </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/social-audit-48.html"
class="left postionrel">Social Audit </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Hunger / HDI</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/poverty-and-inequality-20499.html"
class="left postionrel">Poverty and inequality </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/malnutrition-41.html"
class="left postionrel">Malnutrition </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/public-health-51.html"
class="left postionrel">Public Health </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/education-50.html"
class="left postionrel">Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hunger-overview-40.html"
class="left postionrel">Hunger Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hdi-overview-45.html"
class="left postionrel">HDI Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/pds-ration-food-security-42.html"
class="left postionrel">PDS/ Ration/ Food Security </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/sdgs-113.html"
class="left postionrel">SDGs </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/mid-day-meal-scheme-mdms-53.html"
class="left postionrel">Mid Day Meal Scheme (MDMS) </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Environment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/time-bomb-ticking-52.html"
class="left postionrel">Time Bomb Ticking </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/water-and-sanitation-55.html"
class="left postionrel">Water and Sanitation </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/impact-on-agriculture-54.html"
class="left postionrel">Impact on Agriculture </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Law & Justice</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/social-justice-20500.html"
class="left postionrel">Social Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/access-to-justice-47.html"
class="left postionrel">Access to Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/human-rights-56.html"
class="left postionrel">Human Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/corruption-35.html"
class="left postionrel">Corruption </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/general-insecurity-46.html"
class="left postionrel">General Insecurity </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/disaster-relief-49.html"
class="left postionrel">Disaster & Relief </a>
</p>
</div>
</div>
</div>
</div>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page "><a target="_blank" href="https://im4change.in/nceus_reports.php">NCEUS reports</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children parent-list ">
<a target="_blank" href="https://im4change.in/about-us-9.html">About Us <span
class="sub-indicator"></span></a>
<ul class="sub-menu aboutmenu">
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/objectives-8.html">Objectives</a>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/contactus.php">Contact
Us</a></li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/about-us-9.html">About
Us</a></li>
</ul>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children ">
<a target="_blank" href="https://im4change.in/fellowships.php" title="Fellowships">Fellowships</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/media-workshops.php">Workshops</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/research.php">Research</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/links-64">Partners</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
id="menu-item-539"><a target="_blank" href="https://im4change.in/hindi/"
class="langbutton langlinkfont17">हिन्दी</a></li>
</ul>
</div> </div>
<!-- <div style="float: right;">
<script async src="https://cse.google.com/cse.js?cx=18b4f2e0f11bed3dd"></script>
<div class="gcse-search"></div>
</div> -->
<div class="search-block" style=" margin-left: 8px; margin-right: 7px;">
<form method="get" id="searchform" name="searchform"
action="https://im4change.in/search"
onsubmit="return searchvalidate();">
<button class="search-button" type="submit" value="Search"></button>
<input type="text" id="s" name="qryStr" value=""
onfocus="if (this.value == 'Search...') {this.value = '';}"
onblur="if (this.value == '') {this.value = 'Search...';}">
</form>
</div>
</nav>
</header>
<div class="container">
<div id="main-content" class=" main1 container fade-in animated3 sidebar-narrow-left">
<div class="content-wrap">
<div class="content" style="width: 900px;min-height: 500px;">
<section class="cat-box recent-box innerCatRecent">
<h1 class="cat-box-title">80% of medicines not covered by price control order -Rema Nagarajan</h1>
<a href="JavaScript:void(0);" onclick="return shareArticle(23342);">
<img src="https://im4change.in/images/email.png?1582080630" border="0" width="24" align="right" alt="Share this article"/> </a>
<a href="https://im4change.in/latest-news-updates/80-of-medicines-not-covered-by-price-control-order-rema-nagarajan-23504/print"
rel="nofollow">
<img src="https://im4change.in/images/icon-print.png?1582080630" border="0" width="24" align="right" alt="Share this article"/>
</a>
</section>
<section class="recent-box innerCatRecent">
<small class="pb-1"><span class="dateIcn">
<img src="https://im4change.in/images/published.svg?1582080666" alt="published"/>
Published on</span><span class="text-date"> Dec 1, 2013</span>
<span
class="dateIcn">
<img src="https://im4change.in/images/modified.svg?1582080666" alt="modified"/> Modified on </span><span class="text-date"> Dec 1, 2013</span>
</small>
</section>
<div class="clear"></div>
<div style="padding-top: 10px;">
<div class="innerLineHeight">
<div class="middleContent innerInput latest-news-updates">
<table>
<tr>
<td>
<div>
<div align="justify">-The Times of India</div><p align="justify"><br />About 38 million people in India (which is more than Canada's population) fall below the poverty line every year due to healthcare expenses, of which 70% is on purchase of drugs. Yet, the much-awaited drug price control order (DPCO) 2013, meant to control the price of medicines does not cover over 80% of the medicines in the market. Many drugs crucial for India's disease profile have been left out, which means people are unlikely to see any significant reduction in expenditure on medicines.</p><p align="justify"><img src="https://im4change.in/siteadmin/tinymce/uploaded/Health_1.JPG" alt="Health" width="657" height="296" /> </p><p align="justify">In 2003, the Supreme Court, while hearing a case on the National Pharmaceutical Pricing Policy, had directed the government to formulate appropriate criteria to identify essential and life saving drugs and ensure that they came under price control. It took over a decade for the government to announce the DPCO in May 2013.</p><p align="justify">By the government's own admission in an affidavit filed in court, the market value and share of medicines covered by DPCO is just 18% of the country's pharma market. Many life-saving medicines including anti-cancer drugs, expensive antibiotics and drugs needed for organ transplantation have been left out.</p><p align="justify">The government merely lifted the entire National List of Essential Medicines (NLEM) 2011, comprising 348 medicines, and placed it under price control. "The literal translation of the NLEM into DPCO 2103 has been done without a thought of its implications. The companies have been provided a convenient escape route. A 500 mg Paracetamol tablet is under price control but its 650 mg strength is not; individual anti-TB drugs are under price control but their combinations which outsell single ingredient preparations are not. This undermines the entire objective of making essential medicines more affordable to Indians," explained Dr Anurag Bhargava, associate professor at the Himalayan Institute of Medical Sciences. He stressed the need to expand the scope of price control to include all dosages and combinations, as was the case in the previous DPCO of 1995.</p><p align="justify">With the current DPCO not covering combinations of drugs, a lot of drugs for diabetes and hypertension and many other conditions will move out of price control as they are used in combination. The combinations not covered under NLEM account for Rs 31,866 crore or almost 45% of the total pharma market of Rs 71,246 crore in 2012.</p><p align="justify">An independent evaluation of the National Pharmaceutical Pricing Policy, by the Public Health Foundation of India (PHFI) and the Institute for Studies in Industrial Development (ISID) for a forthcoming report explains why it is important to expand the scope of price control. According to their evaluation, the market value of anti-infectives under price control is Rs 4,636 crore, just 6.5% of the total market. Anti-infectives, which include antibiotics, have the biggest chunk of India's pharma market.</p><p align="justify">"Our evaluation shows that if price control was expanded to combinations, additional strengths and dosages of just the anti-infectives included in the NLEM, the total market value would be worth more than Rs 10,500 crore, about 15% of the total pharma market, a vast improvement over the current coverage of just 6.5%," said Malini Aisola of PHFI.</p><p align="justify">The essential medicines list does not seem to have taken into account India's disease profile as it leaves out several drugs crucial for treating many common conditions, pointed out Dr Bhargava. The government's own affidavit admits that only 18% of anti-diabetics, 19% of anti-TB medicines and 6% of the respiratory therapeutics segment are under price control. This is despite India being the diabetes and TB capital of the world, and facing high prevalence of asthma and chronic obstructive pulmonary disease (COPD).</p><p align="justify">There's good reason why we need price controls. The MRP charged by companies is often many times the cost of production leaving them with profit margins unheard of in any other sector. Price control was meant to address this problem, particularly in medicines important for India. But it has failed to make any significant difference.</p><p align="justify">One reason is the way prices are determined under the current DPCO. Under the 1995 DPCO, the drugs prices under controls was decided by taking the cost of manufacture and fixing a certain percentage as mark-up, which included packaging and distribution costs, retailers' margin, excise duty and profit. But the current DPCO uses a new formula under which the price is fixed by taking the average price of brands having one per cent or more of market share and adding 16% as retail margin.</p><p align="justify">S Srinivasan of LOCOST, a company producing drugs for use by NGOs to treat the poor, explained how the cost of manufacture, including retail margin, for Cetrizine, an anti-allergic, is just Rs 1.20 for ten tablets. The ceiling price under the DPCO is Rs 18.10, the same as the price charged by the market leader GSK. This allows a price that is 15 times the cost of manufacture. In the case of Albendazole, a drug used to treat worm infections, the cost of manufacture including retail margin is Rs 8.50 per 10 tablets, while the DPCO ceiling price is over Rs 91, a ten-fold mark-up, pointed out Srinivasan. The price charged by the market leader in Albendazole, GSK, was Rs 140 per ten tablets. In this case, while price control should bring down the market leader's price, it still allows a huge profit margin. In fact, the PHFI-ISID evaluation shows that in 43% of drugs studied, the sales leader will face little or no impact from price control.</p><p align="justify">To show how effective DPCO has been, the government has compared the price reductions due to DPCO with the highest price of a drug. However, PHFI and ISID point out, it makes more sense to use the price charged by the company with the highest market share for comparison. Out of the 390 formulations for which prices have been notified, in 212 the company with the highest sales does not have the highest price. So, the price reduction achieved by DPCO is nowhere as dramatic as claimed by the government. PHFI and ISID have conducted an independent analysis using the same data as used by the government. Their calculation for 369 formulations shows that the effective average price reduction would be just 11% and the impact on the pharma market as a whole would be a mere 1.8%.</p><p align="justify">In sum, coming in 2013, a decade after the Supreme Court asked for it, the DPCO is clearly late. But even worse, as the PHFI-ISID study reveals, it is too little. Given how much rides on this for the aam aadmi, that is a tragedy of mammoth proportions.About 38 million people in India (which is more than Canada's population) fall below the poverty line every year due to healthcare expenses, of which 70% is on purchase of drugs. Yet, the much-awaited drug price control order (DPCO) 2013, meant to control the price of medicines does not cover over 80% of the medicines in the market. Many drugs crucial for India's disease profile have been left out, which means people are unlikely to see any significant reduction in expenditure on medicines.</p><p align="justify">In 2003, the Supreme Court, while hearing a case on the National Pharmaceutical Pricing Policy, had directed the government to formulate appropriate criteria to identify essential and life saving drugs and ensure that they came under price control. It took over a decade for the government to announce the DPCO in May 2013.</p><p align="justify">By the government's own admission in an affidavit filed in court, the market value and share of medicines covered by DPCO is just 18% of the country's pharma market. Many life-saving medicines including anti-cancer drugs, expensive antibiotics and drugs needed for organ transplantation have been left out.</p><p align="justify">The government merely lifted the entire National List of Essential Medicines (NLEM) 2011, comprising 348 medicines, and placed it under price control. "The literal translation of the NLEM into DPCO 2103 has been done without a thought of its implications. The companies have been provided a convenient escape route. A 500 mg Paracetamol tablet is under price control but its 650 mg strength is not; individual anti-TB drugs are under price control but their combinations which outsell single ingredient preparations are not. This undermines the entire objective of making essential medicines more affordable to Indians," explained Dr Anurag Bhargava, associate professor at the Himalayan Institute of Medical Sciences. He stressed the need to expand the scope of price control to include all dosages and combinations, as was the case in the previous DPCO of 1995.</p><p align="justify">With the current DPCO not covering combinations of drugs, a lot of drugs for diabetes and hypertension and many other conditions will move out of price control as they are used in combination. The combinations not covered under NLEM account for Rs 31,866 crore or almost 45% of the total pharma market of Rs 71,246 crore in 2012.</p><p align="justify">An independent evaluation of the National Pharmaceutical Pricing Policy, by the Public Health Foundation of India (PHFI) and the Institute for Studies in Industrial Development (ISID) for a forthcoming report explains why it is important to expand the scope of price control. According to their evaluation, the market value of anti-infectives under price control is Rs 4,636 crore, just 6.5% of the total market. Anti-infectives, which include antibiotics, have the biggest chunk of India's pharma market.</p><p align="justify">"Our evaluation shows that if price control was expanded to combinations, additional strengths and dosages of just the anti-infectives included in the NLEM, the total market value would be worth more than Rs 10,500 crore, about 15% of the total pharma market, a vast improvement over the current coverage of just 6.5%," said Malini Aisola of PHFI.</p><p align="justify">The essential medicines list does not seem to have taken into account India's disease profile as it leaves out several drugs crucial for treating many common conditions, pointed out Dr Bhargava. The government's own affidavit admits that only 18% of anti-diabetics, 19% of anti-TB medicines and 6% of the respiratory therapeutics segment are under price control. This is despite India being the diabetes and TB capital of the world, and facing high prevalence of asthma and chronic obstructive pulmonary disease (COPD).</p><p align="justify">There's good reason why we need price controls. The MRP charged by companies is often many times the cost of production leaving them with profit margins unheard of in any other sector. Price control was meant to address this problem, particularly in medicines important for India. But it has failed to make any significant difference.</p><p align="justify">One reason is the way prices are determined under the current DPCO. Under the 1995 DPCO, the drugs prices under controls was decided by taking the cost of manufacture and fixing a certain percentage as mark-up, which included packaging and distribution costs, retailers' margin, excise duty and profit. But the current DPCO uses a new formula under which the price is fixed by taking the average price of brands having one per cent or more of market share and adding 16% as retail margin.</p><p align="justify">S Srinivasan of LOCOST, a company producing drugs for use by NGOs to treat the poor, explained how the cost of manufacture, including retail margin, for Cetrizine, an anti-allergic, is just Rs 1.20 for ten tablets. The ceiling price under the DPCO is Rs 18.10, the same as the price charged by the market leader GSK. This allows a price that is 15 times the cost of manufacture. In the case of Albendazole, a drug used to treat worm infections, the cost of manufacture including retail margin is Rs 8.50 per 10 tablets, while the DPCO ceiling price is over Rs 91, a ten-fold mark-up, pointed out Srinivasan. The price charged by the market leader in Albendazole, GSK, was Rs 140 per ten tablets. In this case, while price control should bring down the market leader's price, it still allows a huge profit margin. In fact, the PHFI-ISID evaluation shows that in 43% of drugs studied, the sales leader will face little or no impact from price control.</p><p align="justify">To show how effective DPCO has been, the government has compared the price reductions due to DPCO with the highest price of a drug. However, PHFI and ISID point out, it makes more sense to use the price charged by the company with the highest market share for comparison. Out of the 390 formulations for which prices have been notified, in 212 the company with the highest sales does not have the highest price. So, the price reduction achieved by DPCO is nowhere as dramatic as claimed by the government. PHFI and ISID have conducted an independent analysis using the same data as used by the government. Their calculation for 369 formulations shows that the effective average price reduction would be just 11% and the impact on the pharma market as a whole would be a mere 1.8%.</p><p align="justify">In sum, coming in 2013, a decade after the Supreme Court asked for it, the DPCO is clearly late. But even worse, as the PHFI-ISID study reveals, it is too little. Given how much rides on this for the aam aadmi, that is a tragedy of mammoth proportions.</p>
</div>
</td>
</tr>
</table>
</div>
</div>
</div>
<div class="clear"></div>
<br><a href="http://timesofindia.indiatimes.com/india/80-of-medicines-not-covered-by-price-control-order/articleshow/26678324.cms" class="re" target="_blank">The Times of India, 1 December, 2013, http://timesofindia.indiatimes.com/india/80-of-medicines-not-covered-by-price-control-order/articleshow/26678324.cms</a><div class="clear"></div>
<div style="padding-top: 18px;">
<p class="post-tag">Tagged with:
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=medicines"
title="medicines">
medicines </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Health"
title="Health">
Health </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Public Health"
title="Public Health">
Public Health </a>
</p>
</div>
<div class="clear"></div>
<br><br>
<div class="widget-top">
<h4>Related Articles</h4>
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<ul id="recentcomments">
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/fifth-report-from-gambia-implicates-indian-drug-maker-for-contaminated-syrups-banjot-kaur.html"
title="Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur">
Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-may-have-seen-steepest-dip-in-multidimensional-poverty-among-110-nations-as-per-undp-data-nikhil-rampal.html"
title="India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal">
India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/health-among-top-three-priorities-for-indian-voters-after-jobs-and-education-survey-shows-oliver-heath-jyoti-mishra-louise-tillin-sandhya-venkateswaran.html"
title="Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran">
Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/prevalence-of-zero-food-among-infants-and-young-children-in-india-patterns-of-change-across-the-states-and-union-territories-of-india-1993-2021-the-lancet.html"
title="Prevalence of Zero-Food among infants and young children in India - The Lancet ">
Prevalence of Zero-Food among infants and young children in India - The Lancet </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-s-sustainability-goals-at-risk-because-of-extreme-heatwaves-carbon-copy.html"
title="India's Sustainability Goals at Risk Because of Extreme Heatwaves - Carbon Copy">
India's Sustainability Goals at Risk Because of Extreme Heatwaves - Carbon Copy </a>
</li>
</ul>
</div>
<div class="comment-respond" id="respond">
<a name="commentbox"> </a>
<h3 class="comment-reply-title" id="reply-title">Write Comments</h3>
<form method="post" accept-charset="utf-8" role="form" action="/latest-news-updates/80-of-medicines-not-covered-by-price-control-order-rema-nagarajan-23504.html"><div style="display:none;"><input type="hidden" name="_method" value="POST"/></div> <form class="comment-form" id="commentform" method="post" action="#commentbox" onSubmit="return validate()"
name="cmtform">
<input type="hidden" name="cmttype" value="articlecmt"/>
<input type="hidden" name="article_id" value="23342"/>
<p class="comment-notes">Your email address will not be published. Required fields are marked <span
class="required">*</span></p>
<p class="comment-form-author">
<label for="commenterName">Name</label>
<span class="required">*</span>
<input type="text" aria-required="true" size="30"
value=""
name="commenterName" id="commenterName" required="true">
</p>
<p class="comment-form-email">
<label for="commenterEmail">Email</label> <span class="required">*</span>
<input aria-required="true" size="30" name="commenterEmail" id="commenterEmail" type="email"
value=""
required="true">
</p>
<p class="comment-form-contact">
<label for="commenterPh">Contact No.</label>
<input type="text" size="30"
value=""
name="commenterPh" id="commenterPh">
</p>
<p class="comment-form-comment">
<label for="comment">Comment</label>
<textarea aria-required="true" required="true" rows="8" cols="45" name="comment"
id="comment"></textarea>
</p>
<p class="comment-form-comment">
<label for="comment">Type the characters you see in the image below <span class="required">*</span><br><img
class="captchaImg"
src="https://im4change.in/securimage_show_art.php?tk=1865397053" alt="captcha"/>
</label>
</p>
<input type="text" name="vrcode" required="true"/>
<p class="form-submit" style="width: 200px;">
<input type="submit" value="Post Comment" id="submit" name="submit">
</p></form>
</div>
<style>
.ui-widget-content {
height: auto !important;
}
</style>
<div id="share-modal"></div>
<style>
.middleContent a{
background-color: rgba(108,172,228,.2);
}
.middleContent a:hover{
background-color: #418fde;
border-color: #418fde;
color: #000;
}
</style>
<script>
function shareArticle(article_id) {
var options = {
modal: true,
height: 'auto',
width: 600 + 'px'
};
$('#share-modal').html("");
$('#share-modal').load('https://im4change.in/share_article?article_id=' + article_id).dialog(options).dialog('open');
}
function postShare() {
var param = 'article_id=' + $("#article_id").val();
param = param + '&y_name=' + $("#y_name").val();
param = param + '&y_email=' + $("#y_email").val();
param = param + '&f_name=' + $("#f_name").val();
param = param + '&f_email=' + $("#f_email").val();
param = param + '&y_msg=' + $("#y_msg").val();
$.ajax({
type: "POST",
url: 'https://im4change.in/post_share_article',
data: param,
success: function (response) {
$('#share-modal').html("Thank You, Your message posted to ");
}
});
return false;
}
</script> </div>
</div>
<!-- Right Side Section Start -->
<!-- MAP Section START -->
<aside class="sidebar indexMarg">
<div class="ad-cell">
<a href="https://im4change.in/statemap.php" title="">
<img src="https://im4change.in/images/map_new_version.png?1582080666" alt="India State Map" class="indiamap" width="232" height="252"/> </a>
<div class="rightmapbox">
<div id="sideOne" class="docltitle"><a href="https://im4change.in/state-report/india/36" target="_blank">DOCUMENTS/
REPORTS</a></div>
<div id="sideTwo" class="statetitle"><a href="https://im4change.in/states.php"target="_blank">STATE DATA/
HDRs.</a></div>
</div>
<div class="widget widgePadTop"></div>
</div>
</aside>
<!-- MAP Section END -->
<aside class="sidebar sidePadbottom">
<div class="rightsmlbox1" >
<a href="https://im4change.in/knowledge_gateway" target="_blank" style="color: #035588;
font-size: 17px;">
KNOWLEDGE GATEWAY
</a>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/newsletter" target="_blank">
NEWSLETTER
</a>
</p>
</div>
</div>
<div class="rightsmlbox1" style="height: 325px;">
<div>
<p class="rightsmlbox1_title">
Interview with Prof. Ravi Srivastava
</p>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/video/interview-with-prof-ravi-srivastava-on-current-economic-crisis">
<img width="250" height="200" src="/images/interview_video_home.jpg" alt="Interview with Prof. Ravi Srivastava"/>
</a>
<!--
<iframe width="250" height="200" src="https://www.youtube.com/embed/MmaTlntk-wc" frameborder="0" allow="accelerometer; autoplay; encrypted-media; gyroscope; picture-in-picture" allowfullscreen=""></iframe>-->
</p>
<a href="https://im4change.in/videogallery" class="more-link CatArchalAnch1" target="_blank">
More videos
</a>
</div>
</div>
<div class="rightsmlbox1">
<div>
<!--div id="sstory" class="rightboxicons"></div--->
<p class="rightsmlbox1_title"><a href="https://im4change.in/list-success-stories" target="_blank">Success Stories</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/interviews" target="_blank">Interviews</a>
</p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a href="https://www.commoncause.in/page.php?id=10" >Donate</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/marquee"
class="isf_link more-link" title="India Focus?" style="border: 4px solid #fdd922;width: 90%;background-color: #fdd922;text-align: center;color: #000000;font-size:18px" target="_blank">India Focus</a></p> </div>
</div>
<div class="rightsmlbox1" style="height: 104px !important;">
<a href="https://im4change.in/quarterly_reports.php" target="_blank">
Quarterly Reports on Effect of Economic Slowdown on Employment in India (2008 - 2015)
</a>
</div>
<!-- <div class="rightsmlbox1">
<a href="https://play.google.com/store/apps/details?id=com.im4.im4change" target="_blank">
</a></div> -->
<!-- <section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">Most Visited</h2>
</section> -->
<!-- accordion Starts here -->
<!-- <div id="accordion" class="accordMarg">
</div> -->
<!-- accordion ends here -->
<!-- Widget Tag Cloud Starts here -->
<div id="tag_cloud-2" class="widget widget_tag_cloud">
<section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">MOST VISITED TAGS</h2>
</section>
<div class="widget-top wiPdTp">
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<div class="tagcloud">
<a href="https://im4change.in/search?qryStr=Agriculture"
target="_blank" class="tag-link-4 font4">Agriculture</a>
<a href="https://im4change.in/search?qryStr=Food Security"
target="_blank" class="tag-link-4 font4">Food Security</a>
<a href="https://im4change.in/search?qryStr=Law and Justice"
target="_blank" class="tag-link-4 font4">Law and Justice</a>
<a href="https://im4change.in/search?qryStr=Health"
target="_blank" class="tag-link-4 font4">Health</a>
<a href="https://im4change.in/search?qryStr=Right to Food"
target="_blank" class="tag-link-4 font4">Right to Food</a>
<a href="https://im4change.in/search?qryStr=Corruption"
target="_blank" class="tag-link-4 font4">Corruption</a>
<a href="https://im4change.in/search?qryStr=farming"
target="_blank" class="tag-link-4 font4">farming</a>
<a href="https://im4change.in/search?qryStr=Environment"
target="_blank" class="tag-link-4 font4">Environment</a>
<a href="https://im4change.in/search?qryStr=Right to Information"
target="_blank" class="tag-link-4 font4">Right to Information</a>
<a href="https://im4change.in/search?qryStr=NREGS"
target="_blank" class="tag-link-4 font4">NREGS</a>
<a href="https://im4change.in/search?qryStr=Human Rights"
target="_blank" class="tag-link-4 font4">Human Rights</a>
<a href="https://im4change.in/search?qryStr=Governance"
target="_blank" class="tag-link-4 font4">Governance</a>
<a href="https://im4change.in/search?qryStr=PDS"
target="_blank" class="tag-link-4 font4">PDS</a>
<a href="https://im4change.in/search?qryStr=COVID-19"
target="_blank" class="tag-link-4 font4">COVID-19</a>
<a href="https://im4change.in/search?qryStr=Land Acquisition"
target="_blank" class="tag-link-4 font4">Land Acquisition</a>
<a href="https://im4change.in/search?qryStr=mgnrega"
target="_blank" class="tag-link-4 font4">mgnrega</a>
<a href="https://im4change.in/search?qryStr=Farmers"
target="_blank" class="tag-link-4 font4">Farmers</a>
<a href="https://im4change.in/search?qryStr=transparency"
target="_blank" class="tag-link-4 font4">transparency</a>
<a href="https://im4change.in/search?qryStr=Gender"
target="_blank" class="tag-link-4 font4">Gender</a>
<a href="https://im4change.in/search?qryStr=Poverty"
target="_blank" class="tag-link-4 font4">Poverty</a>
<a href="https://im4change.in/search?qryStr=Farm Laws" target="_blank" class="tag-link-4 font4">Farm Laws
</a>
<a href="https://im4change.in/search?qryStr=Citizenship Amendment Act" target="_blank" class="tag-link-4 font4">Citizenship Amendment Act
</a>
<a href="https://im4change.in/search?qryStr=CAA NPR NRIC" target="_blank" class="tag-link-4 font4">CAA NPR NRIC
</a>
<a href="https://im4change.in/search?qryStr=Job Losses" target="_blank" class="tag-link-4 font4">Job Losses
</a>
<a href="https://im4change.in/search?qryStr=Migrant Workers" target="_blank" class="tag-link-4 font4">Migrant Workers
</a>
<a href="https://im4change.in/search?qryStr=Unemployment" target="_blank" class="tag-link-4 font4">Unemployment
</a>
<a href="https://im4change.in/search?qryStr=PMGKAY" target="_blank" class="tag-link-4 font4">PMGKAY
</a>
<a href="https://im4change.in/search?qryStr=PM-KISAN" target="_blank" class="tag-link-4 font4">PM-KISAN
</a>
<a href="https://im4change.in/search?qryStr=PM-CARES" target="_blank" class="tag-link-4 font4">PM-CARES
</a>
<a href="https://im4change.in/search?qryStr=LFPR" target="_blank" class="tag-link-4 font4">LFPR
</a>
</div>
</div>
</div>
<!-- Widget Tag Cloud Ends here -->
</aside>
<!-- Right Side Section End -->
</div>
<section class="cat-box cats-review-box footerSec">
<h2 class="cat-box-title vSec CatArcha">Video
Archives</h2>
<h2 class="cat-box-title CatArchaTitle">Archives</h2>
<div class="cat-box-content">
<div class="reviews-cat">
<div class="CatArchaDiv1">
<div class="CatArchaDiv2">
<ul>
<li>
<a href="https://im4change.in/news-alerts-57/moving-upstream-luni-fellowship.html" target="_blank">
Moving Upstream: Luni – Fellowship </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/135-million-indians-exited-multidimensional-poverty-as-per-government-figures-is-that-the-same-as-poverty-reduction.html" target="_blank">
135 Million Indians Exited “Multidimensional" Poverty as per Government... </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/explainer-why-are-tomato-prices-on-fire.html" target="_blank">
Explainer: Why are Tomato Prices on Fire? </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/nsso-survey-only-39-1-of-all-households-have-drinking-water-within-dwelling-46-7-of-rural-households-use-firewood-for-cooking.html" target="_blank">
NSSO Survey: Only 39.1% of all Households have Drinking... </a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/news-alerts-57"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/I51LYnP8BOk/1.jpg"
alt=" Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Short-Video-on-im4change-Hindi-website-Inclusive-Media-for-Change" target="_blank">
Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/kNqha-SwfIY/1.jpg"
alt=" "Session 1: Scope of IDEA and AgriStack" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-1- Scope-of-IDEA-and-AgriStack-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 1: Scope of IDEA and AgriStack" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/6kIVjlgZItk/1.jpg"
alt=" "Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-2-Farmer-Centric-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/2BeHTu0y7xc/1.jpg"
alt=" "Session 3: Future of Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-3-Future-of-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 3: Future of Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="divWidth">
<ul class="divWidthMarg">
<li>
<a href="https://im4change.in/video/Public-Spending-on-Agriculture-in-India-Source-Foundation-for-Agrarian-Studies"
title="Public Spending on Agriculture in India (Source: Foundation for Agrarian Studies)" target="_blank">
Public Spending on Agriculture in India (Source: Foundation for...</a>
</li>
<li>
<a href="https://im4change.in/video/Agrarian-Change-Seminar-Protests-against-the-New-Farm-Laws-in-India-by-Prof-Vikas-Rawal-JNU-Source-Journal-Of-Agrarian-Change"
title="Agrarian Change Seminar: 'Protests against the New Farm Laws in India' by Prof. Vikas Rawal, JNU (Source: Journal Of Agrarian Change) " target="_blank">
Agrarian Change Seminar: 'Protests against the New Farm Laws...</a>
</li>
<li>
<a href="https://im4change.in/video/Webinar-Ramrao-The-Story-of-India-Farm-Crisis-Source-Azim-Premji-University"
title="Webinar: Ramrao - The Story of India's Farm Crisis (Source: Azim Premji University)" target="_blank">
Webinar: Ramrao - The Story of India's Farm Crisis...</a>
</li>
<li>
<a href="https://im4change.in/video/water-and-agricultural-transformation-in-India"
title="Water and Agricultural Transformation in India: A Symbiotic Relationship (Source: IGIDR)" target="_blank">
Water and Agricultural Transformation in India: A Symbiotic Relationship...</a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/videogallery"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
</div>
</div>
</div>
</section> </div>
<div class="clear"></div>
<!-- Footer option Starts here -->
<div class="footer-bottom fade-in animated4">
<div class="container">
<div class="social-icons icon_flat">
<p class="SocialMargTop"> Website Developed by <a target="_blank" title="Web Development"
class="wot right"
href="http://www.ravinderkhurana.com/" rel="nofollow">
RAVINDErkHURANA.com</a></p>
</div>
<div class="alignleft">
<a
target="_blank" href="https://im4change.in/objectives-8.html"
class="link"
title="Objectives">Objectives</a> | <a
target="_blank" href="https://im4change.in/about-us-9.html"
class="link" title="About Us">About Us</a> | <a
target="_blank" href="https://im4change.in/media-workshops.php"
class="ucwords">Workshops</a> | <a
target="_blank" href="https://im4change.in/disclaimer/disclaimer-149.html"
title="Disclaimer">Disclaimer</a> </div>
</div>
</div>
<!-- Footer option ends here -->
</div>
<div id="connect">
<a target="_blank"
href="http://www.facebook.com/sharer.php?u=https://im4change.in/latest-news-updates/80-of-medicines-not-covered-by-price-control-order-rema-nagarajan-23504.html"
title="Share on Facebook">
<img src="https://im4change.in/images/Facebook.png?1582080640" alt="share on Facebook" class="ImgBorder"/>
</a><br/>
<a target="_blank"
href="http://twitter.com/share?text=Im4change&url=https://im4change.in/latest-news-updates/80-of-medicines-not-covered-by-price-control-order-rema-nagarajan-23504.html"
title="Share on Twitter">
<img src="https://im4change.in/images/twitter.png?1582080632" alt="Twitter" class="ImgBorder"/> </a>
<br/>
<a href="/feeds" title="RSS Feed" target="_blank">
<img src="https://im4change.in/images/rss.png?1582080632" alt="RSS" class="ImgBorder"/>
</a>
<br/>
<a class="feedback-link" id="feedbackFormLink" href="#">
<img src="https://im4change.in/images/feedback.png?1582080630" alt="Feedback" class="ImgBorder"/>
</a> <br/>
<a href="javascript:function iprl5(){var d=document,z=d.createElement('scr'+'ipt'),b=d.body,l=d.location;try{if(!b)throw(0);d.title='(Saving...) '+d.title;z.setAttribute('src',l.protocol+'//www.instapaper.com/j/WKrH3R7ORD5p?u='+encodeURIComponent(l.href)+'&t='+(new Date().getTime()));b.appendChild(z);}catch(e){alert('Please wait until the page has loaded.');}}iprl5();void(0)"
class="bookmarklet" onclick="return explain_bookmarklet();">
<img src="https://im4change.in/images/read-it-later.png?1582080632" alt="Read Later" class="ImgBorder"/> </a>
</div>
<!-- Feedback form Starts here -->
<div id="feedbackForm" class="overlay_form" class="ImgBorder">
<h2>Contact Form</h2>
<div id="contactform1">
<div id="formleft">
<form id="submitform" action="/contactus.php" method="post">
<input type="hidden" name="submitform" value="submitform"/>
<input type="hidden" name="salt_key" value="a0e0f2c6a0644a70e57ad2c96829709a"/>
<input type="hidden" name="ref" value="feedback"/>
<fieldset>
<label>Name :</label>
<input type="text" name="name" class="tbox" required/>
</fieldset>
<fieldset>
<label>Email :</label>
<input type="text" name="email" class="tbox" required/>
</fieldset>
<fieldset>
<label>Message :</label>
<textarea rows="5" cols="20" name="message" required></textarea>
</fieldset>
<fieldset>
Please enter security code
<div class="clear"></div>
<input type="text" name="vrcode" class="tbox"/>
</fieldset>
<fieldset>
<input type="submit" class="button" value="Submit"/>
<a href="#" id="closefeedbakcformLink">Close</a>
</fieldset>
</form>
</div>
<div class="clearfix"></div>
</div>
</div>
<div id="donate_popup" class="modal" style="max-width: 800px;">
<table width="100%" border="1">
<tr>
<td colspan="2" align="center">
<b>Support im4change</b>
</td>
</tr>
<tr>
<td width="25%" valign="middle">
<img src="https://im4change.in/images/logo2.jpg?1582080632" alt="" width="100%"/> </td>
<td style="padding-left:10px;padding-top:10px;">
<form action="https://im4change.in/donate" method="get">
<table width="100%" cellpadding="2" cellspacing="2">
<tr>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
10
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
100
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
1000
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
50
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
500
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
<input type="text" name="price" placeholder="?" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td colspan="3" align="right">
<input type="button" name="Pay" value="Pay"
style="width: 200px;background-color: rgb(205, 35, 36);color: #ffffff;"/>
</td>
</tr>
</table>
</form>
</td>
</tr>
</table>
</div><script type='text/javascript'>
/* <![CDATA[ */
var tievar = {'go_to': 'Go to...'};
/* ]]> */
</script>
<script src="/js/tie-scripts.js?1575549704"></script><script src="/js/bootstrap.js?1575549704"></script><script src="/js/jquery.modal.min.js?1578284310"></script><script>
$(document).ready(function() {
// tell the autocomplete function to get its data from our php script
$('#s').autocomplete({
source: "/autocomplete"
});
});
</script>
<script src="/vj-main-sw-register.js" async></script>
<script>function init(){var imgDefer=document.getElementsByTagName('img');for(var i=0;i<imgDefer.length;i++){if(imgDefer[i].getAttribute('data-src')){imgDefer[i].setAttribute('src',imgDefer[i].getAttribute('data-src'))}}}
window.onload=init;</script>
</body>
</html>'
}
$maxBufferLength = (int) 8192
$file = '/home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php'
$line = (int) 853
$message = 'Unable to emit headers. Headers sent in file=/home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php line=853'
Cake\Http\ResponseEmitter::emit() - CORE/src/Http/ResponseEmitter.php, line 48
Cake\Http\Server::emit() - CORE/src/Http/Server.php, line 141
[main] - ROOT/webroot/index.php, line 39
Warning (2): Cannot modify header information - headers already sent by (output started at /home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php:853) [CORE/src/Http/ResponseEmitter.php, line 148]
$response = object(Cake\Http\Response) {
'status' => (int) 200,
'contentType' => 'text/html',
'headers' => [
'Content-Type' => [
[maximum depth reached]
]
],
'file' => null,
'fileRange' => [],
'cookies' => object(Cake\Http\Cookie\CookieCollection) {},
'cacheDirectives' => [],
'body' => '<!DOCTYPE html>
<!--[if lt IE 7 ]>
<html class="ie ie6" lang='en'> <![endif]-->
<!--[if IE 7 ]>
<html class="ie ie7" lang='en'> <![endif]-->
<!--[if IE 8 ]>
<html class="ie ie8" lang='en'> <![endif]-->
<!--[if (gte IE 9)|!(IE)]><!-->
<html lang='en'>
<!--<![endif]-->
<head><meta http-equiv="Content-Type" content="text/html; charset=utf-8">
<title>
LATEST NEWS UPDATES | 80% of medicines not covered by price control order -Rema Nagarajan </title>
<meta name="description" content="
-The Times of India
About 38 million people in India (which is more than Canada's population) fall below the poverty line every year due to healthcare expenses, of which 70% is on purchase of drugs. Yet, the much-awaited drug price control..."/>
<meta name="keywords" content="medicines,Health,Public Health"/>
<meta name="news_keywords" content="medicines,Health,Public Health">
<link rel="alternate" type="application/rss+xml" title="ROR" href="/ror.xml"/>
<link rel="alternate" type="application/rss+xml" title="RSS 2.0" href="/feeds/"/>
<link rel="stylesheet" href="/css/bootstrap.min.css?1697864993"/> <link rel="stylesheet" href="/css/style.css?v=1.1.2"/> <link rel="stylesheet" href="/css/style-inner.css?1577045210"/> <link rel="stylesheet" id="Oswald-css"
href="https://fonts.googleapis.com/css?family=Oswald%3Aregular%2C700&ver=3.8.1" type="text/css"
media="all">
<link rel="stylesheet" href="/css/jquery.modal.min.css?1578285302"/> <script src="/js/jquery-1.10.2.js?1575549704"></script> <script src="/js/jquery-migrate.min.js?1575549704"></script> <link rel="shortcut icon" href="/favicon.ico" title="Favicon">
<link rel="stylesheet" href="/css/jquery-ui.css?1580720609"/> <script src="/js/jquery-ui.js?1575549704"></script> <link rel="preload" as="style" href="https://www.im4change.org/css/custom.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery.modal.min.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery-ui.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/li-scroller.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<!-- <link rel="preload" as="style" href="https://www.im4change.org/css/style.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous"> -->
<link rel="preload" as="style" href="https://www.im4change.org/css/style-inner.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel='dns-prefetch' href="//im4change.org/css/custom.css" crossorigin >
<link rel="preload" as="script" href="https://www.im4change.org/js/bootstrap.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.li-scroller.1.0.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.modal.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.ui.totop.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-1.10.2.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-migrate.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-ui.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/setting.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/tie-scripts.js">
<!--[if IE]>
<script type="text/javascript">jQuery(document).ready(function () {
jQuery(".menu-item").has("ul").children("a").attr("aria-haspopup", "true");
});</script>
<![endif]-->
<!--[if lt IE 9]>
<script src="/js/html5.js"></script>
<script src="/js/selectivizr-min.js"></script>
<![endif]-->
<!--[if IE 8]>
<link rel="stylesheet" type="text/css" media="all" href="/css/ie8.css"/>
<![endif]-->
<meta property="og:title" content="LATEST NEWS UPDATES | 80% of medicines not covered by price control order -Rema Nagarajan" />
<meta property="og:url" content="https://im4change.in/latest-news-updates/80-of-medicines-not-covered-by-price-control-order-rema-nagarajan-23504.html" />
<meta property="og:type" content="article" />
<meta property="og:description" content="
-The Times of India
About 38 million people in India (which is more than Canada's population) fall below the poverty line every year due to healthcare expenses, of which 70% is on purchase of drugs. Yet, the much-awaited drug price control..." />
<meta property="og:image" content="" />
<meta property="fb:app_id" content="0" />
<meta name="viewport" content="width=device-width, initial-scale=1, maximum-scale=1, user-scalable=no">
<link rel="apple-touch-icon-precomposed" sizes="144x144" href="https://im4change.in/images/apple1.png">
<link rel="apple-touch-icon-precomposed" sizes="120x120" href="https://im4change.in/images/apple2.png">
<link rel="apple-touch-icon-precomposed" sizes="72x72" href="https://im4change.in/images/apple3.png">
<link rel="apple-touch-icon-precomposed" href="https://im4change.in/images/apple4.png">
<style>
.gsc-results-wrapper-overlay{
top: 38% !important;
height: 50% !important;
}
.gsc-search-button-v2{
border-color: #035588 !important;
background-color: #035588 !important;
}
.gsib_a{
height: 30px !important;
padding: 2px 8px 1px 6px !important;
}
.gsc-search-button-v2{
height: 41px !important;
}
input.gsc-input{
background: none !important;
}
@media only screen and (max-width: 600px) {
.gsc-results-wrapper-overlay{
top: 11% !important;
width: 87% !important;
left: 9% !important;
height: 43% !important;
}
.gsc-search-button-v2{
padding: 10px 10px !important;
}
.gsc-input-box{
height: 28px !important;
}
/* .gsib_a {
padding: 0px 9px 4px 9px !important;
}*/
}
@media only screen and (min-width: 1200px) and (max-width: 1920px) {
table.gsc-search-box{
width: 15% !important;
float: right !important;
margin-top: -118px !important;
}
.gsc-search-button-v2 {
padding: 6px !important;
}
}
</style>
<script>
$(function () {
$("#accordion").accordion({
event: "click hoverintent"
});
});
/*
* hoverIntent | Copyright 2011 Brian Cherne
* http://cherne.net/brian/resources/jquery.hoverIntent.html
* modified by the jQuery UI team
*/
$.event.special.hoverintent = {
setup: function () {
$(this).bind("mouseover", jQuery.event.special.hoverintent.handler);
},
teardown: function () {
$(this).unbind("mouseover", jQuery.event.special.hoverintent.handler);
},
handler: function (event) {
var currentX, currentY, timeout,
args = arguments,
target = $(event.target),
previousX = event.pageX,
previousY = event.pageY;
function track(event) {
currentX = event.pageX;
currentY = event.pageY;
}
;
function clear() {
target
.unbind("mousemove", track)
.unbind("mouseout", clear);
clearTimeout(timeout);
}
function handler() {
var prop,
orig = event;
if ((Math.abs(previousX - currentX) +
Math.abs(previousY - currentY)) < 7) {
clear();
event = $.Event("hoverintent");
for (prop in orig) {
if (!(prop in event)) {
event[prop] = orig[prop];
}
}
// Prevent accessing the original event since the new event
// is fired asynchronously and the old event is no longer
// usable (#6028)
delete event.originalEvent;
target.trigger(event);
} else {
previousX = currentX;
previousY = currentY;
timeout = setTimeout(handler, 100);
}
}
timeout = setTimeout(handler, 100);
target.bind({
mousemove: track,
mouseout: clear
});
}
};
</script>
<script type="text/javascript">
var _gaq = _gaq || [];
_gaq.push(['_setAccount', 'UA-472075-3']);
_gaq.push(['_trackPageview']);
(function () {
var ga = document.createElement('script');
ga.type = 'text/javascript';
ga.async = true;
ga.src = ('https:' == document.location.protocol ? 'https://ssl' : 'http://www') + '.google-analytics.com/ga.js';
var s = document.getElementsByTagName('script')[0];
s.parentNode.insertBefore(ga, s);
})();
</script>
<link rel="stylesheet" href="/css/custom.css?v=1.16"/> <script src="/js/jquery.ui.totop.js?1575549704"></script> <script src="/js/setting.js?1575549704"></script> <link rel="manifest" href="/manifest.json">
<meta name="theme-color" content="#616163" />
<meta name="apple-mobile-web-app-capable" content="yes">
<meta name="apple-mobile-web-app-status-bar-style" content="black">
<meta name="apple-mobile-web-app-title" content="im4change">
<link rel="apple-touch-icon" href="/icons/logo-192x192.png">
</head>
<body id="top" class="home inner blog">
<div class="background-cover"></div>
<div class="wrapper animated">
<header id="theme-header" class="header_inner" style="position: relative;">
<div class="logo inner_logo" style="left:20px !important">
<a title="Home" href="https://im4change.in/">
<img src="https://im4change.in/images/logo2.jpg?1582080632" class="logo_image" alt="im4change"/> </a>
</div>
<div class="langhindi" style="color: #000;display:none;"
href="https://im4change.in/">
<a class="more-link" href="https://im4change.in/">Home</a>
<a href="https://im4change.in/hindi/" class="langbutton ">हिन्दी</a>
</div>
<nav class="fade-in animated2" id="main-nav">
<div class="container">
<div class="main-menu">
<ul class="menu" id="menu-main">
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
style="left: -40px;"><a
target="_blank" href="https://im4change.in/">Home</a>
</li>
<li class="menu-item mega-menu menu-item-type-taxonomy mega-menu menu-item-object-category mega-menu menu-item-has-children parent-list"
style=" margin-left: -40px;"><a href="#">KNOWLEDGE GATEWAY <span class="sub-indicator"></span>
</a>
<div class="mega-menu-block background_menu" style="padding-top:25px;">
<div class="container">
<div class="mega-menu-content">
<div class="mega-menu-item">
<h3><b>Farm Crisis</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/farmers039-suicides-14.html"
class="left postionrel">Farm Suicides </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/unemployment-30.html"
class="left postionrel">Unemployment </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/rural-distress-70.html"
class="left postionrel">Rural distress </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/migration-34.html"
class="left postionrel">Migration </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/key-facts-72.html"
class="left postionrel">Key Facts </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/debt-trap-15.html"
class="left postionrel">Debt Trap </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Empowerment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/union-budget-73.html"
class="left postionrel">Union Budget And Other Economic Policies </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/forest-and-tribal-rights-61.html"
class="left postionrel">Forest and Tribal Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-education-60.html"
class="left postionrel">Right to Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-food-59.html"
class="left postionrel">Right to Food </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/displacement-3279.html"
class="left postionrel">Displacement </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-work-mg-nrega-39.html"
class="left postionrel">Right to Work (MG-NREGA) </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/gender-3280.html"
class="left postionrel">GENDER </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-information-58.html"
class="left postionrel">Right to Information </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/social-audit-48.html"
class="left postionrel">Social Audit </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Hunger / HDI</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/poverty-and-inequality-20499.html"
class="left postionrel">Poverty and inequality </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/malnutrition-41.html"
class="left postionrel">Malnutrition </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/public-health-51.html"
class="left postionrel">Public Health </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/education-50.html"
class="left postionrel">Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hunger-overview-40.html"
class="left postionrel">Hunger Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hdi-overview-45.html"
class="left postionrel">HDI Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/pds-ration-food-security-42.html"
class="left postionrel">PDS/ Ration/ Food Security </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/sdgs-113.html"
class="left postionrel">SDGs </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/mid-day-meal-scheme-mdms-53.html"
class="left postionrel">Mid Day Meal Scheme (MDMS) </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Environment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/time-bomb-ticking-52.html"
class="left postionrel">Time Bomb Ticking </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/water-and-sanitation-55.html"
class="left postionrel">Water and Sanitation </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/impact-on-agriculture-54.html"
class="left postionrel">Impact on Agriculture </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Law & Justice</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/social-justice-20500.html"
class="left postionrel">Social Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/access-to-justice-47.html"
class="left postionrel">Access to Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/human-rights-56.html"
class="left postionrel">Human Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/corruption-35.html"
class="left postionrel">Corruption </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/general-insecurity-46.html"
class="left postionrel">General Insecurity </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/disaster-relief-49.html"
class="left postionrel">Disaster & Relief </a>
</p>
</div>
</div>
</div>
</div>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page "><a target="_blank" href="https://im4change.in/nceus_reports.php">NCEUS reports</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children parent-list ">
<a target="_blank" href="https://im4change.in/about-us-9.html">About Us <span
class="sub-indicator"></span></a>
<ul class="sub-menu aboutmenu">
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/objectives-8.html">Objectives</a>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/contactus.php">Contact
Us</a></li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/about-us-9.html">About
Us</a></li>
</ul>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children ">
<a target="_blank" href="https://im4change.in/fellowships.php" title="Fellowships">Fellowships</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/media-workshops.php">Workshops</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/research.php">Research</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/links-64">Partners</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
id="menu-item-539"><a target="_blank" href="https://im4change.in/hindi/"
class="langbutton langlinkfont17">हिन्दी</a></li>
</ul>
</div> </div>
<!-- <div style="float: right;">
<script async src="https://cse.google.com/cse.js?cx=18b4f2e0f11bed3dd"></script>
<div class="gcse-search"></div>
</div> -->
<div class="search-block" style=" margin-left: 8px; margin-right: 7px;">
<form method="get" id="searchform" name="searchform"
action="https://im4change.in/search"
onsubmit="return searchvalidate();">
<button class="search-button" type="submit" value="Search"></button>
<input type="text" id="s" name="qryStr" value=""
onfocus="if (this.value == 'Search...') {this.value = '';}"
onblur="if (this.value == '') {this.value = 'Search...';}">
</form>
</div>
</nav>
</header>
<div class="container">
<div id="main-content" class=" main1 container fade-in animated3 sidebar-narrow-left">
<div class="content-wrap">
<div class="content" style="width: 900px;min-height: 500px;">
<section class="cat-box recent-box innerCatRecent">
<h1 class="cat-box-title">80% of medicines not covered by price control order -Rema Nagarajan</h1>
<a href="JavaScript:void(0);" onclick="return shareArticle(23342);">
<img src="https://im4change.in/images/email.png?1582080630" border="0" width="24" align="right" alt="Share this article"/> </a>
<a href="https://im4change.in/latest-news-updates/80-of-medicines-not-covered-by-price-control-order-rema-nagarajan-23504/print"
rel="nofollow">
<img src="https://im4change.in/images/icon-print.png?1582080630" border="0" width="24" align="right" alt="Share this article"/>
</a>
</section>
<section class="recent-box innerCatRecent">
<small class="pb-1"><span class="dateIcn">
<img src="https://im4change.in/images/published.svg?1582080666" alt="published"/>
Published on</span><span class="text-date"> Dec 1, 2013</span>
<span
class="dateIcn">
<img src="https://im4change.in/images/modified.svg?1582080666" alt="modified"/> Modified on </span><span class="text-date"> Dec 1, 2013</span>
</small>
</section>
<div class="clear"></div>
<div style="padding-top: 10px;">
<div class="innerLineHeight">
<div class="middleContent innerInput latest-news-updates">
<table>
<tr>
<td>
<div>
<div align="justify">-The Times of India</div><p align="justify"><br />About 38 million people in India (which is more than Canada's population) fall below the poverty line every year due to healthcare expenses, of which 70% is on purchase of drugs. Yet, the much-awaited drug price control order (DPCO) 2013, meant to control the price of medicines does not cover over 80% of the medicines in the market. Many drugs crucial for India's disease profile have been left out, which means people are unlikely to see any significant reduction in expenditure on medicines.</p><p align="justify"><img src="https://im4change.in/siteadmin/tinymce/uploaded/Health_1.JPG" alt="Health" width="657" height="296" /> </p><p align="justify">In 2003, the Supreme Court, while hearing a case on the National Pharmaceutical Pricing Policy, had directed the government to formulate appropriate criteria to identify essential and life saving drugs and ensure that they came under price control. It took over a decade for the government to announce the DPCO in May 2013.</p><p align="justify">By the government's own admission in an affidavit filed in court, the market value and share of medicines covered by DPCO is just 18% of the country's pharma market. Many life-saving medicines including anti-cancer drugs, expensive antibiotics and drugs needed for organ transplantation have been left out.</p><p align="justify">The government merely lifted the entire National List of Essential Medicines (NLEM) 2011, comprising 348 medicines, and placed it under price control. "The literal translation of the NLEM into DPCO 2103 has been done without a thought of its implications. The companies have been provided a convenient escape route. A 500 mg Paracetamol tablet is under price control but its 650 mg strength is not; individual anti-TB drugs are under price control but their combinations which outsell single ingredient preparations are not. This undermines the entire objective of making essential medicines more affordable to Indians," explained Dr Anurag Bhargava, associate professor at the Himalayan Institute of Medical Sciences. He stressed the need to expand the scope of price control to include all dosages and combinations, as was the case in the previous DPCO of 1995.</p><p align="justify">With the current DPCO not covering combinations of drugs, a lot of drugs for diabetes and hypertension and many other conditions will move out of price control as they are used in combination. The combinations not covered under NLEM account for Rs 31,866 crore or almost 45% of the total pharma market of Rs 71,246 crore in 2012.</p><p align="justify">An independent evaluation of the National Pharmaceutical Pricing Policy, by the Public Health Foundation of India (PHFI) and the Institute for Studies in Industrial Development (ISID) for a forthcoming report explains why it is important to expand the scope of price control. According to their evaluation, the market value of anti-infectives under price control is Rs 4,636 crore, just 6.5% of the total market. Anti-infectives, which include antibiotics, have the biggest chunk of India's pharma market.</p><p align="justify">"Our evaluation shows that if price control was expanded to combinations, additional strengths and dosages of just the anti-infectives included in the NLEM, the total market value would be worth more than Rs 10,500 crore, about 15% of the total pharma market, a vast improvement over the current coverage of just 6.5%," said Malini Aisola of PHFI.</p><p align="justify">The essential medicines list does not seem to have taken into account India's disease profile as it leaves out several drugs crucial for treating many common conditions, pointed out Dr Bhargava. The government's own affidavit admits that only 18% of anti-diabetics, 19% of anti-TB medicines and 6% of the respiratory therapeutics segment are under price control. This is despite India being the diabetes and TB capital of the world, and facing high prevalence of asthma and chronic obstructive pulmonary disease (COPD).</p><p align="justify">There's good reason why we need price controls. The MRP charged by companies is often many times the cost of production leaving them with profit margins unheard of in any other sector. Price control was meant to address this problem, particularly in medicines important for India. But it has failed to make any significant difference.</p><p align="justify">One reason is the way prices are determined under the current DPCO. Under the 1995 DPCO, the drugs prices under controls was decided by taking the cost of manufacture and fixing a certain percentage as mark-up, which included packaging and distribution costs, retailers' margin, excise duty and profit. But the current DPCO uses a new formula under which the price is fixed by taking the average price of brands having one per cent or more of market share and adding 16% as retail margin.</p><p align="justify">S Srinivasan of LOCOST, a company producing drugs for use by NGOs to treat the poor, explained how the cost of manufacture, including retail margin, for Cetrizine, an anti-allergic, is just Rs 1.20 for ten tablets. The ceiling price under the DPCO is Rs 18.10, the same as the price charged by the market leader GSK. This allows a price that is 15 times the cost of manufacture. In the case of Albendazole, a drug used to treat worm infections, the cost of manufacture including retail margin is Rs 8.50 per 10 tablets, while the DPCO ceiling price is over Rs 91, a ten-fold mark-up, pointed out Srinivasan. The price charged by the market leader in Albendazole, GSK, was Rs 140 per ten tablets. In this case, while price control should bring down the market leader's price, it still allows a huge profit margin. In fact, the PHFI-ISID evaluation shows that in 43% of drugs studied, the sales leader will face little or no impact from price control.</p><p align="justify">To show how effective DPCO has been, the government has compared the price reductions due to DPCO with the highest price of a drug. However, PHFI and ISID point out, it makes more sense to use the price charged by the company with the highest market share for comparison. Out of the 390 formulations for which prices have been notified, in 212 the company with the highest sales does not have the highest price. So, the price reduction achieved by DPCO is nowhere as dramatic as claimed by the government. PHFI and ISID have conducted an independent analysis using the same data as used by the government. Their calculation for 369 formulations shows that the effective average price reduction would be just 11% and the impact on the pharma market as a whole would be a mere 1.8%.</p><p align="justify">In sum, coming in 2013, a decade after the Supreme Court asked for it, the DPCO is clearly late. But even worse, as the PHFI-ISID study reveals, it is too little. Given how much rides on this for the aam aadmi, that is a tragedy of mammoth proportions.About 38 million people in India (which is more than Canada's population) fall below the poverty line every year due to healthcare expenses, of which 70% is on purchase of drugs. Yet, the much-awaited drug price control order (DPCO) 2013, meant to control the price of medicines does not cover over 80% of the medicines in the market. Many drugs crucial for India's disease profile have been left out, which means people are unlikely to see any significant reduction in expenditure on medicines.</p><p align="justify">In 2003, the Supreme Court, while hearing a case on the National Pharmaceutical Pricing Policy, had directed the government to formulate appropriate criteria to identify essential and life saving drugs and ensure that they came under price control. It took over a decade for the government to announce the DPCO in May 2013.</p><p align="justify">By the government's own admission in an affidavit filed in court, the market value and share of medicines covered by DPCO is just 18% of the country's pharma market. Many life-saving medicines including anti-cancer drugs, expensive antibiotics and drugs needed for organ transplantation have been left out.</p><p align="justify">The government merely lifted the entire National List of Essential Medicines (NLEM) 2011, comprising 348 medicines, and placed it under price control. "The literal translation of the NLEM into DPCO 2103 has been done without a thought of its implications. The companies have been provided a convenient escape route. A 500 mg Paracetamol tablet is under price control but its 650 mg strength is not; individual anti-TB drugs are under price control but their combinations which outsell single ingredient preparations are not. This undermines the entire objective of making essential medicines more affordable to Indians," explained Dr Anurag Bhargava, associate professor at the Himalayan Institute of Medical Sciences. He stressed the need to expand the scope of price control to include all dosages and combinations, as was the case in the previous DPCO of 1995.</p><p align="justify">With the current DPCO not covering combinations of drugs, a lot of drugs for diabetes and hypertension and many other conditions will move out of price control as they are used in combination. The combinations not covered under NLEM account for Rs 31,866 crore or almost 45% of the total pharma market of Rs 71,246 crore in 2012.</p><p align="justify">An independent evaluation of the National Pharmaceutical Pricing Policy, by the Public Health Foundation of India (PHFI) and the Institute for Studies in Industrial Development (ISID) for a forthcoming report explains why it is important to expand the scope of price control. According to their evaluation, the market value of anti-infectives under price control is Rs 4,636 crore, just 6.5% of the total market. Anti-infectives, which include antibiotics, have the biggest chunk of India's pharma market.</p><p align="justify">"Our evaluation shows that if price control was expanded to combinations, additional strengths and dosages of just the anti-infectives included in the NLEM, the total market value would be worth more than Rs 10,500 crore, about 15% of the total pharma market, a vast improvement over the current coverage of just 6.5%," said Malini Aisola of PHFI.</p><p align="justify">The essential medicines list does not seem to have taken into account India's disease profile as it leaves out several drugs crucial for treating many common conditions, pointed out Dr Bhargava. The government's own affidavit admits that only 18% of anti-diabetics, 19% of anti-TB medicines and 6% of the respiratory therapeutics segment are under price control. This is despite India being the diabetes and TB capital of the world, and facing high prevalence of asthma and chronic obstructive pulmonary disease (COPD).</p><p align="justify">There's good reason why we need price controls. The MRP charged by companies is often many times the cost of production leaving them with profit margins unheard of in any other sector. Price control was meant to address this problem, particularly in medicines important for India. But it has failed to make any significant difference.</p><p align="justify">One reason is the way prices are determined under the current DPCO. Under the 1995 DPCO, the drugs prices under controls was decided by taking the cost of manufacture and fixing a certain percentage as mark-up, which included packaging and distribution costs, retailers' margin, excise duty and profit. But the current DPCO uses a new formula under which the price is fixed by taking the average price of brands having one per cent or more of market share and adding 16% as retail margin.</p><p align="justify">S Srinivasan of LOCOST, a company producing drugs for use by NGOs to treat the poor, explained how the cost of manufacture, including retail margin, for Cetrizine, an anti-allergic, is just Rs 1.20 for ten tablets. The ceiling price under the DPCO is Rs 18.10, the same as the price charged by the market leader GSK. This allows a price that is 15 times the cost of manufacture. In the case of Albendazole, a drug used to treat worm infections, the cost of manufacture including retail margin is Rs 8.50 per 10 tablets, while the DPCO ceiling price is over Rs 91, a ten-fold mark-up, pointed out Srinivasan. The price charged by the market leader in Albendazole, GSK, was Rs 140 per ten tablets. In this case, while price control should bring down the market leader's price, it still allows a huge profit margin. In fact, the PHFI-ISID evaluation shows that in 43% of drugs studied, the sales leader will face little or no impact from price control.</p><p align="justify">To show how effective DPCO has been, the government has compared the price reductions due to DPCO with the highest price of a drug. However, PHFI and ISID point out, it makes more sense to use the price charged by the company with the highest market share for comparison. Out of the 390 formulations for which prices have been notified, in 212 the company with the highest sales does not have the highest price. So, the price reduction achieved by DPCO is nowhere as dramatic as claimed by the government. PHFI and ISID have conducted an independent analysis using the same data as used by the government. Their calculation for 369 formulations shows that the effective average price reduction would be just 11% and the impact on the pharma market as a whole would be a mere 1.8%.</p><p align="justify">In sum, coming in 2013, a decade after the Supreme Court asked for it, the DPCO is clearly late. But even worse, as the PHFI-ISID study reveals, it is too little. Given how much rides on this for the aam aadmi, that is a tragedy of mammoth proportions.</p>
</div>
</td>
</tr>
</table>
</div>
</div>
</div>
<div class="clear"></div>
<br><a href="http://timesofindia.indiatimes.com/india/80-of-medicines-not-covered-by-price-control-order/articleshow/26678324.cms" class="re" target="_blank">The Times of India, 1 December, 2013, http://timesofindia.indiatimes.com/india/80-of-medicines-not-covered-by-price-control-order/articleshow/26678324.cms</a><div class="clear"></div>
<div style="padding-top: 18px;">
<p class="post-tag">Tagged with:
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=medicines"
title="medicines">
medicines </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Health"
title="Health">
Health </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Public Health"
title="Public Health">
Public Health </a>
</p>
</div>
<div class="clear"></div>
<br><br>
<div class="widget-top">
<h4>Related Articles</h4>
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<ul id="recentcomments">
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/fifth-report-from-gambia-implicates-indian-drug-maker-for-contaminated-syrups-banjot-kaur.html"
title="Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur">
Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-may-have-seen-steepest-dip-in-multidimensional-poverty-among-110-nations-as-per-undp-data-nikhil-rampal.html"
title="India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal">
India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/health-among-top-three-priorities-for-indian-voters-after-jobs-and-education-survey-shows-oliver-heath-jyoti-mishra-louise-tillin-sandhya-venkateswaran.html"
title="Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran">
Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/prevalence-of-zero-food-among-infants-and-young-children-in-india-patterns-of-change-across-the-states-and-union-territories-of-india-1993-2021-the-lancet.html"
title="Prevalence of Zero-Food among infants and young children in India - The Lancet ">
Prevalence of Zero-Food among infants and young children in India - The Lancet </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-s-sustainability-goals-at-risk-because-of-extreme-heatwaves-carbon-copy.html"
title="India's Sustainability Goals at Risk Because of Extreme Heatwaves - Carbon Copy">
India's Sustainability Goals at Risk Because of Extreme Heatwaves - Carbon Copy </a>
</li>
</ul>
</div>
<div class="comment-respond" id="respond">
<a name="commentbox"> </a>
<h3 class="comment-reply-title" id="reply-title">Write Comments</h3>
<form method="post" accept-charset="utf-8" role="form" action="/latest-news-updates/80-of-medicines-not-covered-by-price-control-order-rema-nagarajan-23504.html"><div style="display:none;"><input type="hidden" name="_method" value="POST"/></div> <form class="comment-form" id="commentform" method="post" action="#commentbox" onSubmit="return validate()"
name="cmtform">
<input type="hidden" name="cmttype" value="articlecmt"/>
<input type="hidden" name="article_id" value="23342"/>
<p class="comment-notes">Your email address will not be published. Required fields are marked <span
class="required">*</span></p>
<p class="comment-form-author">
<label for="commenterName">Name</label>
<span class="required">*</span>
<input type="text" aria-required="true" size="30"
value=""
name="commenterName" id="commenterName" required="true">
</p>
<p class="comment-form-email">
<label for="commenterEmail">Email</label> <span class="required">*</span>
<input aria-required="true" size="30" name="commenterEmail" id="commenterEmail" type="email"
value=""
required="true">
</p>
<p class="comment-form-contact">
<label for="commenterPh">Contact No.</label>
<input type="text" size="30"
value=""
name="commenterPh" id="commenterPh">
</p>
<p class="comment-form-comment">
<label for="comment">Comment</label>
<textarea aria-required="true" required="true" rows="8" cols="45" name="comment"
id="comment"></textarea>
</p>
<p class="comment-form-comment">
<label for="comment">Type the characters you see in the image below <span class="required">*</span><br><img
class="captchaImg"
src="https://im4change.in/securimage_show_art.php?tk=1865397053" alt="captcha"/>
</label>
</p>
<input type="text" name="vrcode" required="true"/>
<p class="form-submit" style="width: 200px;">
<input type="submit" value="Post Comment" id="submit" name="submit">
</p></form>
</div>
<style>
.ui-widget-content {
height: auto !important;
}
</style>
<div id="share-modal"></div>
<style>
.middleContent a{
background-color: rgba(108,172,228,.2);
}
.middleContent a:hover{
background-color: #418fde;
border-color: #418fde;
color: #000;
}
</style>
<script>
function shareArticle(article_id) {
var options = {
modal: true,
height: 'auto',
width: 600 + 'px'
};
$('#share-modal').html("");
$('#share-modal').load('https://im4change.in/share_article?article_id=' + article_id).dialog(options).dialog('open');
}
function postShare() {
var param = 'article_id=' + $("#article_id").val();
param = param + '&y_name=' + $("#y_name").val();
param = param + '&y_email=' + $("#y_email").val();
param = param + '&f_name=' + $("#f_name").val();
param = param + '&f_email=' + $("#f_email").val();
param = param + '&y_msg=' + $("#y_msg").val();
$.ajax({
type: "POST",
url: 'https://im4change.in/post_share_article',
data: param,
success: function (response) {
$('#share-modal').html("Thank You, Your message posted to ");
}
});
return false;
}
</script> </div>
</div>
<!-- Right Side Section Start -->
<!-- MAP Section START -->
<aside class="sidebar indexMarg">
<div class="ad-cell">
<a href="https://im4change.in/statemap.php" title="">
<img src="https://im4change.in/images/map_new_version.png?1582080666" alt="India State Map" class="indiamap" width="232" height="252"/> </a>
<div class="rightmapbox">
<div id="sideOne" class="docltitle"><a href="https://im4change.in/state-report/india/36" target="_blank">DOCUMENTS/
REPORTS</a></div>
<div id="sideTwo" class="statetitle"><a href="https://im4change.in/states.php"target="_blank">STATE DATA/
HDRs.</a></div>
</div>
<div class="widget widgePadTop"></div>
</div>
</aside>
<!-- MAP Section END -->
<aside class="sidebar sidePadbottom">
<div class="rightsmlbox1" >
<a href="https://im4change.in/knowledge_gateway" target="_blank" style="color: #035588;
font-size: 17px;">
KNOWLEDGE GATEWAY
</a>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/newsletter" target="_blank">
NEWSLETTER
</a>
</p>
</div>
</div>
<div class="rightsmlbox1" style="height: 325px;">
<div>
<p class="rightsmlbox1_title">
Interview with Prof. Ravi Srivastava
</p>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/video/interview-with-prof-ravi-srivastava-on-current-economic-crisis">
<img width="250" height="200" src="/images/interview_video_home.jpg" alt="Interview with Prof. Ravi Srivastava"/>
</a>
<!--
<iframe width="250" height="200" src="https://www.youtube.com/embed/MmaTlntk-wc" frameborder="0" allow="accelerometer; autoplay; encrypted-media; gyroscope; picture-in-picture" allowfullscreen=""></iframe>-->
</p>
<a href="https://im4change.in/videogallery" class="more-link CatArchalAnch1" target="_blank">
More videos
</a>
</div>
</div>
<div class="rightsmlbox1">
<div>
<!--div id="sstory" class="rightboxicons"></div--->
<p class="rightsmlbox1_title"><a href="https://im4change.in/list-success-stories" target="_blank">Success Stories</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/interviews" target="_blank">Interviews</a>
</p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a href="https://www.commoncause.in/page.php?id=10" >Donate</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/marquee"
class="isf_link more-link" title="India Focus?" style="border: 4px solid #fdd922;width: 90%;background-color: #fdd922;text-align: center;color: #000000;font-size:18px" target="_blank">India Focus</a></p> </div>
</div>
<div class="rightsmlbox1" style="height: 104px !important;">
<a href="https://im4change.in/quarterly_reports.php" target="_blank">
Quarterly Reports on Effect of Economic Slowdown on Employment in India (2008 - 2015)
</a>
</div>
<!-- <div class="rightsmlbox1">
<a href="https://play.google.com/store/apps/details?id=com.im4.im4change" target="_blank">
</a></div> -->
<!-- <section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">Most Visited</h2>
</section> -->
<!-- accordion Starts here -->
<!-- <div id="accordion" class="accordMarg">
</div> -->
<!-- accordion ends here -->
<!-- Widget Tag Cloud Starts here -->
<div id="tag_cloud-2" class="widget widget_tag_cloud">
<section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">MOST VISITED TAGS</h2>
</section>
<div class="widget-top wiPdTp">
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<div class="tagcloud">
<a href="https://im4change.in/search?qryStr=Agriculture"
target="_blank" class="tag-link-4 font4">Agriculture</a>
<a href="https://im4change.in/search?qryStr=Food Security"
target="_blank" class="tag-link-4 font4">Food Security</a>
<a href="https://im4change.in/search?qryStr=Law and Justice"
target="_blank" class="tag-link-4 font4">Law and Justice</a>
<a href="https://im4change.in/search?qryStr=Health"
target="_blank" class="tag-link-4 font4">Health</a>
<a href="https://im4change.in/search?qryStr=Right to Food"
target="_blank" class="tag-link-4 font4">Right to Food</a>
<a href="https://im4change.in/search?qryStr=Corruption"
target="_blank" class="tag-link-4 font4">Corruption</a>
<a href="https://im4change.in/search?qryStr=farming"
target="_blank" class="tag-link-4 font4">farming</a>
<a href="https://im4change.in/search?qryStr=Environment"
target="_blank" class="tag-link-4 font4">Environment</a>
<a href="https://im4change.in/search?qryStr=Right to Information"
target="_blank" class="tag-link-4 font4">Right to Information</a>
<a href="https://im4change.in/search?qryStr=NREGS"
target="_blank" class="tag-link-4 font4">NREGS</a>
<a href="https://im4change.in/search?qryStr=Human Rights"
target="_blank" class="tag-link-4 font4">Human Rights</a>
<a href="https://im4change.in/search?qryStr=Governance"
target="_blank" class="tag-link-4 font4">Governance</a>
<a href="https://im4change.in/search?qryStr=PDS"
target="_blank" class="tag-link-4 font4">PDS</a>
<a href="https://im4change.in/search?qryStr=COVID-19"
target="_blank" class="tag-link-4 font4">COVID-19</a>
<a href="https://im4change.in/search?qryStr=Land Acquisition"
target="_blank" class="tag-link-4 font4">Land Acquisition</a>
<a href="https://im4change.in/search?qryStr=mgnrega"
target="_blank" class="tag-link-4 font4">mgnrega</a>
<a href="https://im4change.in/search?qryStr=Farmers"
target="_blank" class="tag-link-4 font4">Farmers</a>
<a href="https://im4change.in/search?qryStr=transparency"
target="_blank" class="tag-link-4 font4">transparency</a>
<a href="https://im4change.in/search?qryStr=Gender"
target="_blank" class="tag-link-4 font4">Gender</a>
<a href="https://im4change.in/search?qryStr=Poverty"
target="_blank" class="tag-link-4 font4">Poverty</a>
<a href="https://im4change.in/search?qryStr=Farm Laws" target="_blank" class="tag-link-4 font4">Farm Laws
</a>
<a href="https://im4change.in/search?qryStr=Citizenship Amendment Act" target="_blank" class="tag-link-4 font4">Citizenship Amendment Act
</a>
<a href="https://im4change.in/search?qryStr=CAA NPR NRIC" target="_blank" class="tag-link-4 font4">CAA NPR NRIC
</a>
<a href="https://im4change.in/search?qryStr=Job Losses" target="_blank" class="tag-link-4 font4">Job Losses
</a>
<a href="https://im4change.in/search?qryStr=Migrant Workers" target="_blank" class="tag-link-4 font4">Migrant Workers
</a>
<a href="https://im4change.in/search?qryStr=Unemployment" target="_blank" class="tag-link-4 font4">Unemployment
</a>
<a href="https://im4change.in/search?qryStr=PMGKAY" target="_blank" class="tag-link-4 font4">PMGKAY
</a>
<a href="https://im4change.in/search?qryStr=PM-KISAN" target="_blank" class="tag-link-4 font4">PM-KISAN
</a>
<a href="https://im4change.in/search?qryStr=PM-CARES" target="_blank" class="tag-link-4 font4">PM-CARES
</a>
<a href="https://im4change.in/search?qryStr=LFPR" target="_blank" class="tag-link-4 font4">LFPR
</a>
</div>
</div>
</div>
<!-- Widget Tag Cloud Ends here -->
</aside>
<!-- Right Side Section End -->
</div>
<section class="cat-box cats-review-box footerSec">
<h2 class="cat-box-title vSec CatArcha">Video
Archives</h2>
<h2 class="cat-box-title CatArchaTitle">Archives</h2>
<div class="cat-box-content">
<div class="reviews-cat">
<div class="CatArchaDiv1">
<div class="CatArchaDiv2">
<ul>
<li>
<a href="https://im4change.in/news-alerts-57/moving-upstream-luni-fellowship.html" target="_blank">
Moving Upstream: Luni – Fellowship </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/135-million-indians-exited-multidimensional-poverty-as-per-government-figures-is-that-the-same-as-poverty-reduction.html" target="_blank">
135 Million Indians Exited “Multidimensional" Poverty as per Government... </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/explainer-why-are-tomato-prices-on-fire.html" target="_blank">
Explainer: Why are Tomato Prices on Fire? </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/nsso-survey-only-39-1-of-all-households-have-drinking-water-within-dwelling-46-7-of-rural-households-use-firewood-for-cooking.html" target="_blank">
NSSO Survey: Only 39.1% of all Households have Drinking... </a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/news-alerts-57"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/I51LYnP8BOk/1.jpg"
alt=" Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Short-Video-on-im4change-Hindi-website-Inclusive-Media-for-Change" target="_blank">
Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/kNqha-SwfIY/1.jpg"
alt=" "Session 1: Scope of IDEA and AgriStack" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-1- Scope-of-IDEA-and-AgriStack-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 1: Scope of IDEA and AgriStack" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/6kIVjlgZItk/1.jpg"
alt=" "Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-2-Farmer-Centric-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/2BeHTu0y7xc/1.jpg"
alt=" "Session 3: Future of Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-3-Future-of-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 3: Future of Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="divWidth">
<ul class="divWidthMarg">
<li>
<a href="https://im4change.in/video/Public-Spending-on-Agriculture-in-India-Source-Foundation-for-Agrarian-Studies"
title="Public Spending on Agriculture in India (Source: Foundation for Agrarian Studies)" target="_blank">
Public Spending on Agriculture in India (Source: Foundation for...</a>
</li>
<li>
<a href="https://im4change.in/video/Agrarian-Change-Seminar-Protests-against-the-New-Farm-Laws-in-India-by-Prof-Vikas-Rawal-JNU-Source-Journal-Of-Agrarian-Change"
title="Agrarian Change Seminar: 'Protests against the New Farm Laws in India' by Prof. Vikas Rawal, JNU (Source: Journal Of Agrarian Change) " target="_blank">
Agrarian Change Seminar: 'Protests against the New Farm Laws...</a>
</li>
<li>
<a href="https://im4change.in/video/Webinar-Ramrao-The-Story-of-India-Farm-Crisis-Source-Azim-Premji-University"
title="Webinar: Ramrao - The Story of India's Farm Crisis (Source: Azim Premji University)" target="_blank">
Webinar: Ramrao - The Story of India's Farm Crisis...</a>
</li>
<li>
<a href="https://im4change.in/video/water-and-agricultural-transformation-in-India"
title="Water and Agricultural Transformation in India: A Symbiotic Relationship (Source: IGIDR)" target="_blank">
Water and Agricultural Transformation in India: A Symbiotic Relationship...</a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/videogallery"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
</div>
</div>
</div>
</section> </div>
<div class="clear"></div>
<!-- Footer option Starts here -->
<div class="footer-bottom fade-in animated4">
<div class="container">
<div class="social-icons icon_flat">
<p class="SocialMargTop"> Website Developed by <a target="_blank" title="Web Development"
class="wot right"
href="http://www.ravinderkhurana.com/" rel="nofollow">
RAVINDErkHURANA.com</a></p>
</div>
<div class="alignleft">
<a
target="_blank" href="https://im4change.in/objectives-8.html"
class="link"
title="Objectives">Objectives</a> | <a
target="_blank" href="https://im4change.in/about-us-9.html"
class="link" title="About Us">About Us</a> | <a
target="_blank" href="https://im4change.in/media-workshops.php"
class="ucwords">Workshops</a> | <a
target="_blank" href="https://im4change.in/disclaimer/disclaimer-149.html"
title="Disclaimer">Disclaimer</a> </div>
</div>
</div>
<!-- Footer option ends here -->
</div>
<div id="connect">
<a target="_blank"
href="http://www.facebook.com/sharer.php?u=https://im4change.in/latest-news-updates/80-of-medicines-not-covered-by-price-control-order-rema-nagarajan-23504.html"
title="Share on Facebook">
<img src="https://im4change.in/images/Facebook.png?1582080640" alt="share on Facebook" class="ImgBorder"/>
</a><br/>
<a target="_blank"
href="http://twitter.com/share?text=Im4change&url=https://im4change.in/latest-news-updates/80-of-medicines-not-covered-by-price-control-order-rema-nagarajan-23504.html"
title="Share on Twitter">
<img src="https://im4change.in/images/twitter.png?1582080632" alt="Twitter" class="ImgBorder"/> </a>
<br/>
<a href="/feeds" title="RSS Feed" target="_blank">
<img src="https://im4change.in/images/rss.png?1582080632" alt="RSS" class="ImgBorder"/>
</a>
<br/>
<a class="feedback-link" id="feedbackFormLink" href="#">
<img src="https://im4change.in/images/feedback.png?1582080630" alt="Feedback" class="ImgBorder"/>
</a> <br/>
<a href="javascript:function iprl5(){var d=document,z=d.createElement('scr'+'ipt'),b=d.body,l=d.location;try{if(!b)throw(0);d.title='(Saving...) '+d.title;z.setAttribute('src',l.protocol+'//www.instapaper.com/j/WKrH3R7ORD5p?u='+encodeURIComponent(l.href)+'&t='+(new Date().getTime()));b.appendChild(z);}catch(e){alert('Please wait until the page has loaded.');}}iprl5();void(0)"
class="bookmarklet" onclick="return explain_bookmarklet();">
<img src="https://im4change.in/images/read-it-later.png?1582080632" alt="Read Later" class="ImgBorder"/> </a>
</div>
<!-- Feedback form Starts here -->
<div id="feedbackForm" class="overlay_form" class="ImgBorder">
<h2>Contact Form</h2>
<div id="contactform1">
<div id="formleft">
<form id="submitform" action="/contactus.php" method="post">
<input type="hidden" name="submitform" value="submitform"/>
<input type="hidden" name="salt_key" value="a0e0f2c6a0644a70e57ad2c96829709a"/>
<input type="hidden" name="ref" value="feedback"/>
<fieldset>
<label>Name :</label>
<input type="text" name="name" class="tbox" required/>
</fieldset>
<fieldset>
<label>Email :</label>
<input type="text" name="email" class="tbox" required/>
</fieldset>
<fieldset>
<label>Message :</label>
<textarea rows="5" cols="20" name="message" required></textarea>
</fieldset>
<fieldset>
Please enter security code
<div class="clear"></div>
<input type="text" name="vrcode" class="tbox"/>
</fieldset>
<fieldset>
<input type="submit" class="button" value="Submit"/>
<a href="#" id="closefeedbakcformLink">Close</a>
</fieldset>
</form>
</div>
<div class="clearfix"></div>
</div>
</div>
<div id="donate_popup" class="modal" style="max-width: 800px;">
<table width="100%" border="1">
<tr>
<td colspan="2" align="center">
<b>Support im4change</b>
</td>
</tr>
<tr>
<td width="25%" valign="middle">
<img src="https://im4change.in/images/logo2.jpg?1582080632" alt="" width="100%"/> </td>
<td style="padding-left:10px;padding-top:10px;">
<form action="https://im4change.in/donate" method="get">
<table width="100%" cellpadding="2" cellspacing="2">
<tr>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
10
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
100
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
1000
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
50
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
500
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
<input type="text" name="price" placeholder="?" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td colspan="3" align="right">
<input type="button" name="Pay" value="Pay"
style="width: 200px;background-color: rgb(205, 35, 36);color: #ffffff;"/>
</td>
</tr>
</table>
</form>
</td>
</tr>
</table>
</div><script type='text/javascript'>
/* <![CDATA[ */
var tievar = {'go_to': 'Go to...'};
/* ]]> */
</script>
<script src="/js/tie-scripts.js?1575549704"></script><script src="/js/bootstrap.js?1575549704"></script><script src="/js/jquery.modal.min.js?1578284310"></script><script>
$(document).ready(function() {
// tell the autocomplete function to get its data from our php script
$('#s').autocomplete({
source: "/autocomplete"
});
});
</script>
<script src="/vj-main-sw-register.js" async></script>
<script>function init(){var imgDefer=document.getElementsByTagName('img');for(var i=0;i<imgDefer.length;i++){if(imgDefer[i].getAttribute('data-src')){imgDefer[i].setAttribute('src',imgDefer[i].getAttribute('data-src'))}}}
window.onload=init;</script>
</body>
</html>'
}
$reasonPhrase = 'OK'
header - [internal], line ??
Cake\Http\ResponseEmitter::emitStatusLine() - CORE/src/Http/ResponseEmitter.php, line 148
Cake\Http\ResponseEmitter::emit() - CORE/src/Http/ResponseEmitter.php, line 54
Cake\Http\Server::emit() - CORE/src/Http/Server.php, line 141
[main] - ROOT/webroot/index.php, line 39
Warning (2): Cannot modify header information - headers already sent by (output started at /home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php:853) [CORE/src/Http/ResponseEmitter.php, line 181]
$response = object(Cake\Http\Response) {
'status' => (int) 200,
'contentType' => 'text/html',
'headers' => [
'Content-Type' => [
[maximum depth reached]
]
],
'file' => null,
'fileRange' => [],
'cookies' => object(Cake\Http\Cookie\CookieCollection) {},
'cacheDirectives' => [],
'body' => '<!DOCTYPE html>
<!--[if lt IE 7 ]>
<html class="ie ie6" lang='en'> <![endif]-->
<!--[if IE 7 ]>
<html class="ie ie7" lang='en'> <![endif]-->
<!--[if IE 8 ]>
<html class="ie ie8" lang='en'> <![endif]-->
<!--[if (gte IE 9)|!(IE)]><!-->
<html lang='en'>
<!--<![endif]-->
<head><meta http-equiv="Content-Type" content="text/html; charset=utf-8">
<title>
LATEST NEWS UPDATES | 80% of medicines not covered by price control order -Rema Nagarajan </title>
<meta name="description" content="
-The Times of India
About 38 million people in India (which is more than Canada's population) fall below the poverty line every year due to healthcare expenses, of which 70% is on purchase of drugs. Yet, the much-awaited drug price control..."/>
<meta name="keywords" content="medicines,Health,Public Health"/>
<meta name="news_keywords" content="medicines,Health,Public Health">
<link rel="alternate" type="application/rss+xml" title="ROR" href="/ror.xml"/>
<link rel="alternate" type="application/rss+xml" title="RSS 2.0" href="/feeds/"/>
<link rel="stylesheet" href="/css/bootstrap.min.css?1697864993"/> <link rel="stylesheet" href="/css/style.css?v=1.1.2"/> <link rel="stylesheet" href="/css/style-inner.css?1577045210"/> <link rel="stylesheet" id="Oswald-css"
href="https://fonts.googleapis.com/css?family=Oswald%3Aregular%2C700&ver=3.8.1" type="text/css"
media="all">
<link rel="stylesheet" href="/css/jquery.modal.min.css?1578285302"/> <script src="/js/jquery-1.10.2.js?1575549704"></script> <script src="/js/jquery-migrate.min.js?1575549704"></script> <link rel="shortcut icon" href="/favicon.ico" title="Favicon">
<link rel="stylesheet" href="/css/jquery-ui.css?1580720609"/> <script src="/js/jquery-ui.js?1575549704"></script> <link rel="preload" as="style" href="https://www.im4change.org/css/custom.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery.modal.min.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery-ui.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/li-scroller.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<!-- <link rel="preload" as="style" href="https://www.im4change.org/css/style.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous"> -->
<link rel="preload" as="style" href="https://www.im4change.org/css/style-inner.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel='dns-prefetch' href="//im4change.org/css/custom.css" crossorigin >
<link rel="preload" as="script" href="https://www.im4change.org/js/bootstrap.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.li-scroller.1.0.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.modal.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.ui.totop.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-1.10.2.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-migrate.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-ui.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/setting.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/tie-scripts.js">
<!--[if IE]>
<script type="text/javascript">jQuery(document).ready(function () {
jQuery(".menu-item").has("ul").children("a").attr("aria-haspopup", "true");
});</script>
<![endif]-->
<!--[if lt IE 9]>
<script src="/js/html5.js"></script>
<script src="/js/selectivizr-min.js"></script>
<![endif]-->
<!--[if IE 8]>
<link rel="stylesheet" type="text/css" media="all" href="/css/ie8.css"/>
<![endif]-->
<meta property="og:title" content="LATEST NEWS UPDATES | 80% of medicines not covered by price control order -Rema Nagarajan" />
<meta property="og:url" content="https://im4change.in/latest-news-updates/80-of-medicines-not-covered-by-price-control-order-rema-nagarajan-23504.html" />
<meta property="og:type" content="article" />
<meta property="og:description" content="
-The Times of India
About 38 million people in India (which is more than Canada's population) fall below the poverty line every year due to healthcare expenses, of which 70% is on purchase of drugs. Yet, the much-awaited drug price control..." />
<meta property="og:image" content="" />
<meta property="fb:app_id" content="0" />
<meta name="viewport" content="width=device-width, initial-scale=1, maximum-scale=1, user-scalable=no">
<link rel="apple-touch-icon-precomposed" sizes="144x144" href="https://im4change.in/images/apple1.png">
<link rel="apple-touch-icon-precomposed" sizes="120x120" href="https://im4change.in/images/apple2.png">
<link rel="apple-touch-icon-precomposed" sizes="72x72" href="https://im4change.in/images/apple3.png">
<link rel="apple-touch-icon-precomposed" href="https://im4change.in/images/apple4.png">
<style>
.gsc-results-wrapper-overlay{
top: 38% !important;
height: 50% !important;
}
.gsc-search-button-v2{
border-color: #035588 !important;
background-color: #035588 !important;
}
.gsib_a{
height: 30px !important;
padding: 2px 8px 1px 6px !important;
}
.gsc-search-button-v2{
height: 41px !important;
}
input.gsc-input{
background: none !important;
}
@media only screen and (max-width: 600px) {
.gsc-results-wrapper-overlay{
top: 11% !important;
width: 87% !important;
left: 9% !important;
height: 43% !important;
}
.gsc-search-button-v2{
padding: 10px 10px !important;
}
.gsc-input-box{
height: 28px !important;
}
/* .gsib_a {
padding: 0px 9px 4px 9px !important;
}*/
}
@media only screen and (min-width: 1200px) and (max-width: 1920px) {
table.gsc-search-box{
width: 15% !important;
float: right !important;
margin-top: -118px !important;
}
.gsc-search-button-v2 {
padding: 6px !important;
}
}
</style>
<script>
$(function () {
$("#accordion").accordion({
event: "click hoverintent"
});
});
/*
* hoverIntent | Copyright 2011 Brian Cherne
* http://cherne.net/brian/resources/jquery.hoverIntent.html
* modified by the jQuery UI team
*/
$.event.special.hoverintent = {
setup: function () {
$(this).bind("mouseover", jQuery.event.special.hoverintent.handler);
},
teardown: function () {
$(this).unbind("mouseover", jQuery.event.special.hoverintent.handler);
},
handler: function (event) {
var currentX, currentY, timeout,
args = arguments,
target = $(event.target),
previousX = event.pageX,
previousY = event.pageY;
function track(event) {
currentX = event.pageX;
currentY = event.pageY;
}
;
function clear() {
target
.unbind("mousemove", track)
.unbind("mouseout", clear);
clearTimeout(timeout);
}
function handler() {
var prop,
orig = event;
if ((Math.abs(previousX - currentX) +
Math.abs(previousY - currentY)) < 7) {
clear();
event = $.Event("hoverintent");
for (prop in orig) {
if (!(prop in event)) {
event[prop] = orig[prop];
}
}
// Prevent accessing the original event since the new event
// is fired asynchronously and the old event is no longer
// usable (#6028)
delete event.originalEvent;
target.trigger(event);
} else {
previousX = currentX;
previousY = currentY;
timeout = setTimeout(handler, 100);
}
}
timeout = setTimeout(handler, 100);
target.bind({
mousemove: track,
mouseout: clear
});
}
};
</script>
<script type="text/javascript">
var _gaq = _gaq || [];
_gaq.push(['_setAccount', 'UA-472075-3']);
_gaq.push(['_trackPageview']);
(function () {
var ga = document.createElement('script');
ga.type = 'text/javascript';
ga.async = true;
ga.src = ('https:' == document.location.protocol ? 'https://ssl' : 'http://www') + '.google-analytics.com/ga.js';
var s = document.getElementsByTagName('script')[0];
s.parentNode.insertBefore(ga, s);
})();
</script>
<link rel="stylesheet" href="/css/custom.css?v=1.16"/> <script src="/js/jquery.ui.totop.js?1575549704"></script> <script src="/js/setting.js?1575549704"></script> <link rel="manifest" href="/manifest.json">
<meta name="theme-color" content="#616163" />
<meta name="apple-mobile-web-app-capable" content="yes">
<meta name="apple-mobile-web-app-status-bar-style" content="black">
<meta name="apple-mobile-web-app-title" content="im4change">
<link rel="apple-touch-icon" href="/icons/logo-192x192.png">
</head>
<body id="top" class="home inner blog">
<div class="background-cover"></div>
<div class="wrapper animated">
<header id="theme-header" class="header_inner" style="position: relative;">
<div class="logo inner_logo" style="left:20px !important">
<a title="Home" href="https://im4change.in/">
<img src="https://im4change.in/images/logo2.jpg?1582080632" class="logo_image" alt="im4change"/> </a>
</div>
<div class="langhindi" style="color: #000;display:none;"
href="https://im4change.in/">
<a class="more-link" href="https://im4change.in/">Home</a>
<a href="https://im4change.in/hindi/" class="langbutton ">हिन्दी</a>
</div>
<nav class="fade-in animated2" id="main-nav">
<div class="container">
<div class="main-menu">
<ul class="menu" id="menu-main">
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
style="left: -40px;"><a
target="_blank" href="https://im4change.in/">Home</a>
</li>
<li class="menu-item mega-menu menu-item-type-taxonomy mega-menu menu-item-object-category mega-menu menu-item-has-children parent-list"
style=" margin-left: -40px;"><a href="#">KNOWLEDGE GATEWAY <span class="sub-indicator"></span>
</a>
<div class="mega-menu-block background_menu" style="padding-top:25px;">
<div class="container">
<div class="mega-menu-content">
<div class="mega-menu-item">
<h3><b>Farm Crisis</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/farmers039-suicides-14.html"
class="left postionrel">Farm Suicides </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/unemployment-30.html"
class="left postionrel">Unemployment </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/rural-distress-70.html"
class="left postionrel">Rural distress </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/migration-34.html"
class="left postionrel">Migration </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/key-facts-72.html"
class="left postionrel">Key Facts </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/debt-trap-15.html"
class="left postionrel">Debt Trap </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Empowerment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/union-budget-73.html"
class="left postionrel">Union Budget And Other Economic Policies </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/forest-and-tribal-rights-61.html"
class="left postionrel">Forest and Tribal Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-education-60.html"
class="left postionrel">Right to Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-food-59.html"
class="left postionrel">Right to Food </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/displacement-3279.html"
class="left postionrel">Displacement </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-work-mg-nrega-39.html"
class="left postionrel">Right to Work (MG-NREGA) </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/gender-3280.html"
class="left postionrel">GENDER </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-information-58.html"
class="left postionrel">Right to Information </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/social-audit-48.html"
class="left postionrel">Social Audit </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Hunger / HDI</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/poverty-and-inequality-20499.html"
class="left postionrel">Poverty and inequality </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/malnutrition-41.html"
class="left postionrel">Malnutrition </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/public-health-51.html"
class="left postionrel">Public Health </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/education-50.html"
class="left postionrel">Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hunger-overview-40.html"
class="left postionrel">Hunger Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hdi-overview-45.html"
class="left postionrel">HDI Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/pds-ration-food-security-42.html"
class="left postionrel">PDS/ Ration/ Food Security </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/sdgs-113.html"
class="left postionrel">SDGs </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/mid-day-meal-scheme-mdms-53.html"
class="left postionrel">Mid Day Meal Scheme (MDMS) </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Environment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/time-bomb-ticking-52.html"
class="left postionrel">Time Bomb Ticking </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/water-and-sanitation-55.html"
class="left postionrel">Water and Sanitation </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/impact-on-agriculture-54.html"
class="left postionrel">Impact on Agriculture </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Law & Justice</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/social-justice-20500.html"
class="left postionrel">Social Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/access-to-justice-47.html"
class="left postionrel">Access to Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/human-rights-56.html"
class="left postionrel">Human Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/corruption-35.html"
class="left postionrel">Corruption </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/general-insecurity-46.html"
class="left postionrel">General Insecurity </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/disaster-relief-49.html"
class="left postionrel">Disaster & Relief </a>
</p>
</div>
</div>
</div>
</div>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page "><a target="_blank" href="https://im4change.in/nceus_reports.php">NCEUS reports</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children parent-list ">
<a target="_blank" href="https://im4change.in/about-us-9.html">About Us <span
class="sub-indicator"></span></a>
<ul class="sub-menu aboutmenu">
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/objectives-8.html">Objectives</a>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/contactus.php">Contact
Us</a></li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/about-us-9.html">About
Us</a></li>
</ul>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children ">
<a target="_blank" href="https://im4change.in/fellowships.php" title="Fellowships">Fellowships</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/media-workshops.php">Workshops</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/research.php">Research</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/links-64">Partners</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
id="menu-item-539"><a target="_blank" href="https://im4change.in/hindi/"
class="langbutton langlinkfont17">हिन्दी</a></li>
</ul>
</div> </div>
<!-- <div style="float: right;">
<script async src="https://cse.google.com/cse.js?cx=18b4f2e0f11bed3dd"></script>
<div class="gcse-search"></div>
</div> -->
<div class="search-block" style=" margin-left: 8px; margin-right: 7px;">
<form method="get" id="searchform" name="searchform"
action="https://im4change.in/search"
onsubmit="return searchvalidate();">
<button class="search-button" type="submit" value="Search"></button>
<input type="text" id="s" name="qryStr" value=""
onfocus="if (this.value == 'Search...') {this.value = '';}"
onblur="if (this.value == '') {this.value = 'Search...';}">
</form>
</div>
</nav>
</header>
<div class="container">
<div id="main-content" class=" main1 container fade-in animated3 sidebar-narrow-left">
<div class="content-wrap">
<div class="content" style="width: 900px;min-height: 500px;">
<section class="cat-box recent-box innerCatRecent">
<h1 class="cat-box-title">80% of medicines not covered by price control order -Rema Nagarajan</h1>
<a href="JavaScript:void(0);" onclick="return shareArticle(23342);">
<img src="https://im4change.in/images/email.png?1582080630" border="0" width="24" align="right" alt="Share this article"/> </a>
<a href="https://im4change.in/latest-news-updates/80-of-medicines-not-covered-by-price-control-order-rema-nagarajan-23504/print"
rel="nofollow">
<img src="https://im4change.in/images/icon-print.png?1582080630" border="0" width="24" align="right" alt="Share this article"/>
</a>
</section>
<section class="recent-box innerCatRecent">
<small class="pb-1"><span class="dateIcn">
<img src="https://im4change.in/images/published.svg?1582080666" alt="published"/>
Published on</span><span class="text-date"> Dec 1, 2013</span>
<span
class="dateIcn">
<img src="https://im4change.in/images/modified.svg?1582080666" alt="modified"/> Modified on </span><span class="text-date"> Dec 1, 2013</span>
</small>
</section>
<div class="clear"></div>
<div style="padding-top: 10px;">
<div class="innerLineHeight">
<div class="middleContent innerInput latest-news-updates">
<table>
<tr>
<td>
<div>
<div align="justify">-The Times of India</div><p align="justify"><br />About 38 million people in India (which is more than Canada's population) fall below the poverty line every year due to healthcare expenses, of which 70% is on purchase of drugs. Yet, the much-awaited drug price control order (DPCO) 2013, meant to control the price of medicines does not cover over 80% of the medicines in the market. Many drugs crucial for India's disease profile have been left out, which means people are unlikely to see any significant reduction in expenditure on medicines.</p><p align="justify"><img src="https://im4change.in/siteadmin/tinymce/uploaded/Health_1.JPG" alt="Health" width="657" height="296" /> </p><p align="justify">In 2003, the Supreme Court, while hearing a case on the National Pharmaceutical Pricing Policy, had directed the government to formulate appropriate criteria to identify essential and life saving drugs and ensure that they came under price control. It took over a decade for the government to announce the DPCO in May 2013.</p><p align="justify">By the government's own admission in an affidavit filed in court, the market value and share of medicines covered by DPCO is just 18% of the country's pharma market. Many life-saving medicines including anti-cancer drugs, expensive antibiotics and drugs needed for organ transplantation have been left out.</p><p align="justify">The government merely lifted the entire National List of Essential Medicines (NLEM) 2011, comprising 348 medicines, and placed it under price control. "The literal translation of the NLEM into DPCO 2103 has been done without a thought of its implications. The companies have been provided a convenient escape route. A 500 mg Paracetamol tablet is under price control but its 650 mg strength is not; individual anti-TB drugs are under price control but their combinations which outsell single ingredient preparations are not. This undermines the entire objective of making essential medicines more affordable to Indians," explained Dr Anurag Bhargava, associate professor at the Himalayan Institute of Medical Sciences. He stressed the need to expand the scope of price control to include all dosages and combinations, as was the case in the previous DPCO of 1995.</p><p align="justify">With the current DPCO not covering combinations of drugs, a lot of drugs for diabetes and hypertension and many other conditions will move out of price control as they are used in combination. The combinations not covered under NLEM account for Rs 31,866 crore or almost 45% of the total pharma market of Rs 71,246 crore in 2012.</p><p align="justify">An independent evaluation of the National Pharmaceutical Pricing Policy, by the Public Health Foundation of India (PHFI) and the Institute for Studies in Industrial Development (ISID) for a forthcoming report explains why it is important to expand the scope of price control. According to their evaluation, the market value of anti-infectives under price control is Rs 4,636 crore, just 6.5% of the total market. Anti-infectives, which include antibiotics, have the biggest chunk of India's pharma market.</p><p align="justify">"Our evaluation shows that if price control was expanded to combinations, additional strengths and dosages of just the anti-infectives included in the NLEM, the total market value would be worth more than Rs 10,500 crore, about 15% of the total pharma market, a vast improvement over the current coverage of just 6.5%," said Malini Aisola of PHFI.</p><p align="justify">The essential medicines list does not seem to have taken into account India's disease profile as it leaves out several drugs crucial for treating many common conditions, pointed out Dr Bhargava. The government's own affidavit admits that only 18% of anti-diabetics, 19% of anti-TB medicines and 6% of the respiratory therapeutics segment are under price control. This is despite India being the diabetes and TB capital of the world, and facing high prevalence of asthma and chronic obstructive pulmonary disease (COPD).</p><p align="justify">There's good reason why we need price controls. The MRP charged by companies is often many times the cost of production leaving them with profit margins unheard of in any other sector. Price control was meant to address this problem, particularly in medicines important for India. But it has failed to make any significant difference.</p><p align="justify">One reason is the way prices are determined under the current DPCO. Under the 1995 DPCO, the drugs prices under controls was decided by taking the cost of manufacture and fixing a certain percentage as mark-up, which included packaging and distribution costs, retailers' margin, excise duty and profit. But the current DPCO uses a new formula under which the price is fixed by taking the average price of brands having one per cent or more of market share and adding 16% as retail margin.</p><p align="justify">S Srinivasan of LOCOST, a company producing drugs for use by NGOs to treat the poor, explained how the cost of manufacture, including retail margin, for Cetrizine, an anti-allergic, is just Rs 1.20 for ten tablets. The ceiling price under the DPCO is Rs 18.10, the same as the price charged by the market leader GSK. This allows a price that is 15 times the cost of manufacture. In the case of Albendazole, a drug used to treat worm infections, the cost of manufacture including retail margin is Rs 8.50 per 10 tablets, while the DPCO ceiling price is over Rs 91, a ten-fold mark-up, pointed out Srinivasan. The price charged by the market leader in Albendazole, GSK, was Rs 140 per ten tablets. In this case, while price control should bring down the market leader's price, it still allows a huge profit margin. In fact, the PHFI-ISID evaluation shows that in 43% of drugs studied, the sales leader will face little or no impact from price control.</p><p align="justify">To show how effective DPCO has been, the government has compared the price reductions due to DPCO with the highest price of a drug. However, PHFI and ISID point out, it makes more sense to use the price charged by the company with the highest market share for comparison. Out of the 390 formulations for which prices have been notified, in 212 the company with the highest sales does not have the highest price. So, the price reduction achieved by DPCO is nowhere as dramatic as claimed by the government. PHFI and ISID have conducted an independent analysis using the same data as used by the government. Their calculation for 369 formulations shows that the effective average price reduction would be just 11% and the impact on the pharma market as a whole would be a mere 1.8%.</p><p align="justify">In sum, coming in 2013, a decade after the Supreme Court asked for it, the DPCO is clearly late. But even worse, as the PHFI-ISID study reveals, it is too little. Given how much rides on this for the aam aadmi, that is a tragedy of mammoth proportions.About 38 million people in India (which is more than Canada's population) fall below the poverty line every year due to healthcare expenses, of which 70% is on purchase of drugs. Yet, the much-awaited drug price control order (DPCO) 2013, meant to control the price of medicines does not cover over 80% of the medicines in the market. Many drugs crucial for India's disease profile have been left out, which means people are unlikely to see any significant reduction in expenditure on medicines.</p><p align="justify">In 2003, the Supreme Court, while hearing a case on the National Pharmaceutical Pricing Policy, had directed the government to formulate appropriate criteria to identify essential and life saving drugs and ensure that they came under price control. It took over a decade for the government to announce the DPCO in May 2013.</p><p align="justify">By the government's own admission in an affidavit filed in court, the market value and share of medicines covered by DPCO is just 18% of the country's pharma market. Many life-saving medicines including anti-cancer drugs, expensive antibiotics and drugs needed for organ transplantation have been left out.</p><p align="justify">The government merely lifted the entire National List of Essential Medicines (NLEM) 2011, comprising 348 medicines, and placed it under price control. "The literal translation of the NLEM into DPCO 2103 has been done without a thought of its implications. The companies have been provided a convenient escape route. A 500 mg Paracetamol tablet is under price control but its 650 mg strength is not; individual anti-TB drugs are under price control but their combinations which outsell single ingredient preparations are not. This undermines the entire objective of making essential medicines more affordable to Indians," explained Dr Anurag Bhargava, associate professor at the Himalayan Institute of Medical Sciences. He stressed the need to expand the scope of price control to include all dosages and combinations, as was the case in the previous DPCO of 1995.</p><p align="justify">With the current DPCO not covering combinations of drugs, a lot of drugs for diabetes and hypertension and many other conditions will move out of price control as they are used in combination. The combinations not covered under NLEM account for Rs 31,866 crore or almost 45% of the total pharma market of Rs 71,246 crore in 2012.</p><p align="justify">An independent evaluation of the National Pharmaceutical Pricing Policy, by the Public Health Foundation of India (PHFI) and the Institute for Studies in Industrial Development (ISID) for a forthcoming report explains why it is important to expand the scope of price control. According to their evaluation, the market value of anti-infectives under price control is Rs 4,636 crore, just 6.5% of the total market. Anti-infectives, which include antibiotics, have the biggest chunk of India's pharma market.</p><p align="justify">"Our evaluation shows that if price control was expanded to combinations, additional strengths and dosages of just the anti-infectives included in the NLEM, the total market value would be worth more than Rs 10,500 crore, about 15% of the total pharma market, a vast improvement over the current coverage of just 6.5%," said Malini Aisola of PHFI.</p><p align="justify">The essential medicines list does not seem to have taken into account India's disease profile as it leaves out several drugs crucial for treating many common conditions, pointed out Dr Bhargava. The government's own affidavit admits that only 18% of anti-diabetics, 19% of anti-TB medicines and 6% of the respiratory therapeutics segment are under price control. This is despite India being the diabetes and TB capital of the world, and facing high prevalence of asthma and chronic obstructive pulmonary disease (COPD).</p><p align="justify">There's good reason why we need price controls. The MRP charged by companies is often many times the cost of production leaving them with profit margins unheard of in any other sector. Price control was meant to address this problem, particularly in medicines important for India. But it has failed to make any significant difference.</p><p align="justify">One reason is the way prices are determined under the current DPCO. Under the 1995 DPCO, the drugs prices under controls was decided by taking the cost of manufacture and fixing a certain percentage as mark-up, which included packaging and distribution costs, retailers' margin, excise duty and profit. But the current DPCO uses a new formula under which the price is fixed by taking the average price of brands having one per cent or more of market share and adding 16% as retail margin.</p><p align="justify">S Srinivasan of LOCOST, a company producing drugs for use by NGOs to treat the poor, explained how the cost of manufacture, including retail margin, for Cetrizine, an anti-allergic, is just Rs 1.20 for ten tablets. The ceiling price under the DPCO is Rs 18.10, the same as the price charged by the market leader GSK. This allows a price that is 15 times the cost of manufacture. In the case of Albendazole, a drug used to treat worm infections, the cost of manufacture including retail margin is Rs 8.50 per 10 tablets, while the DPCO ceiling price is over Rs 91, a ten-fold mark-up, pointed out Srinivasan. The price charged by the market leader in Albendazole, GSK, was Rs 140 per ten tablets. In this case, while price control should bring down the market leader's price, it still allows a huge profit margin. In fact, the PHFI-ISID evaluation shows that in 43% of drugs studied, the sales leader will face little or no impact from price control.</p><p align="justify">To show how effective DPCO has been, the government has compared the price reductions due to DPCO with the highest price of a drug. However, PHFI and ISID point out, it makes more sense to use the price charged by the company with the highest market share for comparison. Out of the 390 formulations for which prices have been notified, in 212 the company with the highest sales does not have the highest price. So, the price reduction achieved by DPCO is nowhere as dramatic as claimed by the government. PHFI and ISID have conducted an independent analysis using the same data as used by the government. Their calculation for 369 formulations shows that the effective average price reduction would be just 11% and the impact on the pharma market as a whole would be a mere 1.8%.</p><p align="justify">In sum, coming in 2013, a decade after the Supreme Court asked for it, the DPCO is clearly late. But even worse, as the PHFI-ISID study reveals, it is too little. Given how much rides on this for the aam aadmi, that is a tragedy of mammoth proportions.</p>
</div>
</td>
</tr>
</table>
</div>
</div>
</div>
<div class="clear"></div>
<br><a href="http://timesofindia.indiatimes.com/india/80-of-medicines-not-covered-by-price-control-order/articleshow/26678324.cms" class="re" target="_blank">The Times of India, 1 December, 2013, http://timesofindia.indiatimes.com/india/80-of-medicines-not-covered-by-price-control-order/articleshow/26678324.cms</a><div class="clear"></div>
<div style="padding-top: 18px;">
<p class="post-tag">Tagged with:
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=medicines"
title="medicines">
medicines </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Health"
title="Health">
Health </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Public Health"
title="Public Health">
Public Health </a>
</p>
</div>
<div class="clear"></div>
<br><br>
<div class="widget-top">
<h4>Related Articles</h4>
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<ul id="recentcomments">
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/fifth-report-from-gambia-implicates-indian-drug-maker-for-contaminated-syrups-banjot-kaur.html"
title="Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur">
Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-may-have-seen-steepest-dip-in-multidimensional-poverty-among-110-nations-as-per-undp-data-nikhil-rampal.html"
title="India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal">
India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/health-among-top-three-priorities-for-indian-voters-after-jobs-and-education-survey-shows-oliver-heath-jyoti-mishra-louise-tillin-sandhya-venkateswaran.html"
title="Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran">
Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/prevalence-of-zero-food-among-infants-and-young-children-in-india-patterns-of-change-across-the-states-and-union-territories-of-india-1993-2021-the-lancet.html"
title="Prevalence of Zero-Food among infants and young children in India - The Lancet ">
Prevalence of Zero-Food among infants and young children in India - The Lancet </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-s-sustainability-goals-at-risk-because-of-extreme-heatwaves-carbon-copy.html"
title="India's Sustainability Goals at Risk Because of Extreme Heatwaves - Carbon Copy">
India's Sustainability Goals at Risk Because of Extreme Heatwaves - Carbon Copy </a>
</li>
</ul>
</div>
<div class="comment-respond" id="respond">
<a name="commentbox"> </a>
<h3 class="comment-reply-title" id="reply-title">Write Comments</h3>
<form method="post" accept-charset="utf-8" role="form" action="/latest-news-updates/80-of-medicines-not-covered-by-price-control-order-rema-nagarajan-23504.html"><div style="display:none;"><input type="hidden" name="_method" value="POST"/></div> <form class="comment-form" id="commentform" method="post" action="#commentbox" onSubmit="return validate()"
name="cmtform">
<input type="hidden" name="cmttype" value="articlecmt"/>
<input type="hidden" name="article_id" value="23342"/>
<p class="comment-notes">Your email address will not be published. Required fields are marked <span
class="required">*</span></p>
<p class="comment-form-author">
<label for="commenterName">Name</label>
<span class="required">*</span>
<input type="text" aria-required="true" size="30"
value=""
name="commenterName" id="commenterName" required="true">
</p>
<p class="comment-form-email">
<label for="commenterEmail">Email</label> <span class="required">*</span>
<input aria-required="true" size="30" name="commenterEmail" id="commenterEmail" type="email"
value=""
required="true">
</p>
<p class="comment-form-contact">
<label for="commenterPh">Contact No.</label>
<input type="text" size="30"
value=""
name="commenterPh" id="commenterPh">
</p>
<p class="comment-form-comment">
<label for="comment">Comment</label>
<textarea aria-required="true" required="true" rows="8" cols="45" name="comment"
id="comment"></textarea>
</p>
<p class="comment-form-comment">
<label for="comment">Type the characters you see in the image below <span class="required">*</span><br><img
class="captchaImg"
src="https://im4change.in/securimage_show_art.php?tk=1865397053" alt="captcha"/>
</label>
</p>
<input type="text" name="vrcode" required="true"/>
<p class="form-submit" style="width: 200px;">
<input type="submit" value="Post Comment" id="submit" name="submit">
</p></form>
</div>
<style>
.ui-widget-content {
height: auto !important;
}
</style>
<div id="share-modal"></div>
<style>
.middleContent a{
background-color: rgba(108,172,228,.2);
}
.middleContent a:hover{
background-color: #418fde;
border-color: #418fde;
color: #000;
}
</style>
<script>
function shareArticle(article_id) {
var options = {
modal: true,
height: 'auto',
width: 600 + 'px'
};
$('#share-modal').html("");
$('#share-modal').load('https://im4change.in/share_article?article_id=' + article_id).dialog(options).dialog('open');
}
function postShare() {
var param = 'article_id=' + $("#article_id").val();
param = param + '&y_name=' + $("#y_name").val();
param = param + '&y_email=' + $("#y_email").val();
param = param + '&f_name=' + $("#f_name").val();
param = param + '&f_email=' + $("#f_email").val();
param = param + '&y_msg=' + $("#y_msg").val();
$.ajax({
type: "POST",
url: 'https://im4change.in/post_share_article',
data: param,
success: function (response) {
$('#share-modal').html("Thank You, Your message posted to ");
}
});
return false;
}
</script> </div>
</div>
<!-- Right Side Section Start -->
<!-- MAP Section START -->
<aside class="sidebar indexMarg">
<div class="ad-cell">
<a href="https://im4change.in/statemap.php" title="">
<img src="https://im4change.in/images/map_new_version.png?1582080666" alt="India State Map" class="indiamap" width="232" height="252"/> </a>
<div class="rightmapbox">
<div id="sideOne" class="docltitle"><a href="https://im4change.in/state-report/india/36" target="_blank">DOCUMENTS/
REPORTS</a></div>
<div id="sideTwo" class="statetitle"><a href="https://im4change.in/states.php"target="_blank">STATE DATA/
HDRs.</a></div>
</div>
<div class="widget widgePadTop"></div>
</div>
</aside>
<!-- MAP Section END -->
<aside class="sidebar sidePadbottom">
<div class="rightsmlbox1" >
<a href="https://im4change.in/knowledge_gateway" target="_blank" style="color: #035588;
font-size: 17px;">
KNOWLEDGE GATEWAY
</a>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/newsletter" target="_blank">
NEWSLETTER
</a>
</p>
</div>
</div>
<div class="rightsmlbox1" style="height: 325px;">
<div>
<p class="rightsmlbox1_title">
Interview with Prof. Ravi Srivastava
</p>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/video/interview-with-prof-ravi-srivastava-on-current-economic-crisis">
<img width="250" height="200" src="/images/interview_video_home.jpg" alt="Interview with Prof. Ravi Srivastava"/>
</a>
<!--
<iframe width="250" height="200" src="https://www.youtube.com/embed/MmaTlntk-wc" frameborder="0" allow="accelerometer; autoplay; encrypted-media; gyroscope; picture-in-picture" allowfullscreen=""></iframe>-->
</p>
<a href="https://im4change.in/videogallery" class="more-link CatArchalAnch1" target="_blank">
More videos
</a>
</div>
</div>
<div class="rightsmlbox1">
<div>
<!--div id="sstory" class="rightboxicons"></div--->
<p class="rightsmlbox1_title"><a href="https://im4change.in/list-success-stories" target="_blank">Success Stories</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/interviews" target="_blank">Interviews</a>
</p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a href="https://www.commoncause.in/page.php?id=10" >Donate</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/marquee"
class="isf_link more-link" title="India Focus?" style="border: 4px solid #fdd922;width: 90%;background-color: #fdd922;text-align: center;color: #000000;font-size:18px" target="_blank">India Focus</a></p> </div>
</div>
<div class="rightsmlbox1" style="height: 104px !important;">
<a href="https://im4change.in/quarterly_reports.php" target="_blank">
Quarterly Reports on Effect of Economic Slowdown on Employment in India (2008 - 2015)
</a>
</div>
<!-- <div class="rightsmlbox1">
<a href="https://play.google.com/store/apps/details?id=com.im4.im4change" target="_blank">
</a></div> -->
<!-- <section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">Most Visited</h2>
</section> -->
<!-- accordion Starts here -->
<!-- <div id="accordion" class="accordMarg">
</div> -->
<!-- accordion ends here -->
<!-- Widget Tag Cloud Starts here -->
<div id="tag_cloud-2" class="widget widget_tag_cloud">
<section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">MOST VISITED TAGS</h2>
</section>
<div class="widget-top wiPdTp">
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<div class="tagcloud">
<a href="https://im4change.in/search?qryStr=Agriculture"
target="_blank" class="tag-link-4 font4">Agriculture</a>
<a href="https://im4change.in/search?qryStr=Food Security"
target="_blank" class="tag-link-4 font4">Food Security</a>
<a href="https://im4change.in/search?qryStr=Law and Justice"
target="_blank" class="tag-link-4 font4">Law and Justice</a>
<a href="https://im4change.in/search?qryStr=Health"
target="_blank" class="tag-link-4 font4">Health</a>
<a href="https://im4change.in/search?qryStr=Right to Food"
target="_blank" class="tag-link-4 font4">Right to Food</a>
<a href="https://im4change.in/search?qryStr=Corruption"
target="_blank" class="tag-link-4 font4">Corruption</a>
<a href="https://im4change.in/search?qryStr=farming"
target="_blank" class="tag-link-4 font4">farming</a>
<a href="https://im4change.in/search?qryStr=Environment"
target="_blank" class="tag-link-4 font4">Environment</a>
<a href="https://im4change.in/search?qryStr=Right to Information"
target="_blank" class="tag-link-4 font4">Right to Information</a>
<a href="https://im4change.in/search?qryStr=NREGS"
target="_blank" class="tag-link-4 font4">NREGS</a>
<a href="https://im4change.in/search?qryStr=Human Rights"
target="_blank" class="tag-link-4 font4">Human Rights</a>
<a href="https://im4change.in/search?qryStr=Governance"
target="_blank" class="tag-link-4 font4">Governance</a>
<a href="https://im4change.in/search?qryStr=PDS"
target="_blank" class="tag-link-4 font4">PDS</a>
<a href="https://im4change.in/search?qryStr=COVID-19"
target="_blank" class="tag-link-4 font4">COVID-19</a>
<a href="https://im4change.in/search?qryStr=Land Acquisition"
target="_blank" class="tag-link-4 font4">Land Acquisition</a>
<a href="https://im4change.in/search?qryStr=mgnrega"
target="_blank" class="tag-link-4 font4">mgnrega</a>
<a href="https://im4change.in/search?qryStr=Farmers"
target="_blank" class="tag-link-4 font4">Farmers</a>
<a href="https://im4change.in/search?qryStr=transparency"
target="_blank" class="tag-link-4 font4">transparency</a>
<a href="https://im4change.in/search?qryStr=Gender"
target="_blank" class="tag-link-4 font4">Gender</a>
<a href="https://im4change.in/search?qryStr=Poverty"
target="_blank" class="tag-link-4 font4">Poverty</a>
<a href="https://im4change.in/search?qryStr=Farm Laws" target="_blank" class="tag-link-4 font4">Farm Laws
</a>
<a href="https://im4change.in/search?qryStr=Citizenship Amendment Act" target="_blank" class="tag-link-4 font4">Citizenship Amendment Act
</a>
<a href="https://im4change.in/search?qryStr=CAA NPR NRIC" target="_blank" class="tag-link-4 font4">CAA NPR NRIC
</a>
<a href="https://im4change.in/search?qryStr=Job Losses" target="_blank" class="tag-link-4 font4">Job Losses
</a>
<a href="https://im4change.in/search?qryStr=Migrant Workers" target="_blank" class="tag-link-4 font4">Migrant Workers
</a>
<a href="https://im4change.in/search?qryStr=Unemployment" target="_blank" class="tag-link-4 font4">Unemployment
</a>
<a href="https://im4change.in/search?qryStr=PMGKAY" target="_blank" class="tag-link-4 font4">PMGKAY
</a>
<a href="https://im4change.in/search?qryStr=PM-KISAN" target="_blank" class="tag-link-4 font4">PM-KISAN
</a>
<a href="https://im4change.in/search?qryStr=PM-CARES" target="_blank" class="tag-link-4 font4">PM-CARES
</a>
<a href="https://im4change.in/search?qryStr=LFPR" target="_blank" class="tag-link-4 font4">LFPR
</a>
</div>
</div>
</div>
<!-- Widget Tag Cloud Ends here -->
</aside>
<!-- Right Side Section End -->
</div>
<section class="cat-box cats-review-box footerSec">
<h2 class="cat-box-title vSec CatArcha">Video
Archives</h2>
<h2 class="cat-box-title CatArchaTitle">Archives</h2>
<div class="cat-box-content">
<div class="reviews-cat">
<div class="CatArchaDiv1">
<div class="CatArchaDiv2">
<ul>
<li>
<a href="https://im4change.in/news-alerts-57/moving-upstream-luni-fellowship.html" target="_blank">
Moving Upstream: Luni – Fellowship </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/135-million-indians-exited-multidimensional-poverty-as-per-government-figures-is-that-the-same-as-poverty-reduction.html" target="_blank">
135 Million Indians Exited “Multidimensional" Poverty as per Government... </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/explainer-why-are-tomato-prices-on-fire.html" target="_blank">
Explainer: Why are Tomato Prices on Fire? </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/nsso-survey-only-39-1-of-all-households-have-drinking-water-within-dwelling-46-7-of-rural-households-use-firewood-for-cooking.html" target="_blank">
NSSO Survey: Only 39.1% of all Households have Drinking... </a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/news-alerts-57"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/I51LYnP8BOk/1.jpg"
alt=" Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Short-Video-on-im4change-Hindi-website-Inclusive-Media-for-Change" target="_blank">
Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/kNqha-SwfIY/1.jpg"
alt=" "Session 1: Scope of IDEA and AgriStack" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-1- Scope-of-IDEA-and-AgriStack-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 1: Scope of IDEA and AgriStack" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/6kIVjlgZItk/1.jpg"
alt=" "Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-2-Farmer-Centric-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/2BeHTu0y7xc/1.jpg"
alt=" "Session 3: Future of Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-3-Future-of-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 3: Future of Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="divWidth">
<ul class="divWidthMarg">
<li>
<a href="https://im4change.in/video/Public-Spending-on-Agriculture-in-India-Source-Foundation-for-Agrarian-Studies"
title="Public Spending on Agriculture in India (Source: Foundation for Agrarian Studies)" target="_blank">
Public Spending on Agriculture in India (Source: Foundation for...</a>
</li>
<li>
<a href="https://im4change.in/video/Agrarian-Change-Seminar-Protests-against-the-New-Farm-Laws-in-India-by-Prof-Vikas-Rawal-JNU-Source-Journal-Of-Agrarian-Change"
title="Agrarian Change Seminar: 'Protests against the New Farm Laws in India' by Prof. Vikas Rawal, JNU (Source: Journal Of Agrarian Change) " target="_blank">
Agrarian Change Seminar: 'Protests against the New Farm Laws...</a>
</li>
<li>
<a href="https://im4change.in/video/Webinar-Ramrao-The-Story-of-India-Farm-Crisis-Source-Azim-Premji-University"
title="Webinar: Ramrao - The Story of India's Farm Crisis (Source: Azim Premji University)" target="_blank">
Webinar: Ramrao - The Story of India's Farm Crisis...</a>
</li>
<li>
<a href="https://im4change.in/video/water-and-agricultural-transformation-in-India"
title="Water and Agricultural Transformation in India: A Symbiotic Relationship (Source: IGIDR)" target="_blank">
Water and Agricultural Transformation in India: A Symbiotic Relationship...</a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/videogallery"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
</div>
</div>
</div>
</section> </div>
<div class="clear"></div>
<!-- Footer option Starts here -->
<div class="footer-bottom fade-in animated4">
<div class="container">
<div class="social-icons icon_flat">
<p class="SocialMargTop"> Website Developed by <a target="_blank" title="Web Development"
class="wot right"
href="http://www.ravinderkhurana.com/" rel="nofollow">
RAVINDErkHURANA.com</a></p>
</div>
<div class="alignleft">
<a
target="_blank" href="https://im4change.in/objectives-8.html"
class="link"
title="Objectives">Objectives</a> | <a
target="_blank" href="https://im4change.in/about-us-9.html"
class="link" title="About Us">About Us</a> | <a
target="_blank" href="https://im4change.in/media-workshops.php"
class="ucwords">Workshops</a> | <a
target="_blank" href="https://im4change.in/disclaimer/disclaimer-149.html"
title="Disclaimer">Disclaimer</a> </div>
</div>
</div>
<!-- Footer option ends here -->
</div>
<div id="connect">
<a target="_blank"
href="http://www.facebook.com/sharer.php?u=https://im4change.in/latest-news-updates/80-of-medicines-not-covered-by-price-control-order-rema-nagarajan-23504.html"
title="Share on Facebook">
<img src="https://im4change.in/images/Facebook.png?1582080640" alt="share on Facebook" class="ImgBorder"/>
</a><br/>
<a target="_blank"
href="http://twitter.com/share?text=Im4change&url=https://im4change.in/latest-news-updates/80-of-medicines-not-covered-by-price-control-order-rema-nagarajan-23504.html"
title="Share on Twitter">
<img src="https://im4change.in/images/twitter.png?1582080632" alt="Twitter" class="ImgBorder"/> </a>
<br/>
<a href="/feeds" title="RSS Feed" target="_blank">
<img src="https://im4change.in/images/rss.png?1582080632" alt="RSS" class="ImgBorder"/>
</a>
<br/>
<a class="feedback-link" id="feedbackFormLink" href="#">
<img src="https://im4change.in/images/feedback.png?1582080630" alt="Feedback" class="ImgBorder"/>
</a> <br/>
<a href="javascript:function iprl5(){var d=document,z=d.createElement('scr'+'ipt'),b=d.body,l=d.location;try{if(!b)throw(0);d.title='(Saving...) '+d.title;z.setAttribute('src',l.protocol+'//www.instapaper.com/j/WKrH3R7ORD5p?u='+encodeURIComponent(l.href)+'&t='+(new Date().getTime()));b.appendChild(z);}catch(e){alert('Please wait until the page has loaded.');}}iprl5();void(0)"
class="bookmarklet" onclick="return explain_bookmarklet();">
<img src="https://im4change.in/images/read-it-later.png?1582080632" alt="Read Later" class="ImgBorder"/> </a>
</div>
<!-- Feedback form Starts here -->
<div id="feedbackForm" class="overlay_form" class="ImgBorder">
<h2>Contact Form</h2>
<div id="contactform1">
<div id="formleft">
<form id="submitform" action="/contactus.php" method="post">
<input type="hidden" name="submitform" value="submitform"/>
<input type="hidden" name="salt_key" value="a0e0f2c6a0644a70e57ad2c96829709a"/>
<input type="hidden" name="ref" value="feedback"/>
<fieldset>
<label>Name :</label>
<input type="text" name="name" class="tbox" required/>
</fieldset>
<fieldset>
<label>Email :</label>
<input type="text" name="email" class="tbox" required/>
</fieldset>
<fieldset>
<label>Message :</label>
<textarea rows="5" cols="20" name="message" required></textarea>
</fieldset>
<fieldset>
Please enter security code
<div class="clear"></div>
<input type="text" name="vrcode" class="tbox"/>
</fieldset>
<fieldset>
<input type="submit" class="button" value="Submit"/>
<a href="#" id="closefeedbakcformLink">Close</a>
</fieldset>
</form>
</div>
<div class="clearfix"></div>
</div>
</div>
<div id="donate_popup" class="modal" style="max-width: 800px;">
<table width="100%" border="1">
<tr>
<td colspan="2" align="center">
<b>Support im4change</b>
</td>
</tr>
<tr>
<td width="25%" valign="middle">
<img src="https://im4change.in/images/logo2.jpg?1582080632" alt="" width="100%"/> </td>
<td style="padding-left:10px;padding-top:10px;">
<form action="https://im4change.in/donate" method="get">
<table width="100%" cellpadding="2" cellspacing="2">
<tr>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
10
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
100
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
1000
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
50
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
500
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
<input type="text" name="price" placeholder="?" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td colspan="3" align="right">
<input type="button" name="Pay" value="Pay"
style="width: 200px;background-color: rgb(205, 35, 36);color: #ffffff;"/>
</td>
</tr>
</table>
</form>
</td>
</tr>
</table>
</div><script type='text/javascript'>
/* <![CDATA[ */
var tievar = {'go_to': 'Go to...'};
/* ]]> */
</script>
<script src="/js/tie-scripts.js?1575549704"></script><script src="/js/bootstrap.js?1575549704"></script><script src="/js/jquery.modal.min.js?1578284310"></script><script>
$(document).ready(function() {
// tell the autocomplete function to get its data from our php script
$('#s').autocomplete({
source: "/autocomplete"
});
});
</script>
<script src="/vj-main-sw-register.js" async></script>
<script>function init(){var imgDefer=document.getElementsByTagName('img');for(var i=0;i<imgDefer.length;i++){if(imgDefer[i].getAttribute('data-src')){imgDefer[i].setAttribute('src',imgDefer[i].getAttribute('data-src'))}}}
window.onload=init;</script>
</body>
</html>'
}
$cookies = []
$values = [
(int) 0 => 'text/html; charset=UTF-8'
]
$name = 'Content-Type'
$first = true
$value = 'text/html; charset=UTF-8'
header - [internal], line ??
Cake\Http\ResponseEmitter::emitHeaders() - CORE/src/Http/ResponseEmitter.php, line 181
Cake\Http\ResponseEmitter::emit() - CORE/src/Http/ResponseEmitter.php, line 55
Cake\Http\Server::emit() - CORE/src/Http/Server.php, line 141
[main] - ROOT/webroot/index.php, line 39
LATEST NEWS UPDATES | 80% of medicines not covered by price control order -Rema Nagarajan
80% of medicines not covered by price control order -Rema Nagarajan
Published on Dec 1, 2013 Modified on Dec 1, 2013
-The Times of India
About 38 million people in India (which is more than Canada's population) fall below the poverty line every year due to healthcare expenses, of which 70% is on purchase of drugs. Yet, the much-awaited drug price control order (DPCO) 2013, meant to control the price of medicines does not cover over 80% of the medicines in the market. Many drugs crucial for India's disease profile have been left out, which means people are unlikely to see any significant reduction in expenditure on medicines.
In 2003, the Supreme Court, while hearing a case on the National Pharmaceutical Pricing Policy, had directed the government to formulate appropriate criteria to identify essential and life saving drugs and ensure that they came under price control. It took over a decade for the government to announce the DPCO in May 2013.
By the government's own admission in an affidavit filed in court, the market value and share of medicines covered by DPCO is just 18% of the country's pharma market. Many life-saving medicines including anti-cancer drugs, expensive antibiotics and drugs needed for organ transplantation have been left out.
The government merely lifted the entire National List of Essential Medicines (NLEM) 2011, comprising 348 medicines, and placed it under price control. "The literal translation of the NLEM into DPCO 2103 has been done without a thought of its implications. The companies have been provided a convenient escape route. A 500 mg Paracetamol tablet is under price control but its 650 mg strength is not; individual anti-TB drugs are under price control but their combinations which outsell single ingredient preparations are not. This undermines the entire objective of making essential medicines more affordable to Indians," explained Dr Anurag Bhargava, associate professor at the Himalayan Institute of Medical Sciences. He stressed the need to expand the scope of price control to include all dosages and combinations, as was the case in the previous DPCO of 1995.
With the current DPCO not covering combinations of drugs, a lot of drugs for diabetes and hypertension and many other conditions will move out of price control as they are used in combination. The combinations not covered under NLEM account for Rs 31,866 crore or almost 45% of the total pharma market of Rs 71,246 crore in 2012.
An independent evaluation of the National Pharmaceutical Pricing Policy, by the Public Health Foundation of India (PHFI) and the Institute for Studies in Industrial Development (ISID) for a forthcoming report explains why it is important to expand the scope of price control. According to their evaluation, the market value of anti-infectives under price control is Rs 4,636 crore, just 6.5% of the total market. Anti-infectives, which include antibiotics, have the biggest chunk of India's pharma market.
"Our evaluation shows that if price control was expanded to combinations, additional strengths and dosages of just the anti-infectives included in the NLEM, the total market value would be worth more than Rs 10,500 crore, about 15% of the total pharma market, a vast improvement over the current coverage of just 6.5%," said Malini Aisola of PHFI.
The essential medicines list does not seem to have taken into account India's disease profile as it leaves out several drugs crucial for treating many common conditions, pointed out Dr Bhargava. The government's own affidavit admits that only 18% of anti-diabetics, 19% of anti-TB medicines and 6% of the respiratory therapeutics segment are under price control. This is despite India being the diabetes and TB capital of the world, and facing high prevalence of asthma and chronic obstructive pulmonary disease (COPD).
There's good reason why we need price controls. The MRP charged by companies is often many times the cost of production leaving them with profit margins unheard of in any other sector. Price control was meant to address this problem, particularly in medicines important for India. But it has failed to make any significant difference.
One reason is the way prices are determined under the current DPCO. Under the 1995 DPCO, the drugs prices under controls was decided by taking the cost of manufacture and fixing a certain percentage as mark-up, which included packaging and distribution costs, retailers' margin, excise duty and profit. But the current DPCO uses a new formula under which the price is fixed by taking the average price of brands having one per cent or more of market share and adding 16% as retail margin.
S Srinivasan of LOCOST, a company producing drugs for use by NGOs to treat the poor, explained how the cost of manufacture, including retail margin, for Cetrizine, an anti-allergic, is just Rs 1.20 for ten tablets. The ceiling price under the DPCO is Rs 18.10, the same as the price charged by the market leader GSK. This allows a price that is 15 times the cost of manufacture. In the case of Albendazole, a drug used to treat worm infections, the cost of manufacture including retail margin is Rs 8.50 per 10 tablets, while the DPCO ceiling price is over Rs 91, a ten-fold mark-up, pointed out Srinivasan. The price charged by the market leader in Albendazole, GSK, was Rs 140 per ten tablets. In this case, while price control should bring down the market leader's price, it still allows a huge profit margin. In fact, the PHFI-ISID evaluation shows that in 43% of drugs studied, the sales leader will face little or no impact from price control.
To show how effective DPCO has been, the government has compared the price reductions due to DPCO with the highest price of a drug. However, PHFI and ISID point out, it makes more sense to use the price charged by the company with the highest market share for comparison. Out of the 390 formulations for which prices have been notified, in 212 the company with the highest sales does not have the highest price. So, the price reduction achieved by DPCO is nowhere as dramatic as claimed by the government. PHFI and ISID have conducted an independent analysis using the same data as used by the government. Their calculation for 369 formulations shows that the effective average price reduction would be just 11% and the impact on the pharma market as a whole would be a mere 1.8%.
In sum, coming in 2013, a decade after the Supreme Court asked for it, the DPCO is clearly late. But even worse, as the PHFI-ISID study reveals, it is too little. Given how much rides on this for the aam aadmi, that is a tragedy of mammoth proportions.About 38 million people in India (which is more than Canada's population) fall below the poverty line every year due to healthcare expenses, of which 70% is on purchase of drugs. Yet, the much-awaited drug price control order (DPCO) 2013, meant to control the price of medicines does not cover over 80% of the medicines in the market. Many drugs crucial for India's disease profile have been left out, which means people are unlikely to see any significant reduction in expenditure on medicines.
In 2003, the Supreme Court, while hearing a case on the National Pharmaceutical Pricing Policy, had directed the government to formulate appropriate criteria to identify essential and life saving drugs and ensure that they came under price control. It took over a decade for the government to announce the DPCO in May 2013.
By the government's own admission in an affidavit filed in court, the market value and share of medicines covered by DPCO is just 18% of the country's pharma market. Many life-saving medicines including anti-cancer drugs, expensive antibiotics and drugs needed for organ transplantation have been left out.
The government merely lifted the entire National List of Essential Medicines (NLEM) 2011, comprising 348 medicines, and placed it under price control. "The literal translation of the NLEM into DPCO 2103 has been done without a thought of its implications. The companies have been provided a convenient escape route. A 500 mg Paracetamol tablet is under price control but its 650 mg strength is not; individual anti-TB drugs are under price control but their combinations which outsell single ingredient preparations are not. This undermines the entire objective of making essential medicines more affordable to Indians," explained Dr Anurag Bhargava, associate professor at the Himalayan Institute of Medical Sciences. He stressed the need to expand the scope of price control to include all dosages and combinations, as was the case in the previous DPCO of 1995.
With the current DPCO not covering combinations of drugs, a lot of drugs for diabetes and hypertension and many other conditions will move out of price control as they are used in combination. The combinations not covered under NLEM account for Rs 31,866 crore or almost 45% of the total pharma market of Rs 71,246 crore in 2012.
An independent evaluation of the National Pharmaceutical Pricing Policy, by the Public Health Foundation of India (PHFI) and the Institute for Studies in Industrial Development (ISID) for a forthcoming report explains why it is important to expand the scope of price control. According to their evaluation, the market value of anti-infectives under price control is Rs 4,636 crore, just 6.5% of the total market. Anti-infectives, which include antibiotics, have the biggest chunk of India's pharma market.
"Our evaluation shows that if price control was expanded to combinations, additional strengths and dosages of just the anti-infectives included in the NLEM, the total market value would be worth more than Rs 10,500 crore, about 15% of the total pharma market, a vast improvement over the current coverage of just 6.5%," said Malini Aisola of PHFI.
The essential medicines list does not seem to have taken into account India's disease profile as it leaves out several drugs crucial for treating many common conditions, pointed out Dr Bhargava. The government's own affidavit admits that only 18% of anti-diabetics, 19% of anti-TB medicines and 6% of the respiratory therapeutics segment are under price control. This is despite India being the diabetes and TB capital of the world, and facing high prevalence of asthma and chronic obstructive pulmonary disease (COPD).
There's good reason why we need price controls. The MRP charged by companies is often many times the cost of production leaving them with profit margins unheard of in any other sector. Price control was meant to address this problem, particularly in medicines important for India. But it has failed to make any significant difference.
One reason is the way prices are determined under the current DPCO. Under the 1995 DPCO, the drugs prices under controls was decided by taking the cost of manufacture and fixing a certain percentage as mark-up, which included packaging and distribution costs, retailers' margin, excise duty and profit. But the current DPCO uses a new formula under which the price is fixed by taking the average price of brands having one per cent or more of market share and adding 16% as retail margin.
S Srinivasan of LOCOST, a company producing drugs for use by NGOs to treat the poor, explained how the cost of manufacture, including retail margin, for Cetrizine, an anti-allergic, is just Rs 1.20 for ten tablets. The ceiling price under the DPCO is Rs 18.10, the same as the price charged by the market leader GSK. This allows a price that is 15 times the cost of manufacture. In the case of Albendazole, a drug used to treat worm infections, the cost of manufacture including retail margin is Rs 8.50 per 10 tablets, while the DPCO ceiling price is over Rs 91, a ten-fold mark-up, pointed out Srinivasan. The price charged by the market leader in Albendazole, GSK, was Rs 140 per ten tablets. In this case, while price control should bring down the market leader's price, it still allows a huge profit margin. In fact, the PHFI-ISID evaluation shows that in 43% of drugs studied, the sales leader will face little or no impact from price control.
To show how effective DPCO has been, the government has compared the price reductions due to DPCO with the highest price of a drug. However, PHFI and ISID point out, it makes more sense to use the price charged by the company with the highest market share for comparison. Out of the 390 formulations for which prices have been notified, in 212 the company with the highest sales does not have the highest price. So, the price reduction achieved by DPCO is nowhere as dramatic as claimed by the government. PHFI and ISID have conducted an independent analysis using the same data as used by the government. Their calculation for 369 formulations shows that the effective average price reduction would be just 11% and the impact on the pharma market as a whole would be a mere 1.8%.
In sum, coming in 2013, a decade after the Supreme Court asked for it, the DPCO is clearly late. But even worse, as the PHFI-ISID study reveals, it is too little. Given how much rides on this for the aam aadmi, that is a tragedy of mammoth proportions.
 Published on Dec 1, 2013
Published on Dec 1, 2013
 Modified on Dec 1, 2013
Modified on Dec 1, 2013
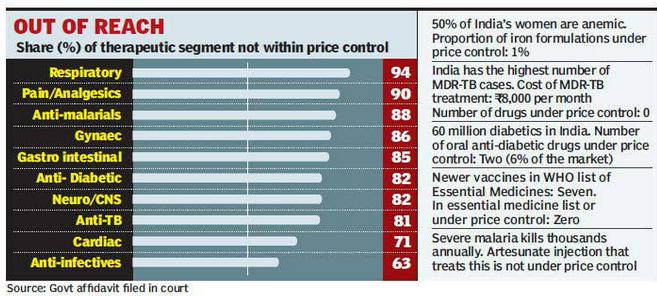









Write Comments