Deprecated (16384): The ArrayAccess methods will be removed in 4.0.0.Use getParam(), getData() and getQuery() instead. - /home/brlfuser/public_html/src/Controller/ArtileDetailController.php, line: 150
You can disable deprecation warnings by setting `Error.errorLevel` to `E_ALL & ~E_USER_DEPRECATED` in your config/app.php. [CORE/src/Core/functions.php, line 311]
deprecationWarning - CORE/src/Core/functions.php, line 311
Cake\Http\ServerRequest::offsetGet() - CORE/src/Http/ServerRequest.php, line 2421
App\Controller\ArtileDetailController::index() - APP/Controller/ArtileDetailController.php, line 150
Cake\Controller\Controller::invokeAction() - CORE/src/Controller/Controller.php, line 610
Cake\Http\ActionDispatcher::_invoke() - CORE/src/Http/ActionDispatcher.php, line 120
Cake\Http\ActionDispatcher::dispatch() - CORE/src/Http/ActionDispatcher.php, line 94
Cake\Http\BaseApplication::__invoke() - CORE/src/Http/BaseApplication.php, line 235
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Routing\Middleware\RoutingMiddleware::__invoke() - CORE/src/Routing/Middleware/RoutingMiddleware.php, line 162
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Routing\Middleware\AssetMiddleware::__invoke() - CORE/src/Routing/Middleware/AssetMiddleware.php, line 97
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Error\Middleware\ErrorHandlerMiddleware::__invoke() - CORE/src/Error/Middleware/ErrorHandlerMiddleware.php, line 96
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Http\Runner::run() - CORE/src/Http/Runner.php, line 51
Cake\Http\Server::run() - CORE/src/Http/Server.php, line 98
Deprecated (16384): The ArrayAccess methods will be removed in 4.0.0.Use getParam(), getData() and getQuery() instead. - /home/brlfuser/public_html/src/Controller/ArtileDetailController.php, line: 151
You can disable deprecation warnings by setting `Error.errorLevel` to `E_ALL & ~E_USER_DEPRECATED` in your config/app.php. [CORE/src/Core/functions.php, line 311]
deprecationWarning - CORE/src/Core/functions.php, line 311
Cake\Http\ServerRequest::offsetGet() - CORE/src/Http/ServerRequest.php, line 2421
App\Controller\ArtileDetailController::index() - APP/Controller/ArtileDetailController.php, line 151
Cake\Controller\Controller::invokeAction() - CORE/src/Controller/Controller.php, line 610
Cake\Http\ActionDispatcher::_invoke() - CORE/src/Http/ActionDispatcher.php, line 120
Cake\Http\ActionDispatcher::dispatch() - CORE/src/Http/ActionDispatcher.php, line 94
Cake\Http\BaseApplication::__invoke() - CORE/src/Http/BaseApplication.php, line 235
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Routing\Middleware\RoutingMiddleware::__invoke() - CORE/src/Routing/Middleware/RoutingMiddleware.php, line 162
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Routing\Middleware\AssetMiddleware::__invoke() - CORE/src/Routing/Middleware/AssetMiddleware.php, line 97
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Error\Middleware\ErrorHandlerMiddleware::__invoke() - CORE/src/Error/Middleware/ErrorHandlerMiddleware.php, line 96
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Http\Runner::run() - CORE/src/Http/Runner.php, line 51
Cake\Http\Server::run() - CORE/src/Http/Server.php, line 98
Warning (512): Unable to emit headers. Headers sent in file=/home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php line=853 [CORE/src/Http/ResponseEmitter.php, line 48]
if (Configure::read('debug')) {
trigger_error($message, E_USER_WARNING);
} else {
$response = object(Cake\Http\Response) {
'status' => (int) 200,
'contentType' => 'text/html',
'headers' => [
'Content-Type' => [
[maximum depth reached]
]
],
'file' => null,
'fileRange' => [],
'cookies' => object(Cake\Http\Cookie\CookieCollection) {},
'cacheDirectives' => [],
'body' => '<!DOCTYPE html>
<!--[if lt IE 7 ]>
<html class="ie ie6" lang='en'> <![endif]-->
<!--[if IE 7 ]>
<html class="ie ie7" lang='en'> <![endif]-->
<!--[if IE 8 ]>
<html class="ie ie8" lang='en'> <![endif]-->
<!--[if (gte IE 9)|!(IE)]><!-->
<html lang='en'>
<!--<![endif]-->
<head><meta http-equiv="Content-Type" content="text/html; charset=utf-8">
<title>
LATEST NEWS UPDATES | Delivering safety -Kundan Pandey </title>
<meta name="description" content="
-Down to Earth
All safe motherhood programmes of the government are focused on institutional deliveries, but health centres are in disarray. Experts suggest ways to reduce deaths during delivery
Lal Mohan, a daily wage labourer, has no clue what took his wife's..."/>
<meta name="keywords" content="maternal mortality ratio,maternal deaths,Health,maternal mortality,Maternal Health,hospitals"/>
<meta name="news_keywords" content="maternal mortality ratio,maternal deaths,Health,maternal mortality,Maternal Health,hospitals">
<link rel="alternate" type="application/rss+xml" title="ROR" href="/ror.xml"/>
<link rel="alternate" type="application/rss+xml" title="RSS 2.0" href="/feeds/"/>
<link rel="stylesheet" href="/css/bootstrap.min.css?1697864993"/> <link rel="stylesheet" href="/css/style.css?v=1.1.2"/> <link rel="stylesheet" href="/css/style-inner.css?1577045210"/> <link rel="stylesheet" id="Oswald-css"
href="https://fonts.googleapis.com/css?family=Oswald%3Aregular%2C700&ver=3.8.1" type="text/css"
media="all">
<link rel="stylesheet" href="/css/jquery.modal.min.css?1578285302"/> <script src="/js/jquery-1.10.2.js?1575549704"></script> <script src="/js/jquery-migrate.min.js?1575549704"></script> <link rel="shortcut icon" href="/favicon.ico" title="Favicon">
<link rel="stylesheet" href="/css/jquery-ui.css?1580720609"/> <script src="/js/jquery-ui.js?1575549704"></script> <link rel="preload" as="style" href="https://www.im4change.org/css/custom.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery.modal.min.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery-ui.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/li-scroller.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<!-- <link rel="preload" as="style" href="https://www.im4change.org/css/style.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous"> -->
<link rel="preload" as="style" href="https://www.im4change.org/css/style-inner.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel='dns-prefetch' href="//im4change.org/css/custom.css" crossorigin >
<link rel="preload" as="script" href="https://www.im4change.org/js/bootstrap.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.li-scroller.1.0.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.modal.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.ui.totop.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-1.10.2.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-migrate.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-ui.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/setting.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/tie-scripts.js">
<!--[if IE]>
<script type="text/javascript">jQuery(document).ready(function () {
jQuery(".menu-item").has("ul").children("a").attr("aria-haspopup", "true");
});</script>
<![endif]-->
<!--[if lt IE 9]>
<script src="/js/html5.js"></script>
<script src="/js/selectivizr-min.js"></script>
<![endif]-->
<!--[if IE 8]>
<link rel="stylesheet" type="text/css" media="all" href="/css/ie8.css"/>
<![endif]-->
<meta property="og:title" content="LATEST NEWS UPDATES | Delivering safety -Kundan Pandey" />
<meta property="og:url" content="https://im4change.in/latest-news-updates/delivering-safety-kundan-pandey-24858.html" />
<meta property="og:type" content="article" />
<meta property="og:description" content="
-Down to Earth
All safe motherhood programmes of the government are focused on institutional deliveries, but health centres are in disarray. Experts suggest ways to reduce deaths during delivery
Lal Mohan, a daily wage labourer, has no clue what took his wife's..." />
<meta property="og:image" content="" />
<meta property="fb:app_id" content="0" />
<meta name="viewport" content="width=device-width, initial-scale=1, maximum-scale=1, user-scalable=no">
<link rel="apple-touch-icon-precomposed" sizes="144x144" href="https://im4change.in/images/apple1.png">
<link rel="apple-touch-icon-precomposed" sizes="120x120" href="https://im4change.in/images/apple2.png">
<link rel="apple-touch-icon-precomposed" sizes="72x72" href="https://im4change.in/images/apple3.png">
<link rel="apple-touch-icon-precomposed" href="https://im4change.in/images/apple4.png">
<style>
.gsc-results-wrapper-overlay{
top: 38% !important;
height: 50% !important;
}
.gsc-search-button-v2{
border-color: #035588 !important;
background-color: #035588 !important;
}
.gsib_a{
height: 30px !important;
padding: 2px 8px 1px 6px !important;
}
.gsc-search-button-v2{
height: 41px !important;
}
input.gsc-input{
background: none !important;
}
@media only screen and (max-width: 600px) {
.gsc-results-wrapper-overlay{
top: 11% !important;
width: 87% !important;
left: 9% !important;
height: 43% !important;
}
.gsc-search-button-v2{
padding: 10px 10px !important;
}
.gsc-input-box{
height: 28px !important;
}
/* .gsib_a {
padding: 0px 9px 4px 9px !important;
}*/
}
@media only screen and (min-width: 1200px) and (max-width: 1920px) {
table.gsc-search-box{
width: 15% !important;
float: right !important;
margin-top: -118px !important;
}
.gsc-search-button-v2 {
padding: 6px !important;
}
}
</style>
<script>
$(function () {
$("#accordion").accordion({
event: "click hoverintent"
});
});
/*
* hoverIntent | Copyright 2011 Brian Cherne
* http://cherne.net/brian/resources/jquery.hoverIntent.html
* modified by the jQuery UI team
*/
$.event.special.hoverintent = {
setup: function () {
$(this).bind("mouseover", jQuery.event.special.hoverintent.handler);
},
teardown: function () {
$(this).unbind("mouseover", jQuery.event.special.hoverintent.handler);
},
handler: function (event) {
var currentX, currentY, timeout,
args = arguments,
target = $(event.target),
previousX = event.pageX,
previousY = event.pageY;
function track(event) {
currentX = event.pageX;
currentY = event.pageY;
}
;
function clear() {
target
.unbind("mousemove", track)
.unbind("mouseout", clear);
clearTimeout(timeout);
}
function handler() {
var prop,
orig = event;
if ((Math.abs(previousX - currentX) +
Math.abs(previousY - currentY)) < 7) {
clear();
event = $.Event("hoverintent");
for (prop in orig) {
if (!(prop in event)) {
event[prop] = orig[prop];
}
}
// Prevent accessing the original event since the new event
// is fired asynchronously and the old event is no longer
// usable (#6028)
delete event.originalEvent;
target.trigger(event);
} else {
previousX = currentX;
previousY = currentY;
timeout = setTimeout(handler, 100);
}
}
timeout = setTimeout(handler, 100);
target.bind({
mousemove: track,
mouseout: clear
});
}
};
</script>
<script type="text/javascript">
var _gaq = _gaq || [];
_gaq.push(['_setAccount', 'UA-472075-3']);
_gaq.push(['_trackPageview']);
(function () {
var ga = document.createElement('script');
ga.type = 'text/javascript';
ga.async = true;
ga.src = ('https:' == document.location.protocol ? 'https://ssl' : 'http://www') + '.google-analytics.com/ga.js';
var s = document.getElementsByTagName('script')[0];
s.parentNode.insertBefore(ga, s);
})();
</script>
<link rel="stylesheet" href="/css/custom.css?v=1.16"/> <script src="/js/jquery.ui.totop.js?1575549704"></script> <script src="/js/setting.js?1575549704"></script> <link rel="manifest" href="/manifest.json">
<meta name="theme-color" content="#616163" />
<meta name="apple-mobile-web-app-capable" content="yes">
<meta name="apple-mobile-web-app-status-bar-style" content="black">
<meta name="apple-mobile-web-app-title" content="im4change">
<link rel="apple-touch-icon" href="/icons/logo-192x192.png">
</head>
<body id="top" class="home inner blog">
<div class="background-cover"></div>
<div class="wrapper animated">
<header id="theme-header" class="header_inner" style="position: relative;">
<div class="logo inner_logo" style="left:20px !important">
<a title="Home" href="https://im4change.in/">
<img src="https://im4change.in/images/logo2.jpg?1582080632" class="logo_image" alt="im4change"/> </a>
</div>
<div class="langhindi" style="color: #000;display:none;"
href="https://im4change.in/">
<a class="more-link" href="https://im4change.in/">Home</a>
<a href="https://im4change.in/hindi/" class="langbutton ">हिन्दी</a>
</div>
<nav class="fade-in animated2" id="main-nav">
<div class="container">
<div class="main-menu">
<ul class="menu" id="menu-main">
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
style="left: -40px;"><a
target="_blank" href="https://im4change.in/">Home</a>
</li>
<li class="menu-item mega-menu menu-item-type-taxonomy mega-menu menu-item-object-category mega-menu menu-item-has-children parent-list"
style=" margin-left: -40px;"><a href="#">KNOWLEDGE GATEWAY <span class="sub-indicator"></span>
</a>
<div class="mega-menu-block background_menu" style="padding-top:25px;">
<div class="container">
<div class="mega-menu-content">
<div class="mega-menu-item">
<h3><b>Farm Crisis</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/farmers039-suicides-14.html"
class="left postionrel">Farm Suicides </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/unemployment-30.html"
class="left postionrel">Unemployment </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/rural-distress-70.html"
class="left postionrel">Rural distress </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/migration-34.html"
class="left postionrel">Migration </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/key-facts-72.html"
class="left postionrel">Key Facts </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/debt-trap-15.html"
class="left postionrel">Debt Trap </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Empowerment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/union-budget-73.html"
class="left postionrel">Union Budget And Other Economic Policies </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/forest-and-tribal-rights-61.html"
class="left postionrel">Forest and Tribal Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-education-60.html"
class="left postionrel">Right to Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-food-59.html"
class="left postionrel">Right to Food </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/displacement-3279.html"
class="left postionrel">Displacement </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-work-mg-nrega-39.html"
class="left postionrel">Right to Work (MG-NREGA) </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/gender-3280.html"
class="left postionrel">GENDER </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-information-58.html"
class="left postionrel">Right to Information </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/social-audit-48.html"
class="left postionrel">Social Audit </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Hunger / HDI</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/poverty-and-inequality-20499.html"
class="left postionrel">Poverty and inequality </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/malnutrition-41.html"
class="left postionrel">Malnutrition </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/public-health-51.html"
class="left postionrel">Public Health </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/education-50.html"
class="left postionrel">Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hunger-overview-40.html"
class="left postionrel">Hunger Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hdi-overview-45.html"
class="left postionrel">HDI Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/pds-ration-food-security-42.html"
class="left postionrel">PDS/ Ration/ Food Security </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/sdgs-113.html"
class="left postionrel">SDGs </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/mid-day-meal-scheme-mdms-53.html"
class="left postionrel">Mid Day Meal Scheme (MDMS) </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Environment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/time-bomb-ticking-52.html"
class="left postionrel">Time Bomb Ticking </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/water-and-sanitation-55.html"
class="left postionrel">Water and Sanitation </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/impact-on-agriculture-54.html"
class="left postionrel">Impact on Agriculture </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Law & Justice</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/social-justice-20500.html"
class="left postionrel">Social Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/access-to-justice-47.html"
class="left postionrel">Access to Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/human-rights-56.html"
class="left postionrel">Human Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/corruption-35.html"
class="left postionrel">Corruption </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/general-insecurity-46.html"
class="left postionrel">General Insecurity </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/disaster-relief-49.html"
class="left postionrel">Disaster & Relief </a>
</p>
</div>
</div>
</div>
</div>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page "><a target="_blank" href="https://im4change.in/nceus_reports.php">NCEUS reports</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children parent-list ">
<a target="_blank" href="https://im4change.in/about-us-9.html">About Us <span
class="sub-indicator"></span></a>
<ul class="sub-menu aboutmenu">
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/objectives-8.html">Objectives</a>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/contactus.php">Contact
Us</a></li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/about-us-9.html">About
Us</a></li>
</ul>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children ">
<a target="_blank" href="https://im4change.in/fellowships.php" title="Fellowships">Fellowships</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/media-workshops.php">Workshops</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/research.php">Research</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/links-64">Partners</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
id="menu-item-539"><a target="_blank" href="https://im4change.in/hindi/"
class="langbutton langlinkfont17">हिन्दी</a></li>
</ul>
</div> </div>
<!-- <div style="float: right;">
<script async src="https://cse.google.com/cse.js?cx=18b4f2e0f11bed3dd"></script>
<div class="gcse-search"></div>
</div> -->
<div class="search-block" style=" margin-left: 8px; margin-right: 7px;">
<form method="get" id="searchform" name="searchform"
action="https://im4change.in/search"
onsubmit="return searchvalidate();">
<button class="search-button" type="submit" value="Search"></button>
<input type="text" id="s" name="qryStr" value=""
onfocus="if (this.value == 'Search...') {this.value = '';}"
onblur="if (this.value == '') {this.value = 'Search...';}">
</form>
</div>
</nav>
</header>
<div class="container">
<div id="main-content" class=" main1 container fade-in animated3 sidebar-narrow-left">
<div class="content-wrap">
<div class="content" style="width: 900px;min-height: 500px;">
<section class="cat-box recent-box innerCatRecent">
<h1 class="cat-box-title">Delivering safety -Kundan Pandey</h1>
<a href="JavaScript:void(0);" onclick="return shareArticle(24677);">
<img src="https://im4change.in/images/email.png?1582080630" border="0" width="24" align="right" alt="Share this article"/> </a>
<a href="https://im4change.in/latest-news-updates/delivering-safety-kundan-pandey-24858/print"
rel="nofollow">
<img src="https://im4change.in/images/icon-print.png?1582080630" border="0" width="24" align="right" alt="Share this article"/>
</a>
</section>
<section class="recent-box innerCatRecent">
<small class="pb-1"><span class="dateIcn">
<img src="https://im4change.in/images/published.svg?1582080666" alt="published"/>
Published on</span><span class="text-date"> Apr 28, 2014</span>
<span
class="dateIcn">
<img src="https://im4change.in/images/modified.svg?1582080666" alt="modified"/> Modified on </span><span class="text-date"> Apr 28, 2014</span>
</small>
</section>
<div class="clear"></div>
<div style="padding-top: 10px;">
<div class="innerLineHeight">
<div class="middleContent innerInput latest-news-updates">
<table>
<tr>
<td>
<div>
<div style="text-align: justify">-Down to Earth</div><div style="text-align: justify"> </div><p style="text-align: justify"><em>All safe motherhood programmes of the government are focused on institutional deliveries, but health centres are in disarray. Experts suggest ways to reduce deaths during delivery</em></p><p style="text-align: justify">Lal Mohan, a daily wage labourer, has no clue what took his wife's life. Sarita Devi, 25, was expecting her third child, and was on way to a good hospital at Bhagalpur district in Bihar. "She was normal all through the nine months of pregnancy," he says. "When labour pains began, we took her to a community health centre (CHC), 15 km from our house in Godda district in Jharkhand. At around 11 pm, doctors advised us to take her to Sadar Hospital, 20 km from the CHC. Here again, doctors referred her to Jawaharlal Nehru Medical College and Hospital in Bhagalpur, another 70 km away." She passed away on the way to hospital.</p><p style="text-align: justify">Sarita's death is not a one-off case. In a year, hundreds of women die during or after pregnancy in the Santhal Pargana region, where Sarita lived. Child marriage is rampant in the region and girls usually become pregnant at the age of 16, says Soumik Bannerjee, health activist in Godda. Their undernourished bodies are ill-prepared for travelling to faraway places during labour pains, that too under no medical supervision or advise. Small wonder, Santhal Pargana has a high maternal mortality ratio (MMR), of more than 300 deaths per 100,000 live births, he says.</p><p style="text-align: justify">This is the result of the government's focus on only institutional deliveries, says Shakeel Ur Rehman of Bihar-based non-profit Centre for Health and Resource Management (CHARM). The government has based all its programmes for expecting mothers on the belief that women can be safe during and after childbirth only if they have access to public health institutions, he says. Programmes like Janani Suraksha Yojana even give cash incentives to women who deliver their babies in hospitals. It allocated as much as Rs 1,700 crore for the programme in 2011-12.</p><p style="text-align: justify">Though the country has been able to reduce its MMR from 212 in 2009 to 178 in 2012, it may not be able to achieve its Millennium Development Goal (MDG). In 2000, the international community had pledged to bring down MMR by one- third. For India, the target was to reduce MMR to 109 by 2015.</p><p style="text-align: justify">To overcome the challenge, member of the Planning Commission Syeda Hameed suggested National Alliance for Maternal Health and Human Rights and Oxfam (international confederation of organisations working to find solutions to social injustices) to present their recommendations to the plan panel. The organisations are now finalising the recommendations (see ‘Experts' recommendations'). The plan panel is set to do mid-term appraisal of the 12th Five Year Plan within a few months. Implementation of the recommendations should be able to reduce MMR, she said at a national convention held recently in New Delhi.</p><p style="text-align: justify">Reduction in the country's MMR is most likely because of under-reporting of deaths, says Rehman. CHARM is currently conducting a survey at public health centres in Bihar. The non-profit has found a big gap between government data and the actual MMR. Phulwari Sharif in Patna has reported zero deaths, but the non-profit found 14 deaths in the block in a month. "The focus is only on achieving targets on paper," he says.</p><p style="text-align: justify">At present, Assam has the highest MMR of 328 in the country followed by Uttar Pradesh and Uttarakhand together at 292, according to a recently released report of the Registrar General of India. Madhya Pradesh, Chhattisgarh, Odisha, Rajasthan, Bihar and Jharkhand have MMR of 200 and above. South India, however, has shown remarkable progress. Kerala has pushed its MMR down from 150 in 1997-98 to 66 in 2012. Tamil Nadu has reduced it from 131 to 90 and Andhra Pradesh from 197 to 110 in the same period (see ‘Meeting targets').</p><p style="text-align: justify"><img src="https://im4change.in/siteadmin/tinymce/uploaded/Down to Earth.jpg" alt="Down to Earth" width="458" height="350" /> </p><p style="text-align: justify"><em>Multi-pronged approach</em></p><p style="text-align: justify">"South Indian states improved their MMR because they have more or less sorted out issues like nutrition and hygiene, which have a big influence on safe delivery," says Ritu Priya Mehrotra, professor at the Centre of Social Medicine and Community Health, Jawaharlal Nehru University, Delhi. Public health system is strong in these states.</p><p style="text-align: justify">"It is strange that the government has initiated programmes focused on public health institutions without improving medical facilities and infrastructure there," says Abhijit Das, director of Centre for Health and Social Justice, a New Delhi-based non-profit. The need is to take a multi-pronged approach, says Smita Bajpai of Gujarat-based non-profit Centre for Health Education, Training and Nutrition Awareness. "Unless the focus shifts to the root cause of the problem, it will not be resolved. Improvement is required in every sector-transport, infrastructure, nutrition and employment," she adds.</p><p style="text-align: justify">A CHARM study on maternal deaths in Bihar found 22 deaths in Phulwari Sharif and Maner blocks between 2012 and 2013. Of these, 15 women died while being taken to health centres in autorickshaws. Two were on foot. Delay in decision-making and reaching health centres was the reason for most deaths, the study states. States should improve access to free ambulances, it says.</p><p style="text-align: justify">In a country like India where midwives still cover 50 per cent of the deliveries, home delivery gets no support from the government, says Das. In the 1920s, developing countries such as Denmark and the Netherlands supported home deliveries and had lower MMR than developing countries like the US and New Zealand which believed only in institutional deliveries, he says. Sri Lanka managed to reduce its MMR to 60 in 2008 by widely using midwives for home deliveries and strengthening the health system. Centre for Global Development, a US-based research organisation, states that 97 per cent of the births in Sri Lanka are attended by skilled midwives. It also provides free medical services to all.</p><p style="text-align: justify">"India cannot provide medical service to all in public institutions. In such a scenario, how justified is it to promote only institutional deliveries?" wonders Mehrotra. She suggests integrating midwives, accredited social health activists (ASHAs) and auxiliary nurse midwives (ANMs) for delivery cases. ASHAs can counsel pregnant women; midwives, with their knowledge of the female body, can identify critical cases and perform normal deliveries; and ANMs can coordinate with health centres for institutional deliveries.</p><p style="text-align: justify">To improve the situation, the government should shift the debate from home delivery versus institutional delivery to safe delivery versus unsafe, says Rehman.</p><p style="text-align: justify"><strong>EXPERTS’ RECOMMENDATIONS</strong></p><p style="text-align: justify">Improve infrastructure at each operation theatre—availability of oxygen, provision for spinal anaesthesia, inverter and generator</p><p style="text-align: justify">Ultrasonography at each community health centre</p><p style="text-align: justify">Clear-cut norms for referring patients from one hospital to another, audit this on a regular basis</p><p style="text-align: justify">Maternal health services as per the local requirement that also protect women’s dignity</p><p style="text-align: justify">Compulsory provisioning of high-nutrition food to expecting mothers</p><p style="text-align: justify">Transparent and centralised medicine supply and procurement system</p><p style="text-align: justify">Wireless system in areas that do not have mobile connectivity</p><p style="text-align: justify">Legalise unbanked direct blood transfusion; ready list of donors to ensure blood availability in emergency situations</p><p style="text-align: justify">Source: List of demands by experts at a national convention on second generation plan on maternal health </p><p style="text-align: justify"> </p><p style="text-align: justify"><em>With inputs from Alok Gupta</em> </p>
</div>
</td>
</tr>
</table>
</div>
</div>
</div>
<div class="clear"></div>
<br><a href="http://www.downtoearth.org.in/content/delivering-safety" class="re" target="_blank">Down to Earth, 30 April, 2014, http://www.downtoearth.org.in/content/delivering-safety</a><div class="clear"></div>
<div style="padding-top: 18px;">
<p class="post-tag">Tagged with:
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=maternal mortality ratio"
title="maternal mortality ratio">
maternal mortality ratio </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=maternal deaths"
title="maternal deaths">
maternal deaths </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Health"
title="Health">
Health </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=maternal mortality"
title="maternal mortality">
maternal mortality </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Maternal Health"
title="Maternal Health">
Maternal Health </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=hospitals"
title="hospitals">
hospitals </a>
</p>
</div>
<div class="clear"></div>
<br><br>
<div class="widget-top">
<h4>Related Articles</h4>
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<ul id="recentcomments">
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/fifth-report-from-gambia-implicates-indian-drug-maker-for-contaminated-syrups-banjot-kaur.html"
title="Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur">
Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-may-have-seen-steepest-dip-in-multidimensional-poverty-among-110-nations-as-per-undp-data-nikhil-rampal.html"
title="India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal">
India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/health-among-top-three-priorities-for-indian-voters-after-jobs-and-education-survey-shows-oliver-heath-jyoti-mishra-louise-tillin-sandhya-venkateswaran.html"
title="Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran">
Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-s-stretched-health-care-system-fails-millions-in-rural-areas-battling-sickle-cell-disease-abc.html"
title="India's stretched health care system fails millions in rural areas battling sickle cell disease - ABC">
India's stretched health care system fails millions in rural areas battling sickle cell disease - ABC </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/prevalence-of-zero-food-among-infants-and-young-children-in-india-patterns-of-change-across-the-states-and-union-territories-of-india-1993-2021-the-lancet.html"
title="Prevalence of Zero-Food among infants and young children in India - The Lancet ">
Prevalence of Zero-Food among infants and young children in India - The Lancet </a>
</li>
</ul>
</div>
<div class="comment-respond" id="respond">
<a name="commentbox"> </a>
<h3 class="comment-reply-title" id="reply-title">Write Comments</h3>
<form method="post" accept-charset="utf-8" role="form" action="/latest-news-updates/delivering-safety-kundan-pandey-24858.html"><div style="display:none;"><input type="hidden" name="_method" value="POST"/></div> <form class="comment-form" id="commentform" method="post" action="#commentbox" onSubmit="return validate()"
name="cmtform">
<input type="hidden" name="cmttype" value="articlecmt"/>
<input type="hidden" name="article_id" value="24677"/>
<p class="comment-notes">Your email address will not be published. Required fields are marked <span
class="required">*</span></p>
<p class="comment-form-author">
<label for="commenterName">Name</label>
<span class="required">*</span>
<input type="text" aria-required="true" size="30"
value=""
name="commenterName" id="commenterName" required="true">
</p>
<p class="comment-form-email">
<label for="commenterEmail">Email</label> <span class="required">*</span>
<input aria-required="true" size="30" name="commenterEmail" id="commenterEmail" type="email"
value=""
required="true">
</p>
<p class="comment-form-contact">
<label for="commenterPh">Contact No.</label>
<input type="text" size="30"
value=""
name="commenterPh" id="commenterPh">
</p>
<p class="comment-form-comment">
<label for="comment">Comment</label>
<textarea aria-required="true" required="true" rows="8" cols="45" name="comment"
id="comment"></textarea>
</p>
<p class="comment-form-comment">
<label for="comment">Type the characters you see in the image below <span class="required">*</span><br><img
class="captchaImg"
src="https://im4change.in/securimage_show_art.php?tk=1760450620" alt="captcha"/>
</label>
</p>
<input type="text" name="vrcode" required="true"/>
<p class="form-submit" style="width: 200px;">
<input type="submit" value="Post Comment" id="submit" name="submit">
</p></form>
</div>
<style>
.ui-widget-content {
height: auto !important;
}
</style>
<div id="share-modal"></div>
<style>
.middleContent a{
background-color: rgba(108,172,228,.2);
}
.middleContent a:hover{
background-color: #418fde;
border-color: #418fde;
color: #000;
}
</style>
<script>
function shareArticle(article_id) {
var options = {
modal: true,
height: 'auto',
width: 600 + 'px'
};
$('#share-modal').html("");
$('#share-modal').load('https://im4change.in/share_article?article_id=' + article_id).dialog(options).dialog('open');
}
function postShare() {
var param = 'article_id=' + $("#article_id").val();
param = param + '&y_name=' + $("#y_name").val();
param = param + '&y_email=' + $("#y_email").val();
param = param + '&f_name=' + $("#f_name").val();
param = param + '&f_email=' + $("#f_email").val();
param = param + '&y_msg=' + $("#y_msg").val();
$.ajax({
type: "POST",
url: 'https://im4change.in/post_share_article',
data: param,
success: function (response) {
$('#share-modal').html("Thank You, Your message posted to ");
}
});
return false;
}
</script> </div>
</div>
<!-- Right Side Section Start -->
<!-- MAP Section START -->
<aside class="sidebar indexMarg">
<div class="ad-cell">
<a href="https://im4change.in/statemap.php" title="">
<img src="https://im4change.in/images/map_new_version.png?1582080666" alt="India State Map" class="indiamap" width="232" height="252"/> </a>
<div class="rightmapbox">
<div id="sideOne" class="docltitle"><a href="https://im4change.in/state-report/india/36" target="_blank">DOCUMENTS/
REPORTS</a></div>
<div id="sideTwo" class="statetitle"><a href="https://im4change.in/states.php"target="_blank">STATE DATA/
HDRs.</a></div>
</div>
<div class="widget widgePadTop"></div>
</div>
</aside>
<!-- MAP Section END -->
<aside class="sidebar sidePadbottom">
<div class="rightsmlbox1" >
<a href="https://im4change.in/knowledge_gateway" target="_blank" style="color: #035588;
font-size: 17px;">
KNOWLEDGE GATEWAY
</a>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/newsletter" target="_blank">
NEWSLETTER
</a>
</p>
</div>
</div>
<div class="rightsmlbox1" style="height: 325px;">
<div>
<p class="rightsmlbox1_title">
Interview with Prof. Ravi Srivastava
</p>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/video/interview-with-prof-ravi-srivastava-on-current-economic-crisis">
<img width="250" height="200" src="/images/interview_video_home.jpg" alt="Interview with Prof. Ravi Srivastava"/>
</a>
<!--
<iframe width="250" height="200" src="https://www.youtube.com/embed/MmaTlntk-wc" frameborder="0" allow="accelerometer; autoplay; encrypted-media; gyroscope; picture-in-picture" allowfullscreen=""></iframe>-->
</p>
<a href="https://im4change.in/videogallery" class="more-link CatArchalAnch1" target="_blank">
More videos
</a>
</div>
</div>
<div class="rightsmlbox1">
<div>
<!--div id="sstory" class="rightboxicons"></div--->
<p class="rightsmlbox1_title"><a href="https://im4change.in/list-success-stories" target="_blank">Success Stories</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/interviews" target="_blank">Interviews</a>
</p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a href="https://www.commoncause.in/page.php?id=10" >Donate</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/marquee"
class="isf_link more-link" title="India Focus?" style="border: 4px solid #fdd922;width: 90%;background-color: #fdd922;text-align: center;color: #000000;font-size:18px" target="_blank">India Focus</a></p> </div>
</div>
<div class="rightsmlbox1" style="height: 104px !important;">
<a href="https://im4change.in/quarterly_reports.php" target="_blank">
Quarterly Reports on Effect of Economic Slowdown on Employment in India (2008 - 2015)
</a>
</div>
<!-- <div class="rightsmlbox1">
<a href="https://play.google.com/store/apps/details?id=com.im4.im4change" target="_blank">
</a></div> -->
<!-- <section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">Most Visited</h2>
</section> -->
<!-- accordion Starts here -->
<!-- <div id="accordion" class="accordMarg">
</div> -->
<!-- accordion ends here -->
<!-- Widget Tag Cloud Starts here -->
<div id="tag_cloud-2" class="widget widget_tag_cloud">
<section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">MOST VISITED TAGS</h2>
</section>
<div class="widget-top wiPdTp">
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<div class="tagcloud">
<a href="https://im4change.in/search?qryStr=Agriculture"
target="_blank" class="tag-link-4 font4">Agriculture</a>
<a href="https://im4change.in/search?qryStr=Food Security"
target="_blank" class="tag-link-4 font4">Food Security</a>
<a href="https://im4change.in/search?qryStr=Law and Justice"
target="_blank" class="tag-link-4 font4">Law and Justice</a>
<a href="https://im4change.in/search?qryStr=Health"
target="_blank" class="tag-link-4 font4">Health</a>
<a href="https://im4change.in/search?qryStr=Right to Food"
target="_blank" class="tag-link-4 font4">Right to Food</a>
<a href="https://im4change.in/search?qryStr=Corruption"
target="_blank" class="tag-link-4 font4">Corruption</a>
<a href="https://im4change.in/search?qryStr=farming"
target="_blank" class="tag-link-4 font4">farming</a>
<a href="https://im4change.in/search?qryStr=Environment"
target="_blank" class="tag-link-4 font4">Environment</a>
<a href="https://im4change.in/search?qryStr=Right to Information"
target="_blank" class="tag-link-4 font4">Right to Information</a>
<a href="https://im4change.in/search?qryStr=NREGS"
target="_blank" class="tag-link-4 font4">NREGS</a>
<a href="https://im4change.in/search?qryStr=Human Rights"
target="_blank" class="tag-link-4 font4">Human Rights</a>
<a href="https://im4change.in/search?qryStr=Governance"
target="_blank" class="tag-link-4 font4">Governance</a>
<a href="https://im4change.in/search?qryStr=PDS"
target="_blank" class="tag-link-4 font4">PDS</a>
<a href="https://im4change.in/search?qryStr=COVID-19"
target="_blank" class="tag-link-4 font4">COVID-19</a>
<a href="https://im4change.in/search?qryStr=Land Acquisition"
target="_blank" class="tag-link-4 font4">Land Acquisition</a>
<a href="https://im4change.in/search?qryStr=mgnrega"
target="_blank" class="tag-link-4 font4">mgnrega</a>
<a href="https://im4change.in/search?qryStr=Farmers"
target="_blank" class="tag-link-4 font4">Farmers</a>
<a href="https://im4change.in/search?qryStr=transparency"
target="_blank" class="tag-link-4 font4">transparency</a>
<a href="https://im4change.in/search?qryStr=Gender"
target="_blank" class="tag-link-4 font4">Gender</a>
<a href="https://im4change.in/search?qryStr=Poverty"
target="_blank" class="tag-link-4 font4">Poverty</a>
<a href="https://im4change.in/search?qryStr=Farm Laws" target="_blank" class="tag-link-4 font4">Farm Laws
</a>
<a href="https://im4change.in/search?qryStr=Citizenship Amendment Act" target="_blank" class="tag-link-4 font4">Citizenship Amendment Act
</a>
<a href="https://im4change.in/search?qryStr=CAA NPR NRIC" target="_blank" class="tag-link-4 font4">CAA NPR NRIC
</a>
<a href="https://im4change.in/search?qryStr=Job Losses" target="_blank" class="tag-link-4 font4">Job Losses
</a>
<a href="https://im4change.in/search?qryStr=Migrant Workers" target="_blank" class="tag-link-4 font4">Migrant Workers
</a>
<a href="https://im4change.in/search?qryStr=Unemployment" target="_blank" class="tag-link-4 font4">Unemployment
</a>
<a href="https://im4change.in/search?qryStr=PMGKAY" target="_blank" class="tag-link-4 font4">PMGKAY
</a>
<a href="https://im4change.in/search?qryStr=PM-KISAN" target="_blank" class="tag-link-4 font4">PM-KISAN
</a>
<a href="https://im4change.in/search?qryStr=PM-CARES" target="_blank" class="tag-link-4 font4">PM-CARES
</a>
<a href="https://im4change.in/search?qryStr=LFPR" target="_blank" class="tag-link-4 font4">LFPR
</a>
</div>
</div>
</div>
<!-- Widget Tag Cloud Ends here -->
</aside>
<!-- Right Side Section End -->
</div>
<section class="cat-box cats-review-box footerSec">
<h2 class="cat-box-title vSec CatArcha">Video
Archives</h2>
<h2 class="cat-box-title CatArchaTitle">Archives</h2>
<div class="cat-box-content">
<div class="reviews-cat">
<div class="CatArchaDiv1">
<div class="CatArchaDiv2">
<ul>
<li>
<a href="https://im4change.in/news-alerts-57/moving-upstream-luni-fellowship.html" target="_blank">
Moving Upstream: Luni – Fellowship </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/135-million-indians-exited-multidimensional-poverty-as-per-government-figures-is-that-the-same-as-poverty-reduction.html" target="_blank">
135 Million Indians Exited “Multidimensional" Poverty as per Government... </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/explainer-why-are-tomato-prices-on-fire.html" target="_blank">
Explainer: Why are Tomato Prices on Fire? </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/nsso-survey-only-39-1-of-all-households-have-drinking-water-within-dwelling-46-7-of-rural-households-use-firewood-for-cooking.html" target="_blank">
NSSO Survey: Only 39.1% of all Households have Drinking... </a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/news-alerts-57"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/I51LYnP8BOk/1.jpg"
alt=" Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Short-Video-on-im4change-Hindi-website-Inclusive-Media-for-Change" target="_blank">
Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/kNqha-SwfIY/1.jpg"
alt=" "Session 1: Scope of IDEA and AgriStack" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-1- Scope-of-IDEA-and-AgriStack-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 1: Scope of IDEA and AgriStack" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/6kIVjlgZItk/1.jpg"
alt=" "Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-2-Farmer-Centric-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/2BeHTu0y7xc/1.jpg"
alt=" "Session 3: Future of Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-3-Future-of-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 3: Future of Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="divWidth">
<ul class="divWidthMarg">
<li>
<a href="https://im4change.in/video/Public-Spending-on-Agriculture-in-India-Source-Foundation-for-Agrarian-Studies"
title="Public Spending on Agriculture in India (Source: Foundation for Agrarian Studies)" target="_blank">
Public Spending on Agriculture in India (Source: Foundation for...</a>
</li>
<li>
<a href="https://im4change.in/video/Agrarian-Change-Seminar-Protests-against-the-New-Farm-Laws-in-India-by-Prof-Vikas-Rawal-JNU-Source-Journal-Of-Agrarian-Change"
title="Agrarian Change Seminar: 'Protests against the New Farm Laws in India' by Prof. Vikas Rawal, JNU (Source: Journal Of Agrarian Change) " target="_blank">
Agrarian Change Seminar: 'Protests against the New Farm Laws...</a>
</li>
<li>
<a href="https://im4change.in/video/Webinar-Ramrao-The-Story-of-India-Farm-Crisis-Source-Azim-Premji-University"
title="Webinar: Ramrao - The Story of India's Farm Crisis (Source: Azim Premji University)" target="_blank">
Webinar: Ramrao - The Story of India's Farm Crisis...</a>
</li>
<li>
<a href="https://im4change.in/video/water-and-agricultural-transformation-in-India"
title="Water and Agricultural Transformation in India: A Symbiotic Relationship (Source: IGIDR)" target="_blank">
Water and Agricultural Transformation in India: A Symbiotic Relationship...</a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/videogallery"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
</div>
</div>
</div>
</section> </div>
<div class="clear"></div>
<!-- Footer option Starts here -->
<div class="footer-bottom fade-in animated4">
<div class="container">
<div class="social-icons icon_flat">
<p class="SocialMargTop"> Website Developed by <a target="_blank" title="Web Development"
class="wot right"
href="http://www.ravinderkhurana.com/" rel="nofollow">
RAVINDErkHURANA.com</a></p>
</div>
<div class="alignleft">
<a
target="_blank" href="https://im4change.in/objectives-8.html"
class="link"
title="Objectives">Objectives</a> | <a
target="_blank" href="https://im4change.in/about-us-9.html"
class="link" title="About Us">About Us</a> | <a
target="_blank" href="https://im4change.in/media-workshops.php"
class="ucwords">Workshops</a> | <a
target="_blank" href="https://im4change.in/disclaimer/disclaimer-149.html"
title="Disclaimer">Disclaimer</a> </div>
</div>
</div>
<!-- Footer option ends here -->
</div>
<div id="connect">
<a target="_blank"
href="http://www.facebook.com/sharer.php?u=https://im4change.in/latest-news-updates/delivering-safety-kundan-pandey-24858.html"
title="Share on Facebook">
<img src="https://im4change.in/images/Facebook.png?1582080640" alt="share on Facebook" class="ImgBorder"/>
</a><br/>
<a target="_blank"
href="http://twitter.com/share?text=Im4change&url=https://im4change.in/latest-news-updates/delivering-safety-kundan-pandey-24858.html"
title="Share on Twitter">
<img src="https://im4change.in/images/twitter.png?1582080632" alt="Twitter" class="ImgBorder"/> </a>
<br/>
<a href="/feeds" title="RSS Feed" target="_blank">
<img src="https://im4change.in/images/rss.png?1582080632" alt="RSS" class="ImgBorder"/>
</a>
<br/>
<a class="feedback-link" id="feedbackFormLink" href="#">
<img src="https://im4change.in/images/feedback.png?1582080630" alt="Feedback" class="ImgBorder"/>
</a> <br/>
<a href="javascript:function iprl5(){var d=document,z=d.createElement('scr'+'ipt'),b=d.body,l=d.location;try{if(!b)throw(0);d.title='(Saving...) '+d.title;z.setAttribute('src',l.protocol+'//www.instapaper.com/j/WKrH3R7ORD5p?u='+encodeURIComponent(l.href)+'&t='+(new Date().getTime()));b.appendChild(z);}catch(e){alert('Please wait until the page has loaded.');}}iprl5();void(0)"
class="bookmarklet" onclick="return explain_bookmarklet();">
<img src="https://im4change.in/images/read-it-later.png?1582080632" alt="Read Later" class="ImgBorder"/> </a>
</div>
<!-- Feedback form Starts here -->
<div id="feedbackForm" class="overlay_form" class="ImgBorder">
<h2>Contact Form</h2>
<div id="contactform1">
<div id="formleft">
<form id="submitform" action="/contactus.php" method="post">
<input type="hidden" name="submitform" value="submitform"/>
<input type="hidden" name="salt_key" value="a0e0f2c6a0644a70e57ad2c96829709a"/>
<input type="hidden" name="ref" value="feedback"/>
<fieldset>
<label>Name :</label>
<input type="text" name="name" class="tbox" required/>
</fieldset>
<fieldset>
<label>Email :</label>
<input type="text" name="email" class="tbox" required/>
</fieldset>
<fieldset>
<label>Message :</label>
<textarea rows="5" cols="20" name="message" required></textarea>
</fieldset>
<fieldset>
Please enter security code
<div class="clear"></div>
<input type="text" name="vrcode" class="tbox"/>
</fieldset>
<fieldset>
<input type="submit" class="button" value="Submit"/>
<a href="#" id="closefeedbakcformLink">Close</a>
</fieldset>
</form>
</div>
<div class="clearfix"></div>
</div>
</div>
<div id="donate_popup" class="modal" style="max-width: 800px;">
<table width="100%" border="1">
<tr>
<td colspan="2" align="center">
<b>Support im4change</b>
</td>
</tr>
<tr>
<td width="25%" valign="middle">
<img src="https://im4change.in/images/logo2.jpg?1582080632" alt="" width="100%"/> </td>
<td style="padding-left:10px;padding-top:10px;">
<form action="https://im4change.in/donate" method="get">
<table width="100%" cellpadding="2" cellspacing="2">
<tr>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
10
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
100
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
1000
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
50
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
500
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
<input type="text" name="price" placeholder="?" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td colspan="3" align="right">
<input type="button" name="Pay" value="Pay"
style="width: 200px;background-color: rgb(205, 35, 36);color: #ffffff;"/>
</td>
</tr>
</table>
</form>
</td>
</tr>
</table>
</div><script type='text/javascript'>
/* <![CDATA[ */
var tievar = {'go_to': 'Go to...'};
/* ]]> */
</script>
<script src="/js/tie-scripts.js?1575549704"></script><script src="/js/bootstrap.js?1575549704"></script><script src="/js/jquery.modal.min.js?1578284310"></script><script>
$(document).ready(function() {
// tell the autocomplete function to get its data from our php script
$('#s').autocomplete({
source: "/autocomplete"
});
});
</script>
<script src="/vj-main-sw-register.js" async></script>
<script>function init(){var imgDefer=document.getElementsByTagName('img');for(var i=0;i<imgDefer.length;i++){if(imgDefer[i].getAttribute('data-src')){imgDefer[i].setAttribute('src',imgDefer[i].getAttribute('data-src'))}}}
window.onload=init;</script>
</body>
</html>'
}
$maxBufferLength = (int) 8192
$file = '/home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php'
$line = (int) 853
$message = 'Unable to emit headers. Headers sent in file=/home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php line=853'
Cake\Http\ResponseEmitter::emit() - CORE/src/Http/ResponseEmitter.php, line 48
Cake\Http\Server::emit() - CORE/src/Http/Server.php, line 141
[main] - ROOT/webroot/index.php, line 39
Warning (2): Cannot modify header information - headers already sent by (output started at /home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php:853) [CORE/src/Http/ResponseEmitter.php, line 148]
$response = object(Cake\Http\Response) {
'status' => (int) 200,
'contentType' => 'text/html',
'headers' => [
'Content-Type' => [
[maximum depth reached]
]
],
'file' => null,
'fileRange' => [],
'cookies' => object(Cake\Http\Cookie\CookieCollection) {},
'cacheDirectives' => [],
'body' => '<!DOCTYPE html>
<!--[if lt IE 7 ]>
<html class="ie ie6" lang='en'> <![endif]-->
<!--[if IE 7 ]>
<html class="ie ie7" lang='en'> <![endif]-->
<!--[if IE 8 ]>
<html class="ie ie8" lang='en'> <![endif]-->
<!--[if (gte IE 9)|!(IE)]><!-->
<html lang='en'>
<!--<![endif]-->
<head><meta http-equiv="Content-Type" content="text/html; charset=utf-8">
<title>
LATEST NEWS UPDATES | Delivering safety -Kundan Pandey </title>
<meta name="description" content="
-Down to Earth
All safe motherhood programmes of the government are focused on institutional deliveries, but health centres are in disarray. Experts suggest ways to reduce deaths during delivery
Lal Mohan, a daily wage labourer, has no clue what took his wife's..."/>
<meta name="keywords" content="maternal mortality ratio,maternal deaths,Health,maternal mortality,Maternal Health,hospitals"/>
<meta name="news_keywords" content="maternal mortality ratio,maternal deaths,Health,maternal mortality,Maternal Health,hospitals">
<link rel="alternate" type="application/rss+xml" title="ROR" href="/ror.xml"/>
<link rel="alternate" type="application/rss+xml" title="RSS 2.0" href="/feeds/"/>
<link rel="stylesheet" href="/css/bootstrap.min.css?1697864993"/> <link rel="stylesheet" href="/css/style.css?v=1.1.2"/> <link rel="stylesheet" href="/css/style-inner.css?1577045210"/> <link rel="stylesheet" id="Oswald-css"
href="https://fonts.googleapis.com/css?family=Oswald%3Aregular%2C700&ver=3.8.1" type="text/css"
media="all">
<link rel="stylesheet" href="/css/jquery.modal.min.css?1578285302"/> <script src="/js/jquery-1.10.2.js?1575549704"></script> <script src="/js/jquery-migrate.min.js?1575549704"></script> <link rel="shortcut icon" href="/favicon.ico" title="Favicon">
<link rel="stylesheet" href="/css/jquery-ui.css?1580720609"/> <script src="/js/jquery-ui.js?1575549704"></script> <link rel="preload" as="style" href="https://www.im4change.org/css/custom.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery.modal.min.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery-ui.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/li-scroller.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<!-- <link rel="preload" as="style" href="https://www.im4change.org/css/style.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous"> -->
<link rel="preload" as="style" href="https://www.im4change.org/css/style-inner.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel='dns-prefetch' href="//im4change.org/css/custom.css" crossorigin >
<link rel="preload" as="script" href="https://www.im4change.org/js/bootstrap.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.li-scroller.1.0.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.modal.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.ui.totop.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-1.10.2.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-migrate.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-ui.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/setting.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/tie-scripts.js">
<!--[if IE]>
<script type="text/javascript">jQuery(document).ready(function () {
jQuery(".menu-item").has("ul").children("a").attr("aria-haspopup", "true");
});</script>
<![endif]-->
<!--[if lt IE 9]>
<script src="/js/html5.js"></script>
<script src="/js/selectivizr-min.js"></script>
<![endif]-->
<!--[if IE 8]>
<link rel="stylesheet" type="text/css" media="all" href="/css/ie8.css"/>
<![endif]-->
<meta property="og:title" content="LATEST NEWS UPDATES | Delivering safety -Kundan Pandey" />
<meta property="og:url" content="https://im4change.in/latest-news-updates/delivering-safety-kundan-pandey-24858.html" />
<meta property="og:type" content="article" />
<meta property="og:description" content="
-Down to Earth
All safe motherhood programmes of the government are focused on institutional deliveries, but health centres are in disarray. Experts suggest ways to reduce deaths during delivery
Lal Mohan, a daily wage labourer, has no clue what took his wife's..." />
<meta property="og:image" content="" />
<meta property="fb:app_id" content="0" />
<meta name="viewport" content="width=device-width, initial-scale=1, maximum-scale=1, user-scalable=no">
<link rel="apple-touch-icon-precomposed" sizes="144x144" href="https://im4change.in/images/apple1.png">
<link rel="apple-touch-icon-precomposed" sizes="120x120" href="https://im4change.in/images/apple2.png">
<link rel="apple-touch-icon-precomposed" sizes="72x72" href="https://im4change.in/images/apple3.png">
<link rel="apple-touch-icon-precomposed" href="https://im4change.in/images/apple4.png">
<style>
.gsc-results-wrapper-overlay{
top: 38% !important;
height: 50% !important;
}
.gsc-search-button-v2{
border-color: #035588 !important;
background-color: #035588 !important;
}
.gsib_a{
height: 30px !important;
padding: 2px 8px 1px 6px !important;
}
.gsc-search-button-v2{
height: 41px !important;
}
input.gsc-input{
background: none !important;
}
@media only screen and (max-width: 600px) {
.gsc-results-wrapper-overlay{
top: 11% !important;
width: 87% !important;
left: 9% !important;
height: 43% !important;
}
.gsc-search-button-v2{
padding: 10px 10px !important;
}
.gsc-input-box{
height: 28px !important;
}
/* .gsib_a {
padding: 0px 9px 4px 9px !important;
}*/
}
@media only screen and (min-width: 1200px) and (max-width: 1920px) {
table.gsc-search-box{
width: 15% !important;
float: right !important;
margin-top: -118px !important;
}
.gsc-search-button-v2 {
padding: 6px !important;
}
}
</style>
<script>
$(function () {
$("#accordion").accordion({
event: "click hoverintent"
});
});
/*
* hoverIntent | Copyright 2011 Brian Cherne
* http://cherne.net/brian/resources/jquery.hoverIntent.html
* modified by the jQuery UI team
*/
$.event.special.hoverintent = {
setup: function () {
$(this).bind("mouseover", jQuery.event.special.hoverintent.handler);
},
teardown: function () {
$(this).unbind("mouseover", jQuery.event.special.hoverintent.handler);
},
handler: function (event) {
var currentX, currentY, timeout,
args = arguments,
target = $(event.target),
previousX = event.pageX,
previousY = event.pageY;
function track(event) {
currentX = event.pageX;
currentY = event.pageY;
}
;
function clear() {
target
.unbind("mousemove", track)
.unbind("mouseout", clear);
clearTimeout(timeout);
}
function handler() {
var prop,
orig = event;
if ((Math.abs(previousX - currentX) +
Math.abs(previousY - currentY)) < 7) {
clear();
event = $.Event("hoverintent");
for (prop in orig) {
if (!(prop in event)) {
event[prop] = orig[prop];
}
}
// Prevent accessing the original event since the new event
// is fired asynchronously and the old event is no longer
// usable (#6028)
delete event.originalEvent;
target.trigger(event);
} else {
previousX = currentX;
previousY = currentY;
timeout = setTimeout(handler, 100);
}
}
timeout = setTimeout(handler, 100);
target.bind({
mousemove: track,
mouseout: clear
});
}
};
</script>
<script type="text/javascript">
var _gaq = _gaq || [];
_gaq.push(['_setAccount', 'UA-472075-3']);
_gaq.push(['_trackPageview']);
(function () {
var ga = document.createElement('script');
ga.type = 'text/javascript';
ga.async = true;
ga.src = ('https:' == document.location.protocol ? 'https://ssl' : 'http://www') + '.google-analytics.com/ga.js';
var s = document.getElementsByTagName('script')[0];
s.parentNode.insertBefore(ga, s);
})();
</script>
<link rel="stylesheet" href="/css/custom.css?v=1.16"/> <script src="/js/jquery.ui.totop.js?1575549704"></script> <script src="/js/setting.js?1575549704"></script> <link rel="manifest" href="/manifest.json">
<meta name="theme-color" content="#616163" />
<meta name="apple-mobile-web-app-capable" content="yes">
<meta name="apple-mobile-web-app-status-bar-style" content="black">
<meta name="apple-mobile-web-app-title" content="im4change">
<link rel="apple-touch-icon" href="/icons/logo-192x192.png">
</head>
<body id="top" class="home inner blog">
<div class="background-cover"></div>
<div class="wrapper animated">
<header id="theme-header" class="header_inner" style="position: relative;">
<div class="logo inner_logo" style="left:20px !important">
<a title="Home" href="https://im4change.in/">
<img src="https://im4change.in/images/logo2.jpg?1582080632" class="logo_image" alt="im4change"/> </a>
</div>
<div class="langhindi" style="color: #000;display:none;"
href="https://im4change.in/">
<a class="more-link" href="https://im4change.in/">Home</a>
<a href="https://im4change.in/hindi/" class="langbutton ">हिन्दी</a>
</div>
<nav class="fade-in animated2" id="main-nav">
<div class="container">
<div class="main-menu">
<ul class="menu" id="menu-main">
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
style="left: -40px;"><a
target="_blank" href="https://im4change.in/">Home</a>
</li>
<li class="menu-item mega-menu menu-item-type-taxonomy mega-menu menu-item-object-category mega-menu menu-item-has-children parent-list"
style=" margin-left: -40px;"><a href="#">KNOWLEDGE GATEWAY <span class="sub-indicator"></span>
</a>
<div class="mega-menu-block background_menu" style="padding-top:25px;">
<div class="container">
<div class="mega-menu-content">
<div class="mega-menu-item">
<h3><b>Farm Crisis</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/farmers039-suicides-14.html"
class="left postionrel">Farm Suicides </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/unemployment-30.html"
class="left postionrel">Unemployment </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/rural-distress-70.html"
class="left postionrel">Rural distress </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/migration-34.html"
class="left postionrel">Migration </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/key-facts-72.html"
class="left postionrel">Key Facts </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/debt-trap-15.html"
class="left postionrel">Debt Trap </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Empowerment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/union-budget-73.html"
class="left postionrel">Union Budget And Other Economic Policies </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/forest-and-tribal-rights-61.html"
class="left postionrel">Forest and Tribal Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-education-60.html"
class="left postionrel">Right to Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-food-59.html"
class="left postionrel">Right to Food </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/displacement-3279.html"
class="left postionrel">Displacement </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-work-mg-nrega-39.html"
class="left postionrel">Right to Work (MG-NREGA) </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/gender-3280.html"
class="left postionrel">GENDER </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-information-58.html"
class="left postionrel">Right to Information </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/social-audit-48.html"
class="left postionrel">Social Audit </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Hunger / HDI</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/poverty-and-inequality-20499.html"
class="left postionrel">Poverty and inequality </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/malnutrition-41.html"
class="left postionrel">Malnutrition </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/public-health-51.html"
class="left postionrel">Public Health </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/education-50.html"
class="left postionrel">Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hunger-overview-40.html"
class="left postionrel">Hunger Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hdi-overview-45.html"
class="left postionrel">HDI Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/pds-ration-food-security-42.html"
class="left postionrel">PDS/ Ration/ Food Security </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/sdgs-113.html"
class="left postionrel">SDGs </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/mid-day-meal-scheme-mdms-53.html"
class="left postionrel">Mid Day Meal Scheme (MDMS) </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Environment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/time-bomb-ticking-52.html"
class="left postionrel">Time Bomb Ticking </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/water-and-sanitation-55.html"
class="left postionrel">Water and Sanitation </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/impact-on-agriculture-54.html"
class="left postionrel">Impact on Agriculture </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Law & Justice</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/social-justice-20500.html"
class="left postionrel">Social Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/access-to-justice-47.html"
class="left postionrel">Access to Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/human-rights-56.html"
class="left postionrel">Human Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/corruption-35.html"
class="left postionrel">Corruption </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/general-insecurity-46.html"
class="left postionrel">General Insecurity </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/disaster-relief-49.html"
class="left postionrel">Disaster & Relief </a>
</p>
</div>
</div>
</div>
</div>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page "><a target="_blank" href="https://im4change.in/nceus_reports.php">NCEUS reports</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children parent-list ">
<a target="_blank" href="https://im4change.in/about-us-9.html">About Us <span
class="sub-indicator"></span></a>
<ul class="sub-menu aboutmenu">
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/objectives-8.html">Objectives</a>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/contactus.php">Contact
Us</a></li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/about-us-9.html">About
Us</a></li>
</ul>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children ">
<a target="_blank" href="https://im4change.in/fellowships.php" title="Fellowships">Fellowships</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/media-workshops.php">Workshops</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/research.php">Research</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/links-64">Partners</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
id="menu-item-539"><a target="_blank" href="https://im4change.in/hindi/"
class="langbutton langlinkfont17">हिन्दी</a></li>
</ul>
</div> </div>
<!-- <div style="float: right;">
<script async src="https://cse.google.com/cse.js?cx=18b4f2e0f11bed3dd"></script>
<div class="gcse-search"></div>
</div> -->
<div class="search-block" style=" margin-left: 8px; margin-right: 7px;">
<form method="get" id="searchform" name="searchform"
action="https://im4change.in/search"
onsubmit="return searchvalidate();">
<button class="search-button" type="submit" value="Search"></button>
<input type="text" id="s" name="qryStr" value=""
onfocus="if (this.value == 'Search...') {this.value = '';}"
onblur="if (this.value == '') {this.value = 'Search...';}">
</form>
</div>
</nav>
</header>
<div class="container">
<div id="main-content" class=" main1 container fade-in animated3 sidebar-narrow-left">
<div class="content-wrap">
<div class="content" style="width: 900px;min-height: 500px;">
<section class="cat-box recent-box innerCatRecent">
<h1 class="cat-box-title">Delivering safety -Kundan Pandey</h1>
<a href="JavaScript:void(0);" onclick="return shareArticle(24677);">
<img src="https://im4change.in/images/email.png?1582080630" border="0" width="24" align="right" alt="Share this article"/> </a>
<a href="https://im4change.in/latest-news-updates/delivering-safety-kundan-pandey-24858/print"
rel="nofollow">
<img src="https://im4change.in/images/icon-print.png?1582080630" border="0" width="24" align="right" alt="Share this article"/>
</a>
</section>
<section class="recent-box innerCatRecent">
<small class="pb-1"><span class="dateIcn">
<img src="https://im4change.in/images/published.svg?1582080666" alt="published"/>
Published on</span><span class="text-date"> Apr 28, 2014</span>
<span
class="dateIcn">
<img src="https://im4change.in/images/modified.svg?1582080666" alt="modified"/> Modified on </span><span class="text-date"> Apr 28, 2014</span>
</small>
</section>
<div class="clear"></div>
<div style="padding-top: 10px;">
<div class="innerLineHeight">
<div class="middleContent innerInput latest-news-updates">
<table>
<tr>
<td>
<div>
<div style="text-align: justify">-Down to Earth</div><div style="text-align: justify"> </div><p style="text-align: justify"><em>All safe motherhood programmes of the government are focused on institutional deliveries, but health centres are in disarray. Experts suggest ways to reduce deaths during delivery</em></p><p style="text-align: justify">Lal Mohan, a daily wage labourer, has no clue what took his wife's life. Sarita Devi, 25, was expecting her third child, and was on way to a good hospital at Bhagalpur district in Bihar. "She was normal all through the nine months of pregnancy," he says. "When labour pains began, we took her to a community health centre (CHC), 15 km from our house in Godda district in Jharkhand. At around 11 pm, doctors advised us to take her to Sadar Hospital, 20 km from the CHC. Here again, doctors referred her to Jawaharlal Nehru Medical College and Hospital in Bhagalpur, another 70 km away." She passed away on the way to hospital.</p><p style="text-align: justify">Sarita's death is not a one-off case. In a year, hundreds of women die during or after pregnancy in the Santhal Pargana region, where Sarita lived. Child marriage is rampant in the region and girls usually become pregnant at the age of 16, says Soumik Bannerjee, health activist in Godda. Their undernourished bodies are ill-prepared for travelling to faraway places during labour pains, that too under no medical supervision or advise. Small wonder, Santhal Pargana has a high maternal mortality ratio (MMR), of more than 300 deaths per 100,000 live births, he says.</p><p style="text-align: justify">This is the result of the government's focus on only institutional deliveries, says Shakeel Ur Rehman of Bihar-based non-profit Centre for Health and Resource Management (CHARM). The government has based all its programmes for expecting mothers on the belief that women can be safe during and after childbirth only if they have access to public health institutions, he says. Programmes like Janani Suraksha Yojana even give cash incentives to women who deliver their babies in hospitals. It allocated as much as Rs 1,700 crore for the programme in 2011-12.</p><p style="text-align: justify">Though the country has been able to reduce its MMR from 212 in 2009 to 178 in 2012, it may not be able to achieve its Millennium Development Goal (MDG). In 2000, the international community had pledged to bring down MMR by one- third. For India, the target was to reduce MMR to 109 by 2015.</p><p style="text-align: justify">To overcome the challenge, member of the Planning Commission Syeda Hameed suggested National Alliance for Maternal Health and Human Rights and Oxfam (international confederation of organisations working to find solutions to social injustices) to present their recommendations to the plan panel. The organisations are now finalising the recommendations (see ‘Experts' recommendations'). The plan panel is set to do mid-term appraisal of the 12th Five Year Plan within a few months. Implementation of the recommendations should be able to reduce MMR, she said at a national convention held recently in New Delhi.</p><p style="text-align: justify">Reduction in the country's MMR is most likely because of under-reporting of deaths, says Rehman. CHARM is currently conducting a survey at public health centres in Bihar. The non-profit has found a big gap between government data and the actual MMR. Phulwari Sharif in Patna has reported zero deaths, but the non-profit found 14 deaths in the block in a month. "The focus is only on achieving targets on paper," he says.</p><p style="text-align: justify">At present, Assam has the highest MMR of 328 in the country followed by Uttar Pradesh and Uttarakhand together at 292, according to a recently released report of the Registrar General of India. Madhya Pradesh, Chhattisgarh, Odisha, Rajasthan, Bihar and Jharkhand have MMR of 200 and above. South India, however, has shown remarkable progress. Kerala has pushed its MMR down from 150 in 1997-98 to 66 in 2012. Tamil Nadu has reduced it from 131 to 90 and Andhra Pradesh from 197 to 110 in the same period (see ‘Meeting targets').</p><p style="text-align: justify"><img src="https://im4change.in/siteadmin/tinymce/uploaded/Down to Earth.jpg" alt="Down to Earth" width="458" height="350" /> </p><p style="text-align: justify"><em>Multi-pronged approach</em></p><p style="text-align: justify">"South Indian states improved their MMR because they have more or less sorted out issues like nutrition and hygiene, which have a big influence on safe delivery," says Ritu Priya Mehrotra, professor at the Centre of Social Medicine and Community Health, Jawaharlal Nehru University, Delhi. Public health system is strong in these states.</p><p style="text-align: justify">"It is strange that the government has initiated programmes focused on public health institutions without improving medical facilities and infrastructure there," says Abhijit Das, director of Centre for Health and Social Justice, a New Delhi-based non-profit. The need is to take a multi-pronged approach, says Smita Bajpai of Gujarat-based non-profit Centre for Health Education, Training and Nutrition Awareness. "Unless the focus shifts to the root cause of the problem, it will not be resolved. Improvement is required in every sector-transport, infrastructure, nutrition and employment," she adds.</p><p style="text-align: justify">A CHARM study on maternal deaths in Bihar found 22 deaths in Phulwari Sharif and Maner blocks between 2012 and 2013. Of these, 15 women died while being taken to health centres in autorickshaws. Two were on foot. Delay in decision-making and reaching health centres was the reason for most deaths, the study states. States should improve access to free ambulances, it says.</p><p style="text-align: justify">In a country like India where midwives still cover 50 per cent of the deliveries, home delivery gets no support from the government, says Das. In the 1920s, developing countries such as Denmark and the Netherlands supported home deliveries and had lower MMR than developing countries like the US and New Zealand which believed only in institutional deliveries, he says. Sri Lanka managed to reduce its MMR to 60 in 2008 by widely using midwives for home deliveries and strengthening the health system. Centre for Global Development, a US-based research organisation, states that 97 per cent of the births in Sri Lanka are attended by skilled midwives. It also provides free medical services to all.</p><p style="text-align: justify">"India cannot provide medical service to all in public institutions. In such a scenario, how justified is it to promote only institutional deliveries?" wonders Mehrotra. She suggests integrating midwives, accredited social health activists (ASHAs) and auxiliary nurse midwives (ANMs) for delivery cases. ASHAs can counsel pregnant women; midwives, with their knowledge of the female body, can identify critical cases and perform normal deliveries; and ANMs can coordinate with health centres for institutional deliveries.</p><p style="text-align: justify">To improve the situation, the government should shift the debate from home delivery versus institutional delivery to safe delivery versus unsafe, says Rehman.</p><p style="text-align: justify"><strong>EXPERTS’ RECOMMENDATIONS</strong></p><p style="text-align: justify">Improve infrastructure at each operation theatre—availability of oxygen, provision for spinal anaesthesia, inverter and generator</p><p style="text-align: justify">Ultrasonography at each community health centre</p><p style="text-align: justify">Clear-cut norms for referring patients from one hospital to another, audit this on a regular basis</p><p style="text-align: justify">Maternal health services as per the local requirement that also protect women’s dignity</p><p style="text-align: justify">Compulsory provisioning of high-nutrition food to expecting mothers</p><p style="text-align: justify">Transparent and centralised medicine supply and procurement system</p><p style="text-align: justify">Wireless system in areas that do not have mobile connectivity</p><p style="text-align: justify">Legalise unbanked direct blood transfusion; ready list of donors to ensure blood availability in emergency situations</p><p style="text-align: justify">Source: List of demands by experts at a national convention on second generation plan on maternal health </p><p style="text-align: justify"> </p><p style="text-align: justify"><em>With inputs from Alok Gupta</em> </p>
</div>
</td>
</tr>
</table>
</div>
</div>
</div>
<div class="clear"></div>
<br><a href="http://www.downtoearth.org.in/content/delivering-safety" class="re" target="_blank">Down to Earth, 30 April, 2014, http://www.downtoearth.org.in/content/delivering-safety</a><div class="clear"></div>
<div style="padding-top: 18px;">
<p class="post-tag">Tagged with:
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=maternal mortality ratio"
title="maternal mortality ratio">
maternal mortality ratio </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=maternal deaths"
title="maternal deaths">
maternal deaths </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Health"
title="Health">
Health </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=maternal mortality"
title="maternal mortality">
maternal mortality </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Maternal Health"
title="Maternal Health">
Maternal Health </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=hospitals"
title="hospitals">
hospitals </a>
</p>
</div>
<div class="clear"></div>
<br><br>
<div class="widget-top">
<h4>Related Articles</h4>
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<ul id="recentcomments">
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/fifth-report-from-gambia-implicates-indian-drug-maker-for-contaminated-syrups-banjot-kaur.html"
title="Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur">
Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-may-have-seen-steepest-dip-in-multidimensional-poverty-among-110-nations-as-per-undp-data-nikhil-rampal.html"
title="India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal">
India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/health-among-top-three-priorities-for-indian-voters-after-jobs-and-education-survey-shows-oliver-heath-jyoti-mishra-louise-tillin-sandhya-venkateswaran.html"
title="Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran">
Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-s-stretched-health-care-system-fails-millions-in-rural-areas-battling-sickle-cell-disease-abc.html"
title="India's stretched health care system fails millions in rural areas battling sickle cell disease - ABC">
India's stretched health care system fails millions in rural areas battling sickle cell disease - ABC </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/prevalence-of-zero-food-among-infants-and-young-children-in-india-patterns-of-change-across-the-states-and-union-territories-of-india-1993-2021-the-lancet.html"
title="Prevalence of Zero-Food among infants and young children in India - The Lancet ">
Prevalence of Zero-Food among infants and young children in India - The Lancet </a>
</li>
</ul>
</div>
<div class="comment-respond" id="respond">
<a name="commentbox"> </a>
<h3 class="comment-reply-title" id="reply-title">Write Comments</h3>
<form method="post" accept-charset="utf-8" role="form" action="/latest-news-updates/delivering-safety-kundan-pandey-24858.html"><div style="display:none;"><input type="hidden" name="_method" value="POST"/></div> <form class="comment-form" id="commentform" method="post" action="#commentbox" onSubmit="return validate()"
name="cmtform">
<input type="hidden" name="cmttype" value="articlecmt"/>
<input type="hidden" name="article_id" value="24677"/>
<p class="comment-notes">Your email address will not be published. Required fields are marked <span
class="required">*</span></p>
<p class="comment-form-author">
<label for="commenterName">Name</label>
<span class="required">*</span>
<input type="text" aria-required="true" size="30"
value=""
name="commenterName" id="commenterName" required="true">
</p>
<p class="comment-form-email">
<label for="commenterEmail">Email</label> <span class="required">*</span>
<input aria-required="true" size="30" name="commenterEmail" id="commenterEmail" type="email"
value=""
required="true">
</p>
<p class="comment-form-contact">
<label for="commenterPh">Contact No.</label>
<input type="text" size="30"
value=""
name="commenterPh" id="commenterPh">
</p>
<p class="comment-form-comment">
<label for="comment">Comment</label>
<textarea aria-required="true" required="true" rows="8" cols="45" name="comment"
id="comment"></textarea>
</p>
<p class="comment-form-comment">
<label for="comment">Type the characters you see in the image below <span class="required">*</span><br><img
class="captchaImg"
src="https://im4change.in/securimage_show_art.php?tk=1760450620" alt="captcha"/>
</label>
</p>
<input type="text" name="vrcode" required="true"/>
<p class="form-submit" style="width: 200px;">
<input type="submit" value="Post Comment" id="submit" name="submit">
</p></form>
</div>
<style>
.ui-widget-content {
height: auto !important;
}
</style>
<div id="share-modal"></div>
<style>
.middleContent a{
background-color: rgba(108,172,228,.2);
}
.middleContent a:hover{
background-color: #418fde;
border-color: #418fde;
color: #000;
}
</style>
<script>
function shareArticle(article_id) {
var options = {
modal: true,
height: 'auto',
width: 600 + 'px'
};
$('#share-modal').html("");
$('#share-modal').load('https://im4change.in/share_article?article_id=' + article_id).dialog(options).dialog('open');
}
function postShare() {
var param = 'article_id=' + $("#article_id").val();
param = param + '&y_name=' + $("#y_name").val();
param = param + '&y_email=' + $("#y_email").val();
param = param + '&f_name=' + $("#f_name").val();
param = param + '&f_email=' + $("#f_email").val();
param = param + '&y_msg=' + $("#y_msg").val();
$.ajax({
type: "POST",
url: 'https://im4change.in/post_share_article',
data: param,
success: function (response) {
$('#share-modal').html("Thank You, Your message posted to ");
}
});
return false;
}
</script> </div>
</div>
<!-- Right Side Section Start -->
<!-- MAP Section START -->
<aside class="sidebar indexMarg">
<div class="ad-cell">
<a href="https://im4change.in/statemap.php" title="">
<img src="https://im4change.in/images/map_new_version.png?1582080666" alt="India State Map" class="indiamap" width="232" height="252"/> </a>
<div class="rightmapbox">
<div id="sideOne" class="docltitle"><a href="https://im4change.in/state-report/india/36" target="_blank">DOCUMENTS/
REPORTS</a></div>
<div id="sideTwo" class="statetitle"><a href="https://im4change.in/states.php"target="_blank">STATE DATA/
HDRs.</a></div>
</div>
<div class="widget widgePadTop"></div>
</div>
</aside>
<!-- MAP Section END -->
<aside class="sidebar sidePadbottom">
<div class="rightsmlbox1" >
<a href="https://im4change.in/knowledge_gateway" target="_blank" style="color: #035588;
font-size: 17px;">
KNOWLEDGE GATEWAY
</a>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/newsletter" target="_blank">
NEWSLETTER
</a>
</p>
</div>
</div>
<div class="rightsmlbox1" style="height: 325px;">
<div>
<p class="rightsmlbox1_title">
Interview with Prof. Ravi Srivastava
</p>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/video/interview-with-prof-ravi-srivastava-on-current-economic-crisis">
<img width="250" height="200" src="/images/interview_video_home.jpg" alt="Interview with Prof. Ravi Srivastava"/>
</a>
<!--
<iframe width="250" height="200" src="https://www.youtube.com/embed/MmaTlntk-wc" frameborder="0" allow="accelerometer; autoplay; encrypted-media; gyroscope; picture-in-picture" allowfullscreen=""></iframe>-->
</p>
<a href="https://im4change.in/videogallery" class="more-link CatArchalAnch1" target="_blank">
More videos
</a>
</div>
</div>
<div class="rightsmlbox1">
<div>
<!--div id="sstory" class="rightboxicons"></div--->
<p class="rightsmlbox1_title"><a href="https://im4change.in/list-success-stories" target="_blank">Success Stories</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/interviews" target="_blank">Interviews</a>
</p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a href="https://www.commoncause.in/page.php?id=10" >Donate</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/marquee"
class="isf_link more-link" title="India Focus?" style="border: 4px solid #fdd922;width: 90%;background-color: #fdd922;text-align: center;color: #000000;font-size:18px" target="_blank">India Focus</a></p> </div>
</div>
<div class="rightsmlbox1" style="height: 104px !important;">
<a href="https://im4change.in/quarterly_reports.php" target="_blank">
Quarterly Reports on Effect of Economic Slowdown on Employment in India (2008 - 2015)
</a>
</div>
<!-- <div class="rightsmlbox1">
<a href="https://play.google.com/store/apps/details?id=com.im4.im4change" target="_blank">
</a></div> -->
<!-- <section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">Most Visited</h2>
</section> -->
<!-- accordion Starts here -->
<!-- <div id="accordion" class="accordMarg">
</div> -->
<!-- accordion ends here -->
<!-- Widget Tag Cloud Starts here -->
<div id="tag_cloud-2" class="widget widget_tag_cloud">
<section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">MOST VISITED TAGS</h2>
</section>
<div class="widget-top wiPdTp">
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<div class="tagcloud">
<a href="https://im4change.in/search?qryStr=Agriculture"
target="_blank" class="tag-link-4 font4">Agriculture</a>
<a href="https://im4change.in/search?qryStr=Food Security"
target="_blank" class="tag-link-4 font4">Food Security</a>
<a href="https://im4change.in/search?qryStr=Law and Justice"
target="_blank" class="tag-link-4 font4">Law and Justice</a>
<a href="https://im4change.in/search?qryStr=Health"
target="_blank" class="tag-link-4 font4">Health</a>
<a href="https://im4change.in/search?qryStr=Right to Food"
target="_blank" class="tag-link-4 font4">Right to Food</a>
<a href="https://im4change.in/search?qryStr=Corruption"
target="_blank" class="tag-link-4 font4">Corruption</a>
<a href="https://im4change.in/search?qryStr=farming"
target="_blank" class="tag-link-4 font4">farming</a>
<a href="https://im4change.in/search?qryStr=Environment"
target="_blank" class="tag-link-4 font4">Environment</a>
<a href="https://im4change.in/search?qryStr=Right to Information"
target="_blank" class="tag-link-4 font4">Right to Information</a>
<a href="https://im4change.in/search?qryStr=NREGS"
target="_blank" class="tag-link-4 font4">NREGS</a>
<a href="https://im4change.in/search?qryStr=Human Rights"
target="_blank" class="tag-link-4 font4">Human Rights</a>
<a href="https://im4change.in/search?qryStr=Governance"
target="_blank" class="tag-link-4 font4">Governance</a>
<a href="https://im4change.in/search?qryStr=PDS"
target="_blank" class="tag-link-4 font4">PDS</a>
<a href="https://im4change.in/search?qryStr=COVID-19"
target="_blank" class="tag-link-4 font4">COVID-19</a>
<a href="https://im4change.in/search?qryStr=Land Acquisition"
target="_blank" class="tag-link-4 font4">Land Acquisition</a>
<a href="https://im4change.in/search?qryStr=mgnrega"
target="_blank" class="tag-link-4 font4">mgnrega</a>
<a href="https://im4change.in/search?qryStr=Farmers"
target="_blank" class="tag-link-4 font4">Farmers</a>
<a href="https://im4change.in/search?qryStr=transparency"
target="_blank" class="tag-link-4 font4">transparency</a>
<a href="https://im4change.in/search?qryStr=Gender"
target="_blank" class="tag-link-4 font4">Gender</a>
<a href="https://im4change.in/search?qryStr=Poverty"
target="_blank" class="tag-link-4 font4">Poverty</a>
<a href="https://im4change.in/search?qryStr=Farm Laws" target="_blank" class="tag-link-4 font4">Farm Laws
</a>
<a href="https://im4change.in/search?qryStr=Citizenship Amendment Act" target="_blank" class="tag-link-4 font4">Citizenship Amendment Act
</a>
<a href="https://im4change.in/search?qryStr=CAA NPR NRIC" target="_blank" class="tag-link-4 font4">CAA NPR NRIC
</a>
<a href="https://im4change.in/search?qryStr=Job Losses" target="_blank" class="tag-link-4 font4">Job Losses
</a>
<a href="https://im4change.in/search?qryStr=Migrant Workers" target="_blank" class="tag-link-4 font4">Migrant Workers
</a>
<a href="https://im4change.in/search?qryStr=Unemployment" target="_blank" class="tag-link-4 font4">Unemployment
</a>
<a href="https://im4change.in/search?qryStr=PMGKAY" target="_blank" class="tag-link-4 font4">PMGKAY
</a>
<a href="https://im4change.in/search?qryStr=PM-KISAN" target="_blank" class="tag-link-4 font4">PM-KISAN
</a>
<a href="https://im4change.in/search?qryStr=PM-CARES" target="_blank" class="tag-link-4 font4">PM-CARES
</a>
<a href="https://im4change.in/search?qryStr=LFPR" target="_blank" class="tag-link-4 font4">LFPR
</a>
</div>
</div>
</div>
<!-- Widget Tag Cloud Ends here -->
</aside>
<!-- Right Side Section End -->
</div>
<section class="cat-box cats-review-box footerSec">
<h2 class="cat-box-title vSec CatArcha">Video
Archives</h2>
<h2 class="cat-box-title CatArchaTitle">Archives</h2>
<div class="cat-box-content">
<div class="reviews-cat">
<div class="CatArchaDiv1">
<div class="CatArchaDiv2">
<ul>
<li>
<a href="https://im4change.in/news-alerts-57/moving-upstream-luni-fellowship.html" target="_blank">
Moving Upstream: Luni – Fellowship </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/135-million-indians-exited-multidimensional-poverty-as-per-government-figures-is-that-the-same-as-poverty-reduction.html" target="_blank">
135 Million Indians Exited “Multidimensional" Poverty as per Government... </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/explainer-why-are-tomato-prices-on-fire.html" target="_blank">
Explainer: Why are Tomato Prices on Fire? </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/nsso-survey-only-39-1-of-all-households-have-drinking-water-within-dwelling-46-7-of-rural-households-use-firewood-for-cooking.html" target="_blank">
NSSO Survey: Only 39.1% of all Households have Drinking... </a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/news-alerts-57"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/I51LYnP8BOk/1.jpg"
alt=" Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Short-Video-on-im4change-Hindi-website-Inclusive-Media-for-Change" target="_blank">
Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/kNqha-SwfIY/1.jpg"
alt=" "Session 1: Scope of IDEA and AgriStack" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-1- Scope-of-IDEA-and-AgriStack-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 1: Scope of IDEA and AgriStack" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/6kIVjlgZItk/1.jpg"
alt=" "Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-2-Farmer-Centric-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/2BeHTu0y7xc/1.jpg"
alt=" "Session 3: Future of Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-3-Future-of-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 3: Future of Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="divWidth">
<ul class="divWidthMarg">
<li>
<a href="https://im4change.in/video/Public-Spending-on-Agriculture-in-India-Source-Foundation-for-Agrarian-Studies"
title="Public Spending on Agriculture in India (Source: Foundation for Agrarian Studies)" target="_blank">
Public Spending on Agriculture in India (Source: Foundation for...</a>
</li>
<li>
<a href="https://im4change.in/video/Agrarian-Change-Seminar-Protests-against-the-New-Farm-Laws-in-India-by-Prof-Vikas-Rawal-JNU-Source-Journal-Of-Agrarian-Change"
title="Agrarian Change Seminar: 'Protests against the New Farm Laws in India' by Prof. Vikas Rawal, JNU (Source: Journal Of Agrarian Change) " target="_blank">
Agrarian Change Seminar: 'Protests against the New Farm Laws...</a>
</li>
<li>
<a href="https://im4change.in/video/Webinar-Ramrao-The-Story-of-India-Farm-Crisis-Source-Azim-Premji-University"
title="Webinar: Ramrao - The Story of India's Farm Crisis (Source: Azim Premji University)" target="_blank">
Webinar: Ramrao - The Story of India's Farm Crisis...</a>
</li>
<li>
<a href="https://im4change.in/video/water-and-agricultural-transformation-in-India"
title="Water and Agricultural Transformation in India: A Symbiotic Relationship (Source: IGIDR)" target="_blank">
Water and Agricultural Transformation in India: A Symbiotic Relationship...</a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/videogallery"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
</div>
</div>
</div>
</section> </div>
<div class="clear"></div>
<!-- Footer option Starts here -->
<div class="footer-bottom fade-in animated4">
<div class="container">
<div class="social-icons icon_flat">
<p class="SocialMargTop"> Website Developed by <a target="_blank" title="Web Development"
class="wot right"
href="http://www.ravinderkhurana.com/" rel="nofollow">
RAVINDErkHURANA.com</a></p>
</div>
<div class="alignleft">
<a
target="_blank" href="https://im4change.in/objectives-8.html"
class="link"
title="Objectives">Objectives</a> | <a
target="_blank" href="https://im4change.in/about-us-9.html"
class="link" title="About Us">About Us</a> | <a
target="_blank" href="https://im4change.in/media-workshops.php"
class="ucwords">Workshops</a> | <a
target="_blank" href="https://im4change.in/disclaimer/disclaimer-149.html"
title="Disclaimer">Disclaimer</a> </div>
</div>
</div>
<!-- Footer option ends here -->
</div>
<div id="connect">
<a target="_blank"
href="http://www.facebook.com/sharer.php?u=https://im4change.in/latest-news-updates/delivering-safety-kundan-pandey-24858.html"
title="Share on Facebook">
<img src="https://im4change.in/images/Facebook.png?1582080640" alt="share on Facebook" class="ImgBorder"/>
</a><br/>
<a target="_blank"
href="http://twitter.com/share?text=Im4change&url=https://im4change.in/latest-news-updates/delivering-safety-kundan-pandey-24858.html"
title="Share on Twitter">
<img src="https://im4change.in/images/twitter.png?1582080632" alt="Twitter" class="ImgBorder"/> </a>
<br/>
<a href="/feeds" title="RSS Feed" target="_blank">
<img src="https://im4change.in/images/rss.png?1582080632" alt="RSS" class="ImgBorder"/>
</a>
<br/>
<a class="feedback-link" id="feedbackFormLink" href="#">
<img src="https://im4change.in/images/feedback.png?1582080630" alt="Feedback" class="ImgBorder"/>
</a> <br/>
<a href="javascript:function iprl5(){var d=document,z=d.createElement('scr'+'ipt'),b=d.body,l=d.location;try{if(!b)throw(0);d.title='(Saving...) '+d.title;z.setAttribute('src',l.protocol+'//www.instapaper.com/j/WKrH3R7ORD5p?u='+encodeURIComponent(l.href)+'&t='+(new Date().getTime()));b.appendChild(z);}catch(e){alert('Please wait until the page has loaded.');}}iprl5();void(0)"
class="bookmarklet" onclick="return explain_bookmarklet();">
<img src="https://im4change.in/images/read-it-later.png?1582080632" alt="Read Later" class="ImgBorder"/> </a>
</div>
<!-- Feedback form Starts here -->
<div id="feedbackForm" class="overlay_form" class="ImgBorder">
<h2>Contact Form</h2>
<div id="contactform1">
<div id="formleft">
<form id="submitform" action="/contactus.php" method="post">
<input type="hidden" name="submitform" value="submitform"/>
<input type="hidden" name="salt_key" value="a0e0f2c6a0644a70e57ad2c96829709a"/>
<input type="hidden" name="ref" value="feedback"/>
<fieldset>
<label>Name :</label>
<input type="text" name="name" class="tbox" required/>
</fieldset>
<fieldset>
<label>Email :</label>
<input type="text" name="email" class="tbox" required/>
</fieldset>
<fieldset>
<label>Message :</label>
<textarea rows="5" cols="20" name="message" required></textarea>
</fieldset>
<fieldset>
Please enter security code
<div class="clear"></div>
<input type="text" name="vrcode" class="tbox"/>
</fieldset>
<fieldset>
<input type="submit" class="button" value="Submit"/>
<a href="#" id="closefeedbakcformLink">Close</a>
</fieldset>
</form>
</div>
<div class="clearfix"></div>
</div>
</div>
<div id="donate_popup" class="modal" style="max-width: 800px;">
<table width="100%" border="1">
<tr>
<td colspan="2" align="center">
<b>Support im4change</b>
</td>
</tr>
<tr>
<td width="25%" valign="middle">
<img src="https://im4change.in/images/logo2.jpg?1582080632" alt="" width="100%"/> </td>
<td style="padding-left:10px;padding-top:10px;">
<form action="https://im4change.in/donate" method="get">
<table width="100%" cellpadding="2" cellspacing="2">
<tr>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
10
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
100
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
1000
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
50
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
500
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
<input type="text" name="price" placeholder="?" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td colspan="3" align="right">
<input type="button" name="Pay" value="Pay"
style="width: 200px;background-color: rgb(205, 35, 36);color: #ffffff;"/>
</td>
</tr>
</table>
</form>
</td>
</tr>
</table>
</div><script type='text/javascript'>
/* <![CDATA[ */
var tievar = {'go_to': 'Go to...'};
/* ]]> */
</script>
<script src="/js/tie-scripts.js?1575549704"></script><script src="/js/bootstrap.js?1575549704"></script><script src="/js/jquery.modal.min.js?1578284310"></script><script>
$(document).ready(function() {
// tell the autocomplete function to get its data from our php script
$('#s').autocomplete({
source: "/autocomplete"
});
});
</script>
<script src="/vj-main-sw-register.js" async></script>
<script>function init(){var imgDefer=document.getElementsByTagName('img');for(var i=0;i<imgDefer.length;i++){if(imgDefer[i].getAttribute('data-src')){imgDefer[i].setAttribute('src',imgDefer[i].getAttribute('data-src'))}}}
window.onload=init;</script>
</body>
</html>'
}
$reasonPhrase = 'OK'
header - [internal], line ??
Cake\Http\ResponseEmitter::emitStatusLine() - CORE/src/Http/ResponseEmitter.php, line 148
Cake\Http\ResponseEmitter::emit() - CORE/src/Http/ResponseEmitter.php, line 54
Cake\Http\Server::emit() - CORE/src/Http/Server.php, line 141
[main] - ROOT/webroot/index.php, line 39
Warning (2): Cannot modify header information - headers already sent by (output started at /home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php:853) [CORE/src/Http/ResponseEmitter.php, line 181]
$response = object(Cake\Http\Response) {
'status' => (int) 200,
'contentType' => 'text/html',
'headers' => [
'Content-Type' => [
[maximum depth reached]
]
],
'file' => null,
'fileRange' => [],
'cookies' => object(Cake\Http\Cookie\CookieCollection) {},
'cacheDirectives' => [],
'body' => '<!DOCTYPE html>
<!--[if lt IE 7 ]>
<html class="ie ie6" lang='en'> <![endif]-->
<!--[if IE 7 ]>
<html class="ie ie7" lang='en'> <![endif]-->
<!--[if IE 8 ]>
<html class="ie ie8" lang='en'> <![endif]-->
<!--[if (gte IE 9)|!(IE)]><!-->
<html lang='en'>
<!--<![endif]-->
<head><meta http-equiv="Content-Type" content="text/html; charset=utf-8">
<title>
LATEST NEWS UPDATES | Delivering safety -Kundan Pandey </title>
<meta name="description" content="
-Down to Earth
All safe motherhood programmes of the government are focused on institutional deliveries, but health centres are in disarray. Experts suggest ways to reduce deaths during delivery
Lal Mohan, a daily wage labourer, has no clue what took his wife's..."/>
<meta name="keywords" content="maternal mortality ratio,maternal deaths,Health,maternal mortality,Maternal Health,hospitals"/>
<meta name="news_keywords" content="maternal mortality ratio,maternal deaths,Health,maternal mortality,Maternal Health,hospitals">
<link rel="alternate" type="application/rss+xml" title="ROR" href="/ror.xml"/>
<link rel="alternate" type="application/rss+xml" title="RSS 2.0" href="/feeds/"/>
<link rel="stylesheet" href="/css/bootstrap.min.css?1697864993"/> <link rel="stylesheet" href="/css/style.css?v=1.1.2"/> <link rel="stylesheet" href="/css/style-inner.css?1577045210"/> <link rel="stylesheet" id="Oswald-css"
href="https://fonts.googleapis.com/css?family=Oswald%3Aregular%2C700&ver=3.8.1" type="text/css"
media="all">
<link rel="stylesheet" href="/css/jquery.modal.min.css?1578285302"/> <script src="/js/jquery-1.10.2.js?1575549704"></script> <script src="/js/jquery-migrate.min.js?1575549704"></script> <link rel="shortcut icon" href="/favicon.ico" title="Favicon">
<link rel="stylesheet" href="/css/jquery-ui.css?1580720609"/> <script src="/js/jquery-ui.js?1575549704"></script> <link rel="preload" as="style" href="https://www.im4change.org/css/custom.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery.modal.min.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery-ui.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/li-scroller.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<!-- <link rel="preload" as="style" href="https://www.im4change.org/css/style.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous"> -->
<link rel="preload" as="style" href="https://www.im4change.org/css/style-inner.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel='dns-prefetch' href="//im4change.org/css/custom.css" crossorigin >
<link rel="preload" as="script" href="https://www.im4change.org/js/bootstrap.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.li-scroller.1.0.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.modal.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.ui.totop.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-1.10.2.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-migrate.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-ui.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/setting.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/tie-scripts.js">
<!--[if IE]>
<script type="text/javascript">jQuery(document).ready(function () {
jQuery(".menu-item").has("ul").children("a").attr("aria-haspopup", "true");
});</script>
<![endif]-->
<!--[if lt IE 9]>
<script src="/js/html5.js"></script>
<script src="/js/selectivizr-min.js"></script>
<![endif]-->
<!--[if IE 8]>
<link rel="stylesheet" type="text/css" media="all" href="/css/ie8.css"/>
<![endif]-->
<meta property="og:title" content="LATEST NEWS UPDATES | Delivering safety -Kundan Pandey" />
<meta property="og:url" content="https://im4change.in/latest-news-updates/delivering-safety-kundan-pandey-24858.html" />
<meta property="og:type" content="article" />
<meta property="og:description" content="
-Down to Earth
All safe motherhood programmes of the government are focused on institutional deliveries, but health centres are in disarray. Experts suggest ways to reduce deaths during delivery
Lal Mohan, a daily wage labourer, has no clue what took his wife's..." />
<meta property="og:image" content="" />
<meta property="fb:app_id" content="0" />
<meta name="viewport" content="width=device-width, initial-scale=1, maximum-scale=1, user-scalable=no">
<link rel="apple-touch-icon-precomposed" sizes="144x144" href="https://im4change.in/images/apple1.png">
<link rel="apple-touch-icon-precomposed" sizes="120x120" href="https://im4change.in/images/apple2.png">
<link rel="apple-touch-icon-precomposed" sizes="72x72" href="https://im4change.in/images/apple3.png">
<link rel="apple-touch-icon-precomposed" href="https://im4change.in/images/apple4.png">
<style>
.gsc-results-wrapper-overlay{
top: 38% !important;
height: 50% !important;
}
.gsc-search-button-v2{
border-color: #035588 !important;
background-color: #035588 !important;
}
.gsib_a{
height: 30px !important;
padding: 2px 8px 1px 6px !important;
}
.gsc-search-button-v2{
height: 41px !important;
}
input.gsc-input{
background: none !important;
}
@media only screen and (max-width: 600px) {
.gsc-results-wrapper-overlay{
top: 11% !important;
width: 87% !important;
left: 9% !important;
height: 43% !important;
}
.gsc-search-button-v2{
padding: 10px 10px !important;
}
.gsc-input-box{
height: 28px !important;
}
/* .gsib_a {
padding: 0px 9px 4px 9px !important;
}*/
}
@media only screen and (min-width: 1200px) and (max-width: 1920px) {
table.gsc-search-box{
width: 15% !important;
float: right !important;
margin-top: -118px !important;
}
.gsc-search-button-v2 {
padding: 6px !important;
}
}
</style>
<script>
$(function () {
$("#accordion").accordion({
event: "click hoverintent"
});
});
/*
* hoverIntent | Copyright 2011 Brian Cherne
* http://cherne.net/brian/resources/jquery.hoverIntent.html
* modified by the jQuery UI team
*/
$.event.special.hoverintent = {
setup: function () {
$(this).bind("mouseover", jQuery.event.special.hoverintent.handler);
},
teardown: function () {
$(this).unbind("mouseover", jQuery.event.special.hoverintent.handler);
},
handler: function (event) {
var currentX, currentY, timeout,
args = arguments,
target = $(event.target),
previousX = event.pageX,
previousY = event.pageY;
function track(event) {
currentX = event.pageX;
currentY = event.pageY;
}
;
function clear() {
target
.unbind("mousemove", track)
.unbind("mouseout", clear);
clearTimeout(timeout);
}
function handler() {
var prop,
orig = event;
if ((Math.abs(previousX - currentX) +
Math.abs(previousY - currentY)) < 7) {
clear();
event = $.Event("hoverintent");
for (prop in orig) {
if (!(prop in event)) {
event[prop] = orig[prop];
}
}
// Prevent accessing the original event since the new event
// is fired asynchronously and the old event is no longer
// usable (#6028)
delete event.originalEvent;
target.trigger(event);
} else {
previousX = currentX;
previousY = currentY;
timeout = setTimeout(handler, 100);
}
}
timeout = setTimeout(handler, 100);
target.bind({
mousemove: track,
mouseout: clear
});
}
};
</script>
<script type="text/javascript">
var _gaq = _gaq || [];
_gaq.push(['_setAccount', 'UA-472075-3']);
_gaq.push(['_trackPageview']);
(function () {
var ga = document.createElement('script');
ga.type = 'text/javascript';
ga.async = true;
ga.src = ('https:' == document.location.protocol ? 'https://ssl' : 'http://www') + '.google-analytics.com/ga.js';
var s = document.getElementsByTagName('script')[0];
s.parentNode.insertBefore(ga, s);
})();
</script>
<link rel="stylesheet" href="/css/custom.css?v=1.16"/> <script src="/js/jquery.ui.totop.js?1575549704"></script> <script src="/js/setting.js?1575549704"></script> <link rel="manifest" href="/manifest.json">
<meta name="theme-color" content="#616163" />
<meta name="apple-mobile-web-app-capable" content="yes">
<meta name="apple-mobile-web-app-status-bar-style" content="black">
<meta name="apple-mobile-web-app-title" content="im4change">
<link rel="apple-touch-icon" href="/icons/logo-192x192.png">
</head>
<body id="top" class="home inner blog">
<div class="background-cover"></div>
<div class="wrapper animated">
<header id="theme-header" class="header_inner" style="position: relative;">
<div class="logo inner_logo" style="left:20px !important">
<a title="Home" href="https://im4change.in/">
<img src="https://im4change.in/images/logo2.jpg?1582080632" class="logo_image" alt="im4change"/> </a>
</div>
<div class="langhindi" style="color: #000;display:none;"
href="https://im4change.in/">
<a class="more-link" href="https://im4change.in/">Home</a>
<a href="https://im4change.in/hindi/" class="langbutton ">हिन्दी</a>
</div>
<nav class="fade-in animated2" id="main-nav">
<div class="container">
<div class="main-menu">
<ul class="menu" id="menu-main">
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
style="left: -40px;"><a
target="_blank" href="https://im4change.in/">Home</a>
</li>
<li class="menu-item mega-menu menu-item-type-taxonomy mega-menu menu-item-object-category mega-menu menu-item-has-children parent-list"
style=" margin-left: -40px;"><a href="#">KNOWLEDGE GATEWAY <span class="sub-indicator"></span>
</a>
<div class="mega-menu-block background_menu" style="padding-top:25px;">
<div class="container">
<div class="mega-menu-content">
<div class="mega-menu-item">
<h3><b>Farm Crisis</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/farmers039-suicides-14.html"
class="left postionrel">Farm Suicides </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/unemployment-30.html"
class="left postionrel">Unemployment </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/rural-distress-70.html"
class="left postionrel">Rural distress </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/migration-34.html"
class="left postionrel">Migration </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/key-facts-72.html"
class="left postionrel">Key Facts </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/debt-trap-15.html"
class="left postionrel">Debt Trap </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Empowerment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/union-budget-73.html"
class="left postionrel">Union Budget And Other Economic Policies </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/forest-and-tribal-rights-61.html"
class="left postionrel">Forest and Tribal Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-education-60.html"
class="left postionrel">Right to Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-food-59.html"
class="left postionrel">Right to Food </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/displacement-3279.html"
class="left postionrel">Displacement </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-work-mg-nrega-39.html"
class="left postionrel">Right to Work (MG-NREGA) </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/gender-3280.html"
class="left postionrel">GENDER </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-information-58.html"
class="left postionrel">Right to Information </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/social-audit-48.html"
class="left postionrel">Social Audit </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Hunger / HDI</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/poverty-and-inequality-20499.html"
class="left postionrel">Poverty and inequality </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/malnutrition-41.html"
class="left postionrel">Malnutrition </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/public-health-51.html"
class="left postionrel">Public Health </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/education-50.html"
class="left postionrel">Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hunger-overview-40.html"
class="left postionrel">Hunger Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hdi-overview-45.html"
class="left postionrel">HDI Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/pds-ration-food-security-42.html"
class="left postionrel">PDS/ Ration/ Food Security </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/sdgs-113.html"
class="left postionrel">SDGs </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/mid-day-meal-scheme-mdms-53.html"
class="left postionrel">Mid Day Meal Scheme (MDMS) </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Environment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/time-bomb-ticking-52.html"
class="left postionrel">Time Bomb Ticking </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/water-and-sanitation-55.html"
class="left postionrel">Water and Sanitation </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/impact-on-agriculture-54.html"
class="left postionrel">Impact on Agriculture </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Law & Justice</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/social-justice-20500.html"
class="left postionrel">Social Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/access-to-justice-47.html"
class="left postionrel">Access to Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/human-rights-56.html"
class="left postionrel">Human Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/corruption-35.html"
class="left postionrel">Corruption </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/general-insecurity-46.html"
class="left postionrel">General Insecurity </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/disaster-relief-49.html"
class="left postionrel">Disaster & Relief </a>
</p>
</div>
</div>
</div>
</div>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page "><a target="_blank" href="https://im4change.in/nceus_reports.php">NCEUS reports</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children parent-list ">
<a target="_blank" href="https://im4change.in/about-us-9.html">About Us <span
class="sub-indicator"></span></a>
<ul class="sub-menu aboutmenu">
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/objectives-8.html">Objectives</a>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/contactus.php">Contact
Us</a></li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/about-us-9.html">About
Us</a></li>
</ul>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children ">
<a target="_blank" href="https://im4change.in/fellowships.php" title="Fellowships">Fellowships</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/media-workshops.php">Workshops</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/research.php">Research</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/links-64">Partners</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
id="menu-item-539"><a target="_blank" href="https://im4change.in/hindi/"
class="langbutton langlinkfont17">हिन्दी</a></li>
</ul>
</div> </div>
<!-- <div style="float: right;">
<script async src="https://cse.google.com/cse.js?cx=18b4f2e0f11bed3dd"></script>
<div class="gcse-search"></div>
</div> -->
<div class="search-block" style=" margin-left: 8px; margin-right: 7px;">
<form method="get" id="searchform" name="searchform"
action="https://im4change.in/search"
onsubmit="return searchvalidate();">
<button class="search-button" type="submit" value="Search"></button>
<input type="text" id="s" name="qryStr" value=""
onfocus="if (this.value == 'Search...') {this.value = '';}"
onblur="if (this.value == '') {this.value = 'Search...';}">
</form>
</div>
</nav>
</header>
<div class="container">
<div id="main-content" class=" main1 container fade-in animated3 sidebar-narrow-left">
<div class="content-wrap">
<div class="content" style="width: 900px;min-height: 500px;">
<section class="cat-box recent-box innerCatRecent">
<h1 class="cat-box-title">Delivering safety -Kundan Pandey</h1>
<a href="JavaScript:void(0);" onclick="return shareArticle(24677);">
<img src="https://im4change.in/images/email.png?1582080630" border="0" width="24" align="right" alt="Share this article"/> </a>
<a href="https://im4change.in/latest-news-updates/delivering-safety-kundan-pandey-24858/print"
rel="nofollow">
<img src="https://im4change.in/images/icon-print.png?1582080630" border="0" width="24" align="right" alt="Share this article"/>
</a>
</section>
<section class="recent-box innerCatRecent">
<small class="pb-1"><span class="dateIcn">
<img src="https://im4change.in/images/published.svg?1582080666" alt="published"/>
Published on</span><span class="text-date"> Apr 28, 2014</span>
<span
class="dateIcn">
<img src="https://im4change.in/images/modified.svg?1582080666" alt="modified"/> Modified on </span><span class="text-date"> Apr 28, 2014</span>
</small>
</section>
<div class="clear"></div>
<div style="padding-top: 10px;">
<div class="innerLineHeight">
<div class="middleContent innerInput latest-news-updates">
<table>
<tr>
<td>
<div>
<div style="text-align: justify">-Down to Earth</div><div style="text-align: justify"> </div><p style="text-align: justify"><em>All safe motherhood programmes of the government are focused on institutional deliveries, but health centres are in disarray. Experts suggest ways to reduce deaths during delivery</em></p><p style="text-align: justify">Lal Mohan, a daily wage labourer, has no clue what took his wife's life. Sarita Devi, 25, was expecting her third child, and was on way to a good hospital at Bhagalpur district in Bihar. "She was normal all through the nine months of pregnancy," he says. "When labour pains began, we took her to a community health centre (CHC), 15 km from our house in Godda district in Jharkhand. At around 11 pm, doctors advised us to take her to Sadar Hospital, 20 km from the CHC. Here again, doctors referred her to Jawaharlal Nehru Medical College and Hospital in Bhagalpur, another 70 km away." She passed away on the way to hospital.</p><p style="text-align: justify">Sarita's death is not a one-off case. In a year, hundreds of women die during or after pregnancy in the Santhal Pargana region, where Sarita lived. Child marriage is rampant in the region and girls usually become pregnant at the age of 16, says Soumik Bannerjee, health activist in Godda. Their undernourished bodies are ill-prepared for travelling to faraway places during labour pains, that too under no medical supervision or advise. Small wonder, Santhal Pargana has a high maternal mortality ratio (MMR), of more than 300 deaths per 100,000 live births, he says.</p><p style="text-align: justify">This is the result of the government's focus on only institutional deliveries, says Shakeel Ur Rehman of Bihar-based non-profit Centre for Health and Resource Management (CHARM). The government has based all its programmes for expecting mothers on the belief that women can be safe during and after childbirth only if they have access to public health institutions, he says. Programmes like Janani Suraksha Yojana even give cash incentives to women who deliver their babies in hospitals. It allocated as much as Rs 1,700 crore for the programme in 2011-12.</p><p style="text-align: justify">Though the country has been able to reduce its MMR from 212 in 2009 to 178 in 2012, it may not be able to achieve its Millennium Development Goal (MDG). In 2000, the international community had pledged to bring down MMR by one- third. For India, the target was to reduce MMR to 109 by 2015.</p><p style="text-align: justify">To overcome the challenge, member of the Planning Commission Syeda Hameed suggested National Alliance for Maternal Health and Human Rights and Oxfam (international confederation of organisations working to find solutions to social injustices) to present their recommendations to the plan panel. The organisations are now finalising the recommendations (see ‘Experts' recommendations'). The plan panel is set to do mid-term appraisal of the 12th Five Year Plan within a few months. Implementation of the recommendations should be able to reduce MMR, she said at a national convention held recently in New Delhi.</p><p style="text-align: justify">Reduction in the country's MMR is most likely because of under-reporting of deaths, says Rehman. CHARM is currently conducting a survey at public health centres in Bihar. The non-profit has found a big gap between government data and the actual MMR. Phulwari Sharif in Patna has reported zero deaths, but the non-profit found 14 deaths in the block in a month. "The focus is only on achieving targets on paper," he says.</p><p style="text-align: justify">At present, Assam has the highest MMR of 328 in the country followed by Uttar Pradesh and Uttarakhand together at 292, according to a recently released report of the Registrar General of India. Madhya Pradesh, Chhattisgarh, Odisha, Rajasthan, Bihar and Jharkhand have MMR of 200 and above. South India, however, has shown remarkable progress. Kerala has pushed its MMR down from 150 in 1997-98 to 66 in 2012. Tamil Nadu has reduced it from 131 to 90 and Andhra Pradesh from 197 to 110 in the same period (see ‘Meeting targets').</p><p style="text-align: justify"><img src="https://im4change.in/siteadmin/tinymce/uploaded/Down to Earth.jpg" alt="Down to Earth" width="458" height="350" /> </p><p style="text-align: justify"><em>Multi-pronged approach</em></p><p style="text-align: justify">"South Indian states improved their MMR because they have more or less sorted out issues like nutrition and hygiene, which have a big influence on safe delivery," says Ritu Priya Mehrotra, professor at the Centre of Social Medicine and Community Health, Jawaharlal Nehru University, Delhi. Public health system is strong in these states.</p><p style="text-align: justify">"It is strange that the government has initiated programmes focused on public health institutions without improving medical facilities and infrastructure there," says Abhijit Das, director of Centre for Health and Social Justice, a New Delhi-based non-profit. The need is to take a multi-pronged approach, says Smita Bajpai of Gujarat-based non-profit Centre for Health Education, Training and Nutrition Awareness. "Unless the focus shifts to the root cause of the problem, it will not be resolved. Improvement is required in every sector-transport, infrastructure, nutrition and employment," she adds.</p><p style="text-align: justify">A CHARM study on maternal deaths in Bihar found 22 deaths in Phulwari Sharif and Maner blocks between 2012 and 2013. Of these, 15 women died while being taken to health centres in autorickshaws. Two were on foot. Delay in decision-making and reaching health centres was the reason for most deaths, the study states. States should improve access to free ambulances, it says.</p><p style="text-align: justify">In a country like India where midwives still cover 50 per cent of the deliveries, home delivery gets no support from the government, says Das. In the 1920s, developing countries such as Denmark and the Netherlands supported home deliveries and had lower MMR than developing countries like the US and New Zealand which believed only in institutional deliveries, he says. Sri Lanka managed to reduce its MMR to 60 in 2008 by widely using midwives for home deliveries and strengthening the health system. Centre for Global Development, a US-based research organisation, states that 97 per cent of the births in Sri Lanka are attended by skilled midwives. It also provides free medical services to all.</p><p style="text-align: justify">"India cannot provide medical service to all in public institutions. In such a scenario, how justified is it to promote only institutional deliveries?" wonders Mehrotra. She suggests integrating midwives, accredited social health activists (ASHAs) and auxiliary nurse midwives (ANMs) for delivery cases. ASHAs can counsel pregnant women; midwives, with their knowledge of the female body, can identify critical cases and perform normal deliveries; and ANMs can coordinate with health centres for institutional deliveries.</p><p style="text-align: justify">To improve the situation, the government should shift the debate from home delivery versus institutional delivery to safe delivery versus unsafe, says Rehman.</p><p style="text-align: justify"><strong>EXPERTS’ RECOMMENDATIONS</strong></p><p style="text-align: justify">Improve infrastructure at each operation theatre—availability of oxygen, provision for spinal anaesthesia, inverter and generator</p><p style="text-align: justify">Ultrasonography at each community health centre</p><p style="text-align: justify">Clear-cut norms for referring patients from one hospital to another, audit this on a regular basis</p><p style="text-align: justify">Maternal health services as per the local requirement that also protect women’s dignity</p><p style="text-align: justify">Compulsory provisioning of high-nutrition food to expecting mothers</p><p style="text-align: justify">Transparent and centralised medicine supply and procurement system</p><p style="text-align: justify">Wireless system in areas that do not have mobile connectivity</p><p style="text-align: justify">Legalise unbanked direct blood transfusion; ready list of donors to ensure blood availability in emergency situations</p><p style="text-align: justify">Source: List of demands by experts at a national convention on second generation plan on maternal health </p><p style="text-align: justify"> </p><p style="text-align: justify"><em>With inputs from Alok Gupta</em> </p>
</div>
</td>
</tr>
</table>
</div>
</div>
</div>
<div class="clear"></div>
<br><a href="http://www.downtoearth.org.in/content/delivering-safety" class="re" target="_blank">Down to Earth, 30 April, 2014, http://www.downtoearth.org.in/content/delivering-safety</a><div class="clear"></div>
<div style="padding-top: 18px;">
<p class="post-tag">Tagged with:
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=maternal mortality ratio"
title="maternal mortality ratio">
maternal mortality ratio </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=maternal deaths"
title="maternal deaths">
maternal deaths </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Health"
title="Health">
Health </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=maternal mortality"
title="maternal mortality">
maternal mortality </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Maternal Health"
title="Maternal Health">
Maternal Health </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=hospitals"
title="hospitals">
hospitals </a>
</p>
</div>
<div class="clear"></div>
<br><br>
<div class="widget-top">
<h4>Related Articles</h4>
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<ul id="recentcomments">
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/fifth-report-from-gambia-implicates-indian-drug-maker-for-contaminated-syrups-banjot-kaur.html"
title="Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur">
Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-may-have-seen-steepest-dip-in-multidimensional-poverty-among-110-nations-as-per-undp-data-nikhil-rampal.html"
title="India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal">
India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/health-among-top-three-priorities-for-indian-voters-after-jobs-and-education-survey-shows-oliver-heath-jyoti-mishra-louise-tillin-sandhya-venkateswaran.html"
title="Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran">
Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-s-stretched-health-care-system-fails-millions-in-rural-areas-battling-sickle-cell-disease-abc.html"
title="India's stretched health care system fails millions in rural areas battling sickle cell disease - ABC">
India's stretched health care system fails millions in rural areas battling sickle cell disease - ABC </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/prevalence-of-zero-food-among-infants-and-young-children-in-india-patterns-of-change-across-the-states-and-union-territories-of-india-1993-2021-the-lancet.html"
title="Prevalence of Zero-Food among infants and young children in India - The Lancet ">
Prevalence of Zero-Food among infants and young children in India - The Lancet </a>
</li>
</ul>
</div>
<div class="comment-respond" id="respond">
<a name="commentbox"> </a>
<h3 class="comment-reply-title" id="reply-title">Write Comments</h3>
<form method="post" accept-charset="utf-8" role="form" action="/latest-news-updates/delivering-safety-kundan-pandey-24858.html"><div style="display:none;"><input type="hidden" name="_method" value="POST"/></div> <form class="comment-form" id="commentform" method="post" action="#commentbox" onSubmit="return validate()"
name="cmtform">
<input type="hidden" name="cmttype" value="articlecmt"/>
<input type="hidden" name="article_id" value="24677"/>
<p class="comment-notes">Your email address will not be published. Required fields are marked <span
class="required">*</span></p>
<p class="comment-form-author">
<label for="commenterName">Name</label>
<span class="required">*</span>
<input type="text" aria-required="true" size="30"
value=""
name="commenterName" id="commenterName" required="true">
</p>
<p class="comment-form-email">
<label for="commenterEmail">Email</label> <span class="required">*</span>
<input aria-required="true" size="30" name="commenterEmail" id="commenterEmail" type="email"
value=""
required="true">
</p>
<p class="comment-form-contact">
<label for="commenterPh">Contact No.</label>
<input type="text" size="30"
value=""
name="commenterPh" id="commenterPh">
</p>
<p class="comment-form-comment">
<label for="comment">Comment</label>
<textarea aria-required="true" required="true" rows="8" cols="45" name="comment"
id="comment"></textarea>
</p>
<p class="comment-form-comment">
<label for="comment">Type the characters you see in the image below <span class="required">*</span><br><img
class="captchaImg"
src="https://im4change.in/securimage_show_art.php?tk=1760450620" alt="captcha"/>
</label>
</p>
<input type="text" name="vrcode" required="true"/>
<p class="form-submit" style="width: 200px;">
<input type="submit" value="Post Comment" id="submit" name="submit">
</p></form>
</div>
<style>
.ui-widget-content {
height: auto !important;
}
</style>
<div id="share-modal"></div>
<style>
.middleContent a{
background-color: rgba(108,172,228,.2);
}
.middleContent a:hover{
background-color: #418fde;
border-color: #418fde;
color: #000;
}
</style>
<script>
function shareArticle(article_id) {
var options = {
modal: true,
height: 'auto',
width: 600 + 'px'
};
$('#share-modal').html("");
$('#share-modal').load('https://im4change.in/share_article?article_id=' + article_id).dialog(options).dialog('open');
}
function postShare() {
var param = 'article_id=' + $("#article_id").val();
param = param + '&y_name=' + $("#y_name").val();
param = param + '&y_email=' + $("#y_email").val();
param = param + '&f_name=' + $("#f_name").val();
param = param + '&f_email=' + $("#f_email").val();
param = param + '&y_msg=' + $("#y_msg").val();
$.ajax({
type: "POST",
url: 'https://im4change.in/post_share_article',
data: param,
success: function (response) {
$('#share-modal').html("Thank You, Your message posted to ");
}
});
return false;
}
</script> </div>
</div>
<!-- Right Side Section Start -->
<!-- MAP Section START -->
<aside class="sidebar indexMarg">
<div class="ad-cell">
<a href="https://im4change.in/statemap.php" title="">
<img src="https://im4change.in/images/map_new_version.png?1582080666" alt="India State Map" class="indiamap" width="232" height="252"/> </a>
<div class="rightmapbox">
<div id="sideOne" class="docltitle"><a href="https://im4change.in/state-report/india/36" target="_blank">DOCUMENTS/
REPORTS</a></div>
<div id="sideTwo" class="statetitle"><a href="https://im4change.in/states.php"target="_blank">STATE DATA/
HDRs.</a></div>
</div>
<div class="widget widgePadTop"></div>
</div>
</aside>
<!-- MAP Section END -->
<aside class="sidebar sidePadbottom">
<div class="rightsmlbox1" >
<a href="https://im4change.in/knowledge_gateway" target="_blank" style="color: #035588;
font-size: 17px;">
KNOWLEDGE GATEWAY
</a>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/newsletter" target="_blank">
NEWSLETTER
</a>
</p>
</div>
</div>
<div class="rightsmlbox1" style="height: 325px;">
<div>
<p class="rightsmlbox1_title">
Interview with Prof. Ravi Srivastava
</p>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/video/interview-with-prof-ravi-srivastava-on-current-economic-crisis">
<img width="250" height="200" src="/images/interview_video_home.jpg" alt="Interview with Prof. Ravi Srivastava"/>
</a>
<!--
<iframe width="250" height="200" src="https://www.youtube.com/embed/MmaTlntk-wc" frameborder="0" allow="accelerometer; autoplay; encrypted-media; gyroscope; picture-in-picture" allowfullscreen=""></iframe>-->
</p>
<a href="https://im4change.in/videogallery" class="more-link CatArchalAnch1" target="_blank">
More videos
</a>
</div>
</div>
<div class="rightsmlbox1">
<div>
<!--div id="sstory" class="rightboxicons"></div--->
<p class="rightsmlbox1_title"><a href="https://im4change.in/list-success-stories" target="_blank">Success Stories</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/interviews" target="_blank">Interviews</a>
</p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a href="https://www.commoncause.in/page.php?id=10" >Donate</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/marquee"
class="isf_link more-link" title="India Focus?" style="border: 4px solid #fdd922;width: 90%;background-color: #fdd922;text-align: center;color: #000000;font-size:18px" target="_blank">India Focus</a></p> </div>
</div>
<div class="rightsmlbox1" style="height: 104px !important;">
<a href="https://im4change.in/quarterly_reports.php" target="_blank">
Quarterly Reports on Effect of Economic Slowdown on Employment in India (2008 - 2015)
</a>
</div>
<!-- <div class="rightsmlbox1">
<a href="https://play.google.com/store/apps/details?id=com.im4.im4change" target="_blank">
</a></div> -->
<!-- <section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">Most Visited</h2>
</section> -->
<!-- accordion Starts here -->
<!-- <div id="accordion" class="accordMarg">
</div> -->
<!-- accordion ends here -->
<!-- Widget Tag Cloud Starts here -->
<div id="tag_cloud-2" class="widget widget_tag_cloud">
<section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">MOST VISITED TAGS</h2>
</section>
<div class="widget-top wiPdTp">
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<div class="tagcloud">
<a href="https://im4change.in/search?qryStr=Agriculture"
target="_blank" class="tag-link-4 font4">Agriculture</a>
<a href="https://im4change.in/search?qryStr=Food Security"
target="_blank" class="tag-link-4 font4">Food Security</a>
<a href="https://im4change.in/search?qryStr=Law and Justice"
target="_blank" class="tag-link-4 font4">Law and Justice</a>
<a href="https://im4change.in/search?qryStr=Health"
target="_blank" class="tag-link-4 font4">Health</a>
<a href="https://im4change.in/search?qryStr=Right to Food"
target="_blank" class="tag-link-4 font4">Right to Food</a>
<a href="https://im4change.in/search?qryStr=Corruption"
target="_blank" class="tag-link-4 font4">Corruption</a>
<a href="https://im4change.in/search?qryStr=farming"
target="_blank" class="tag-link-4 font4">farming</a>
<a href="https://im4change.in/search?qryStr=Environment"
target="_blank" class="tag-link-4 font4">Environment</a>
<a href="https://im4change.in/search?qryStr=Right to Information"
target="_blank" class="tag-link-4 font4">Right to Information</a>
<a href="https://im4change.in/search?qryStr=NREGS"
target="_blank" class="tag-link-4 font4">NREGS</a>
<a href="https://im4change.in/search?qryStr=Human Rights"
target="_blank" class="tag-link-4 font4">Human Rights</a>
<a href="https://im4change.in/search?qryStr=Governance"
target="_blank" class="tag-link-4 font4">Governance</a>
<a href="https://im4change.in/search?qryStr=PDS"
target="_blank" class="tag-link-4 font4">PDS</a>
<a href="https://im4change.in/search?qryStr=COVID-19"
target="_blank" class="tag-link-4 font4">COVID-19</a>
<a href="https://im4change.in/search?qryStr=Land Acquisition"
target="_blank" class="tag-link-4 font4">Land Acquisition</a>
<a href="https://im4change.in/search?qryStr=mgnrega"
target="_blank" class="tag-link-4 font4">mgnrega</a>
<a href="https://im4change.in/search?qryStr=Farmers"
target="_blank" class="tag-link-4 font4">Farmers</a>
<a href="https://im4change.in/search?qryStr=transparency"
target="_blank" class="tag-link-4 font4">transparency</a>
<a href="https://im4change.in/search?qryStr=Gender"
target="_blank" class="tag-link-4 font4">Gender</a>
<a href="https://im4change.in/search?qryStr=Poverty"
target="_blank" class="tag-link-4 font4">Poverty</a>
<a href="https://im4change.in/search?qryStr=Farm Laws" target="_blank" class="tag-link-4 font4">Farm Laws
</a>
<a href="https://im4change.in/search?qryStr=Citizenship Amendment Act" target="_blank" class="tag-link-4 font4">Citizenship Amendment Act
</a>
<a href="https://im4change.in/search?qryStr=CAA NPR NRIC" target="_blank" class="tag-link-4 font4">CAA NPR NRIC
</a>
<a href="https://im4change.in/search?qryStr=Job Losses" target="_blank" class="tag-link-4 font4">Job Losses
</a>
<a href="https://im4change.in/search?qryStr=Migrant Workers" target="_blank" class="tag-link-4 font4">Migrant Workers
</a>
<a href="https://im4change.in/search?qryStr=Unemployment" target="_blank" class="tag-link-4 font4">Unemployment
</a>
<a href="https://im4change.in/search?qryStr=PMGKAY" target="_blank" class="tag-link-4 font4">PMGKAY
</a>
<a href="https://im4change.in/search?qryStr=PM-KISAN" target="_blank" class="tag-link-4 font4">PM-KISAN
</a>
<a href="https://im4change.in/search?qryStr=PM-CARES" target="_blank" class="tag-link-4 font4">PM-CARES
</a>
<a href="https://im4change.in/search?qryStr=LFPR" target="_blank" class="tag-link-4 font4">LFPR
</a>
</div>
</div>
</div>
<!-- Widget Tag Cloud Ends here -->
</aside>
<!-- Right Side Section End -->
</div>
<section class="cat-box cats-review-box footerSec">
<h2 class="cat-box-title vSec CatArcha">Video
Archives</h2>
<h2 class="cat-box-title CatArchaTitle">Archives</h2>
<div class="cat-box-content">
<div class="reviews-cat">
<div class="CatArchaDiv1">
<div class="CatArchaDiv2">
<ul>
<li>
<a href="https://im4change.in/news-alerts-57/moving-upstream-luni-fellowship.html" target="_blank">
Moving Upstream: Luni – Fellowship </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/135-million-indians-exited-multidimensional-poverty-as-per-government-figures-is-that-the-same-as-poverty-reduction.html" target="_blank">
135 Million Indians Exited “Multidimensional" Poverty as per Government... </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/explainer-why-are-tomato-prices-on-fire.html" target="_blank">
Explainer: Why are Tomato Prices on Fire? </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/nsso-survey-only-39-1-of-all-households-have-drinking-water-within-dwelling-46-7-of-rural-households-use-firewood-for-cooking.html" target="_blank">
NSSO Survey: Only 39.1% of all Households have Drinking... </a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/news-alerts-57"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/I51LYnP8BOk/1.jpg"
alt=" Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Short-Video-on-im4change-Hindi-website-Inclusive-Media-for-Change" target="_blank">
Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/kNqha-SwfIY/1.jpg"
alt=" "Session 1: Scope of IDEA and AgriStack" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-1- Scope-of-IDEA-and-AgriStack-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 1: Scope of IDEA and AgriStack" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/6kIVjlgZItk/1.jpg"
alt=" "Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-2-Farmer-Centric-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/2BeHTu0y7xc/1.jpg"
alt=" "Session 3: Future of Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-3-Future-of-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 3: Future of Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="divWidth">
<ul class="divWidthMarg">
<li>
<a href="https://im4change.in/video/Public-Spending-on-Agriculture-in-India-Source-Foundation-for-Agrarian-Studies"
title="Public Spending on Agriculture in India (Source: Foundation for Agrarian Studies)" target="_blank">
Public Spending on Agriculture in India (Source: Foundation for...</a>
</li>
<li>
<a href="https://im4change.in/video/Agrarian-Change-Seminar-Protests-against-the-New-Farm-Laws-in-India-by-Prof-Vikas-Rawal-JNU-Source-Journal-Of-Agrarian-Change"
title="Agrarian Change Seminar: 'Protests against the New Farm Laws in India' by Prof. Vikas Rawal, JNU (Source: Journal Of Agrarian Change) " target="_blank">
Agrarian Change Seminar: 'Protests against the New Farm Laws...</a>
</li>
<li>
<a href="https://im4change.in/video/Webinar-Ramrao-The-Story-of-India-Farm-Crisis-Source-Azim-Premji-University"
title="Webinar: Ramrao - The Story of India's Farm Crisis (Source: Azim Premji University)" target="_blank">
Webinar: Ramrao - The Story of India's Farm Crisis...</a>
</li>
<li>
<a href="https://im4change.in/video/water-and-agricultural-transformation-in-India"
title="Water and Agricultural Transformation in India: A Symbiotic Relationship (Source: IGIDR)" target="_blank">
Water and Agricultural Transformation in India: A Symbiotic Relationship...</a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/videogallery"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
</div>
</div>
</div>
</section> </div>
<div class="clear"></div>
<!-- Footer option Starts here -->
<div class="footer-bottom fade-in animated4">
<div class="container">
<div class="social-icons icon_flat">
<p class="SocialMargTop"> Website Developed by <a target="_blank" title="Web Development"
class="wot right"
href="http://www.ravinderkhurana.com/" rel="nofollow">
RAVINDErkHURANA.com</a></p>
</div>
<div class="alignleft">
<a
target="_blank" href="https://im4change.in/objectives-8.html"
class="link"
title="Objectives">Objectives</a> | <a
target="_blank" href="https://im4change.in/about-us-9.html"
class="link" title="About Us">About Us</a> | <a
target="_blank" href="https://im4change.in/media-workshops.php"
class="ucwords">Workshops</a> | <a
target="_blank" href="https://im4change.in/disclaimer/disclaimer-149.html"
title="Disclaimer">Disclaimer</a> </div>
</div>
</div>
<!-- Footer option ends here -->
</div>
<div id="connect">
<a target="_blank"
href="http://www.facebook.com/sharer.php?u=https://im4change.in/latest-news-updates/delivering-safety-kundan-pandey-24858.html"
title="Share on Facebook">
<img src="https://im4change.in/images/Facebook.png?1582080640" alt="share on Facebook" class="ImgBorder"/>
</a><br/>
<a target="_blank"
href="http://twitter.com/share?text=Im4change&url=https://im4change.in/latest-news-updates/delivering-safety-kundan-pandey-24858.html"
title="Share on Twitter">
<img src="https://im4change.in/images/twitter.png?1582080632" alt="Twitter" class="ImgBorder"/> </a>
<br/>
<a href="/feeds" title="RSS Feed" target="_blank">
<img src="https://im4change.in/images/rss.png?1582080632" alt="RSS" class="ImgBorder"/>
</a>
<br/>
<a class="feedback-link" id="feedbackFormLink" href="#">
<img src="https://im4change.in/images/feedback.png?1582080630" alt="Feedback" class="ImgBorder"/>
</a> <br/>
<a href="javascript:function iprl5(){var d=document,z=d.createElement('scr'+'ipt'),b=d.body,l=d.location;try{if(!b)throw(0);d.title='(Saving...) '+d.title;z.setAttribute('src',l.protocol+'//www.instapaper.com/j/WKrH3R7ORD5p?u='+encodeURIComponent(l.href)+'&t='+(new Date().getTime()));b.appendChild(z);}catch(e){alert('Please wait until the page has loaded.');}}iprl5();void(0)"
class="bookmarklet" onclick="return explain_bookmarklet();">
<img src="https://im4change.in/images/read-it-later.png?1582080632" alt="Read Later" class="ImgBorder"/> </a>
</div>
<!-- Feedback form Starts here -->
<div id="feedbackForm" class="overlay_form" class="ImgBorder">
<h2>Contact Form</h2>
<div id="contactform1">
<div id="formleft">
<form id="submitform" action="/contactus.php" method="post">
<input type="hidden" name="submitform" value="submitform"/>
<input type="hidden" name="salt_key" value="a0e0f2c6a0644a70e57ad2c96829709a"/>
<input type="hidden" name="ref" value="feedback"/>
<fieldset>
<label>Name :</label>
<input type="text" name="name" class="tbox" required/>
</fieldset>
<fieldset>
<label>Email :</label>
<input type="text" name="email" class="tbox" required/>
</fieldset>
<fieldset>
<label>Message :</label>
<textarea rows="5" cols="20" name="message" required></textarea>
</fieldset>
<fieldset>
Please enter security code
<div class="clear"></div>
<input type="text" name="vrcode" class="tbox"/>
</fieldset>
<fieldset>
<input type="submit" class="button" value="Submit"/>
<a href="#" id="closefeedbakcformLink">Close</a>
</fieldset>
</form>
</div>
<div class="clearfix"></div>
</div>
</div>
<div id="donate_popup" class="modal" style="max-width: 800px;">
<table width="100%" border="1">
<tr>
<td colspan="2" align="center">
<b>Support im4change</b>
</td>
</tr>
<tr>
<td width="25%" valign="middle">
<img src="https://im4change.in/images/logo2.jpg?1582080632" alt="" width="100%"/> </td>
<td style="padding-left:10px;padding-top:10px;">
<form action="https://im4change.in/donate" method="get">
<table width="100%" cellpadding="2" cellspacing="2">
<tr>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
10
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
100
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
1000
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
50
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
500
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
<input type="text" name="price" placeholder="?" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td colspan="3" align="right">
<input type="button" name="Pay" value="Pay"
style="width: 200px;background-color: rgb(205, 35, 36);color: #ffffff;"/>
</td>
</tr>
</table>
</form>
</td>
</tr>
</table>
</div><script type='text/javascript'>
/* <![CDATA[ */
var tievar = {'go_to': 'Go to...'};
/* ]]> */
</script>
<script src="/js/tie-scripts.js?1575549704"></script><script src="/js/bootstrap.js?1575549704"></script><script src="/js/jquery.modal.min.js?1578284310"></script><script>
$(document).ready(function() {
// tell the autocomplete function to get its data from our php script
$('#s').autocomplete({
source: "/autocomplete"
});
});
</script>
<script src="/vj-main-sw-register.js" async></script>
<script>function init(){var imgDefer=document.getElementsByTagName('img');for(var i=0;i<imgDefer.length;i++){if(imgDefer[i].getAttribute('data-src')){imgDefer[i].setAttribute('src',imgDefer[i].getAttribute('data-src'))}}}
window.onload=init;</script>
</body>
</html>'
}
$cookies = []
$values = [
(int) 0 => 'text/html; charset=UTF-8'
]
$name = 'Content-Type'
$first = true
$value = 'text/html; charset=UTF-8'
header - [internal], line ??
Cake\Http\ResponseEmitter::emitHeaders() - CORE/src/Http/ResponseEmitter.php, line 181
Cake\Http\ResponseEmitter::emit() - CORE/src/Http/ResponseEmitter.php, line 55
Cake\Http\Server::emit() - CORE/src/Http/Server.php, line 141
[main] - ROOT/webroot/index.php, line 39
Published on Apr 28, 2014 Modified on Apr 28, 2014
-Down to Earth
All safe motherhood programmes of the government are focused on institutional deliveries, but health centres are in disarray. Experts suggest ways to reduce deaths during delivery
Lal Mohan, a daily wage labourer, has no clue what took his wife's life. Sarita Devi, 25, was expecting her third child, and was on way to a good hospital at Bhagalpur district in Bihar. "She was normal all through the nine months of pregnancy," he says. "When labour pains began, we took her to a community health centre (CHC), 15 km from our house in Godda district in Jharkhand. At around 11 pm, doctors advised us to take her to Sadar Hospital, 20 km from the CHC. Here again, doctors referred her to Jawaharlal Nehru Medical College and Hospital in Bhagalpur, another 70 km away." She passed away on the way to hospital.
Sarita's death is not a one-off case. In a year, hundreds of women die during or after pregnancy in the Santhal Pargana region, where Sarita lived. Child marriage is rampant in the region and girls usually become pregnant at the age of 16, says Soumik Bannerjee, health activist in Godda. Their undernourished bodies are ill-prepared for travelling to faraway places during labour pains, that too under no medical supervision or advise. Small wonder, Santhal Pargana has a high maternal mortality ratio (MMR), of more than 300 deaths per 100,000 live births, he says.
This is the result of the government's focus on only institutional deliveries, says Shakeel Ur Rehman of Bihar-based non-profit Centre for Health and Resource Management (CHARM). The government has based all its programmes for expecting mothers on the belief that women can be safe during and after childbirth only if they have access to public health institutions, he says. Programmes like Janani Suraksha Yojana even give cash incentives to women who deliver their babies in hospitals. It allocated as much as Rs 1,700 crore for the programme in 2011-12.
Though the country has been able to reduce its MMR from 212 in 2009 to 178 in 2012, it may not be able to achieve its Millennium Development Goal (MDG). In 2000, the international community had pledged to bring down MMR by one- third. For India, the target was to reduce MMR to 109 by 2015.
To overcome the challenge, member of the Planning Commission Syeda Hameed suggested National Alliance for Maternal Health and Human Rights and Oxfam (international confederation of organisations working to find solutions to social injustices) to present their recommendations to the plan panel. The organisations are now finalising the recommendations (see ‘Experts' recommendations'). The plan panel is set to do mid-term appraisal of the 12th Five Year Plan within a few months. Implementation of the recommendations should be able to reduce MMR, she said at a national convention held recently in New Delhi.
Reduction in the country's MMR is most likely because of under-reporting of deaths, says Rehman. CHARM is currently conducting a survey at public health centres in Bihar. The non-profit has found a big gap between government data and the actual MMR. Phulwari Sharif in Patna has reported zero deaths, but the non-profit found 14 deaths in the block in a month. "The focus is only on achieving targets on paper," he says.
At present, Assam has the highest MMR of 328 in the country followed by Uttar Pradesh and Uttarakhand together at 292, according to a recently released report of the Registrar General of India. Madhya Pradesh, Chhattisgarh, Odisha, Rajasthan, Bihar and Jharkhand have MMR of 200 and above. South India, however, has shown remarkable progress. Kerala has pushed its MMR down from 150 in 1997-98 to 66 in 2012. Tamil Nadu has reduced it from 131 to 90 and Andhra Pradesh from 197 to 110 in the same period (see ‘Meeting targets').
Multi-pronged approach
"South Indian states improved their MMR because they have more or less sorted out issues like nutrition and hygiene, which have a big influence on safe delivery," says Ritu Priya Mehrotra, professor at the Centre of Social Medicine and Community Health, Jawaharlal Nehru University, Delhi. Public health system is strong in these states.
"It is strange that the government has initiated programmes focused on public health institutions without improving medical facilities and infrastructure there," says Abhijit Das, director of Centre for Health and Social Justice, a New Delhi-based non-profit. The need is to take a multi-pronged approach, says Smita Bajpai of Gujarat-based non-profit Centre for Health Education, Training and Nutrition Awareness. "Unless the focus shifts to the root cause of the problem, it will not be resolved. Improvement is required in every sector-transport, infrastructure, nutrition and employment," she adds.
A CHARM study on maternal deaths in Bihar found 22 deaths in Phulwari Sharif and Maner blocks between 2012 and 2013. Of these, 15 women died while being taken to health centres in autorickshaws. Two were on foot. Delay in decision-making and reaching health centres was the reason for most deaths, the study states. States should improve access to free ambulances, it says.
In a country like India where midwives still cover 50 per cent of the deliveries, home delivery gets no support from the government, says Das. In the 1920s, developing countries such as Denmark and the Netherlands supported home deliveries and had lower MMR than developing countries like the US and New Zealand which believed only in institutional deliveries, he says. Sri Lanka managed to reduce its MMR to 60 in 2008 by widely using midwives for home deliveries and strengthening the health system. Centre for Global Development, a US-based research organisation, states that 97 per cent of the births in Sri Lanka are attended by skilled midwives. It also provides free medical services to all.
"India cannot provide medical service to all in public institutions. In such a scenario, how justified is it to promote only institutional deliveries?" wonders Mehrotra. She suggests integrating midwives, accredited social health activists (ASHAs) and auxiliary nurse midwives (ANMs) for delivery cases. ASHAs can counsel pregnant women; midwives, with their knowledge of the female body, can identify critical cases and perform normal deliveries; and ANMs can coordinate with health centres for institutional deliveries.
To improve the situation, the government should shift the debate from home delivery versus institutional delivery to safe delivery versus unsafe, says Rehman.
EXPERTS’ RECOMMENDATIONS
Improve infrastructure at each operation theatre—availability of oxygen, provision for spinal anaesthesia, inverter and generator
Ultrasonography at each community health centre
Clear-cut norms for referring patients from one hospital to another, audit this on a regular basis
Maternal health services as per the local requirement that also protect women’s dignity
Compulsory provisioning of high-nutrition food to expecting mothers
Transparent and centralised medicine supply and procurement system
Wireless system in areas that do not have mobile connectivity
Legalise unbanked direct blood transfusion; ready list of donors to ensure blood availability in emergency situations
Source: List of demands by experts at a national convention on second generation plan on maternal health
 Published on Apr 28, 2014
Published on Apr 28, 2014
 Modified on Apr 28, 2014
Modified on Apr 28, 2014
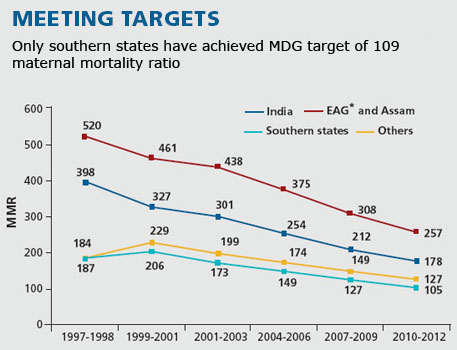









Write Comments