Deprecated (16384): The ArrayAccess methods will be removed in 4.0.0.Use getParam(), getData() and getQuery() instead. - /home/brlfuser/public_html/src/Controller/ArtileDetailController.php, line: 150
You can disable deprecation warnings by setting `Error.errorLevel` to `E_ALL & ~E_USER_DEPRECATED` in your config/app.php. [CORE/src/Core/functions.php, line 311]
deprecationWarning - CORE/src/Core/functions.php, line 311
Cake\Http\ServerRequest::offsetGet() - CORE/src/Http/ServerRequest.php, line 2421
App\Controller\ArtileDetailController::index() - APP/Controller/ArtileDetailController.php, line 150
Cake\Controller\Controller::invokeAction() - CORE/src/Controller/Controller.php, line 610
Cake\Http\ActionDispatcher::_invoke() - CORE/src/Http/ActionDispatcher.php, line 120
Cake\Http\ActionDispatcher::dispatch() - CORE/src/Http/ActionDispatcher.php, line 94
Cake\Http\BaseApplication::__invoke() - CORE/src/Http/BaseApplication.php, line 235
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Routing\Middleware\RoutingMiddleware::__invoke() - CORE/src/Routing/Middleware/RoutingMiddleware.php, line 162
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Routing\Middleware\AssetMiddleware::__invoke() - CORE/src/Routing/Middleware/AssetMiddleware.php, line 97
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Error\Middleware\ErrorHandlerMiddleware::__invoke() - CORE/src/Error/Middleware/ErrorHandlerMiddleware.php, line 96
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Http\Runner::run() - CORE/src/Http/Runner.php, line 51
Cake\Http\Server::run() - CORE/src/Http/Server.php, line 98
Deprecated (16384): The ArrayAccess methods will be removed in 4.0.0.Use getParam(), getData() and getQuery() instead. - /home/brlfuser/public_html/src/Controller/ArtileDetailController.php, line: 151
You can disable deprecation warnings by setting `Error.errorLevel` to `E_ALL & ~E_USER_DEPRECATED` in your config/app.php. [CORE/src/Core/functions.php, line 311]
deprecationWarning - CORE/src/Core/functions.php, line 311
Cake\Http\ServerRequest::offsetGet() - CORE/src/Http/ServerRequest.php, line 2421
App\Controller\ArtileDetailController::index() - APP/Controller/ArtileDetailController.php, line 151
Cake\Controller\Controller::invokeAction() - CORE/src/Controller/Controller.php, line 610
Cake\Http\ActionDispatcher::_invoke() - CORE/src/Http/ActionDispatcher.php, line 120
Cake\Http\ActionDispatcher::dispatch() - CORE/src/Http/ActionDispatcher.php, line 94
Cake\Http\BaseApplication::__invoke() - CORE/src/Http/BaseApplication.php, line 235
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Routing\Middleware\RoutingMiddleware::__invoke() - CORE/src/Routing/Middleware/RoutingMiddleware.php, line 162
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Routing\Middleware\AssetMiddleware::__invoke() - CORE/src/Routing/Middleware/AssetMiddleware.php, line 97
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Error\Middleware\ErrorHandlerMiddleware::__invoke() - CORE/src/Error/Middleware/ErrorHandlerMiddleware.php, line 96
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Http\Runner::run() - CORE/src/Http/Runner.php, line 51
Cake\Http\Server::run() - CORE/src/Http/Server.php, line 98
Warning (512): Unable to emit headers. Headers sent in file=/home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php line=853 [CORE/src/Http/ResponseEmitter.php, line 48]
if (Configure::read('debug')) {
trigger_error($message, E_USER_WARNING);
} else {
$response = object(Cake\Http\Response) {
'status' => (int) 200,
'contentType' => 'text/html',
'headers' => [
'Content-Type' => [
[maximum depth reached]
]
],
'file' => null,
'fileRange' => [],
'cookies' => object(Cake\Http\Cookie\CookieCollection) {},
'cacheDirectives' => [],
'body' => '<!DOCTYPE html>
<!--[if lt IE 7 ]>
<html class="ie ie6" lang='en'> <![endif]-->
<!--[if IE 7 ]>
<html class="ie ie7" lang='en'> <![endif]-->
<!--[if IE 8 ]>
<html class="ie ie8" lang='en'> <![endif]-->
<!--[if (gte IE 9)|!(IE)]><!-->
<html lang='en'>
<!--<![endif]-->
<head><meta http-equiv="Content-Type" content="text/html; charset=utf-8">
<title>
LATEST NEWS UPDATES | How Women Pay the Price for Population Control -Ruhi Kandhari </title>
<meta name="description" content="
-Tehelka
Despite the serious toll it takes on women's health, female sterilisation remains the most prevalent form of contraception in India.
While memories of the 21 months of Emergency in 1975-77, imposed by the then prime minister Indira Gandhi, survives even..."/>
<meta name="keywords" content="gender discrimination,Gender Equality,Reproductive Health,Contraception,Population Control,Health"/>
<meta name="news_keywords" content="gender discrimination,Gender Equality,Reproductive Health,Contraception,Population Control,Health">
<link rel="alternate" type="application/rss+xml" title="ROR" href="/ror.xml"/>
<link rel="alternate" type="application/rss+xml" title="RSS 2.0" href="/feeds/"/>
<link rel="stylesheet" href="/css/bootstrap.min.css?1697864993"/> <link rel="stylesheet" href="/css/style.css?v=1.1.2"/> <link rel="stylesheet" href="/css/style-inner.css?1577045210"/> <link rel="stylesheet" id="Oswald-css"
href="https://fonts.googleapis.com/css?family=Oswald%3Aregular%2C700&ver=3.8.1" type="text/css"
media="all">
<link rel="stylesheet" href="/css/jquery.modal.min.css?1578285302"/> <script src="/js/jquery-1.10.2.js?1575549704"></script> <script src="/js/jquery-migrate.min.js?1575549704"></script> <link rel="shortcut icon" href="/favicon.ico" title="Favicon">
<link rel="stylesheet" href="/css/jquery-ui.css?1580720609"/> <script src="/js/jquery-ui.js?1575549704"></script> <link rel="preload" as="style" href="https://www.im4change.org/css/custom.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery.modal.min.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery-ui.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/li-scroller.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<!-- <link rel="preload" as="style" href="https://www.im4change.org/css/style.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous"> -->
<link rel="preload" as="style" href="https://www.im4change.org/css/style-inner.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel='dns-prefetch' href="//im4change.org/css/custom.css" crossorigin >
<link rel="preload" as="script" href="https://www.im4change.org/js/bootstrap.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.li-scroller.1.0.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.modal.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.ui.totop.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-1.10.2.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-migrate.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-ui.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/setting.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/tie-scripts.js">
<!--[if IE]>
<script type="text/javascript">jQuery(document).ready(function () {
jQuery(".menu-item").has("ul").children("a").attr("aria-haspopup", "true");
});</script>
<![endif]-->
<!--[if lt IE 9]>
<script src="/js/html5.js"></script>
<script src="/js/selectivizr-min.js"></script>
<![endif]-->
<!--[if IE 8]>
<link rel="stylesheet" type="text/css" media="all" href="/css/ie8.css"/>
<![endif]-->
<meta property="og:title" content="LATEST NEWS UPDATES | How Women Pay the Price for Population Control -Ruhi Kandhari" />
<meta property="og:url" content="https://im4change.in/latest-news-updates/how-women-pay-the-price-for-population-control-ruhi-kandhari-4674133.html" />
<meta property="og:type" content="article" />
<meta property="og:description" content="
-Tehelka
Despite the serious toll it takes on women's health, female sterilisation remains the most prevalent form of contraception in India.
While memories of the 21 months of Emergency in 1975-77, imposed by the then prime minister Indira Gandhi, survives even..." />
<meta property="og:image" content="" />
<meta property="fb:app_id" content="0" />
<meta name="viewport" content="width=device-width, initial-scale=1, maximum-scale=1, user-scalable=no">
<link rel="apple-touch-icon-precomposed" sizes="144x144" href="https://im4change.in/images/apple1.png">
<link rel="apple-touch-icon-precomposed" sizes="120x120" href="https://im4change.in/images/apple2.png">
<link rel="apple-touch-icon-precomposed" sizes="72x72" href="https://im4change.in/images/apple3.png">
<link rel="apple-touch-icon-precomposed" href="https://im4change.in/images/apple4.png">
<style>
.gsc-results-wrapper-overlay{
top: 38% !important;
height: 50% !important;
}
.gsc-search-button-v2{
border-color: #035588 !important;
background-color: #035588 !important;
}
.gsib_a{
height: 30px !important;
padding: 2px 8px 1px 6px !important;
}
.gsc-search-button-v2{
height: 41px !important;
}
input.gsc-input{
background: none !important;
}
@media only screen and (max-width: 600px) {
.gsc-results-wrapper-overlay{
top: 11% !important;
width: 87% !important;
left: 9% !important;
height: 43% !important;
}
.gsc-search-button-v2{
padding: 10px 10px !important;
}
.gsc-input-box{
height: 28px !important;
}
/* .gsib_a {
padding: 0px 9px 4px 9px !important;
}*/
}
@media only screen and (min-width: 1200px) and (max-width: 1920px) {
table.gsc-search-box{
width: 15% !important;
float: right !important;
margin-top: -118px !important;
}
.gsc-search-button-v2 {
padding: 6px !important;
}
}
</style>
<script>
$(function () {
$("#accordion").accordion({
event: "click hoverintent"
});
});
/*
* hoverIntent | Copyright 2011 Brian Cherne
* http://cherne.net/brian/resources/jquery.hoverIntent.html
* modified by the jQuery UI team
*/
$.event.special.hoverintent = {
setup: function () {
$(this).bind("mouseover", jQuery.event.special.hoverintent.handler);
},
teardown: function () {
$(this).unbind("mouseover", jQuery.event.special.hoverintent.handler);
},
handler: function (event) {
var currentX, currentY, timeout,
args = arguments,
target = $(event.target),
previousX = event.pageX,
previousY = event.pageY;
function track(event) {
currentX = event.pageX;
currentY = event.pageY;
}
;
function clear() {
target
.unbind("mousemove", track)
.unbind("mouseout", clear);
clearTimeout(timeout);
}
function handler() {
var prop,
orig = event;
if ((Math.abs(previousX - currentX) +
Math.abs(previousY - currentY)) < 7) {
clear();
event = $.Event("hoverintent");
for (prop in orig) {
if (!(prop in event)) {
event[prop] = orig[prop];
}
}
// Prevent accessing the original event since the new event
// is fired asynchronously and the old event is no longer
// usable (#6028)
delete event.originalEvent;
target.trigger(event);
} else {
previousX = currentX;
previousY = currentY;
timeout = setTimeout(handler, 100);
}
}
timeout = setTimeout(handler, 100);
target.bind({
mousemove: track,
mouseout: clear
});
}
};
</script>
<script type="text/javascript">
var _gaq = _gaq || [];
_gaq.push(['_setAccount', 'UA-472075-3']);
_gaq.push(['_trackPageview']);
(function () {
var ga = document.createElement('script');
ga.type = 'text/javascript';
ga.async = true;
ga.src = ('https:' == document.location.protocol ? 'https://ssl' : 'http://www') + '.google-analytics.com/ga.js';
var s = document.getElementsByTagName('script')[0];
s.parentNode.insertBefore(ga, s);
})();
</script>
<link rel="stylesheet" href="/css/custom.css?v=1.16"/> <script src="/js/jquery.ui.totop.js?1575549704"></script> <script src="/js/setting.js?1575549704"></script> <link rel="manifest" href="/manifest.json">
<meta name="theme-color" content="#616163" />
<meta name="apple-mobile-web-app-capable" content="yes">
<meta name="apple-mobile-web-app-status-bar-style" content="black">
<meta name="apple-mobile-web-app-title" content="im4change">
<link rel="apple-touch-icon" href="/icons/logo-192x192.png">
</head>
<body id="top" class="home inner blog">
<div class="background-cover"></div>
<div class="wrapper animated">
<header id="theme-header" class="header_inner" style="position: relative;">
<div class="logo inner_logo" style="left:20px !important">
<a title="Home" href="https://im4change.in/">
<img src="https://im4change.in/images/logo2.jpg?1582080632" class="logo_image" alt="im4change"/> </a>
</div>
<div class="langhindi" style="color: #000;display:none;"
href="https://im4change.in/">
<a class="more-link" href="https://im4change.in/">Home</a>
<a href="https://im4change.in/hindi/" class="langbutton ">हिन्दी</a>
</div>
<nav class="fade-in animated2" id="main-nav">
<div class="container">
<div class="main-menu">
<ul class="menu" id="menu-main">
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
style="left: -40px;"><a
target="_blank" href="https://im4change.in/">Home</a>
</li>
<li class="menu-item mega-menu menu-item-type-taxonomy mega-menu menu-item-object-category mega-menu menu-item-has-children parent-list"
style=" margin-left: -40px;"><a href="#">KNOWLEDGE GATEWAY <span class="sub-indicator"></span>
</a>
<div class="mega-menu-block background_menu" style="padding-top:25px;">
<div class="container">
<div class="mega-menu-content">
<div class="mega-menu-item">
<h3><b>Farm Crisis</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/farmers039-suicides-14.html"
class="left postionrel">Farm Suicides </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/unemployment-30.html"
class="left postionrel">Unemployment </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/rural-distress-70.html"
class="left postionrel">Rural distress </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/migration-34.html"
class="left postionrel">Migration </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/key-facts-72.html"
class="left postionrel">Key Facts </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/debt-trap-15.html"
class="left postionrel">Debt Trap </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Empowerment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/union-budget-73.html"
class="left postionrel">Union Budget And Other Economic Policies </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/forest-and-tribal-rights-61.html"
class="left postionrel">Forest and Tribal Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-education-60.html"
class="left postionrel">Right to Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-food-59.html"
class="left postionrel">Right to Food </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/displacement-3279.html"
class="left postionrel">Displacement </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-work-mg-nrega-39.html"
class="left postionrel">Right to Work (MG-NREGA) </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/gender-3280.html"
class="left postionrel">GENDER </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-information-58.html"
class="left postionrel">Right to Information </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/social-audit-48.html"
class="left postionrel">Social Audit </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Hunger / HDI</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/poverty-and-inequality-20499.html"
class="left postionrel">Poverty and inequality </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/malnutrition-41.html"
class="left postionrel">Malnutrition </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/public-health-51.html"
class="left postionrel">Public Health </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/education-50.html"
class="left postionrel">Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hunger-overview-40.html"
class="left postionrel">Hunger Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hdi-overview-45.html"
class="left postionrel">HDI Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/pds-ration-food-security-42.html"
class="left postionrel">PDS/ Ration/ Food Security </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/sdgs-113.html"
class="left postionrel">SDGs </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/mid-day-meal-scheme-mdms-53.html"
class="left postionrel">Mid Day Meal Scheme (MDMS) </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Environment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/time-bomb-ticking-52.html"
class="left postionrel">Time Bomb Ticking </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/water-and-sanitation-55.html"
class="left postionrel">Water and Sanitation </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/impact-on-agriculture-54.html"
class="left postionrel">Impact on Agriculture </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Law & Justice</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/social-justice-20500.html"
class="left postionrel">Social Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/access-to-justice-47.html"
class="left postionrel">Access to Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/human-rights-56.html"
class="left postionrel">Human Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/corruption-35.html"
class="left postionrel">Corruption </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/general-insecurity-46.html"
class="left postionrel">General Insecurity </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/disaster-relief-49.html"
class="left postionrel">Disaster & Relief </a>
</p>
</div>
</div>
</div>
</div>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page "><a target="_blank" href="https://im4change.in/nceus_reports.php">NCEUS reports</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children parent-list ">
<a target="_blank" href="https://im4change.in/about-us-9.html">About Us <span
class="sub-indicator"></span></a>
<ul class="sub-menu aboutmenu">
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/objectives-8.html">Objectives</a>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/contactus.php">Contact
Us</a></li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/about-us-9.html">About
Us</a></li>
</ul>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children ">
<a target="_blank" href="https://im4change.in/fellowships.php" title="Fellowships">Fellowships</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/media-workshops.php">Workshops</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/research.php">Research</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/links-64">Partners</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
id="menu-item-539"><a target="_blank" href="https://im4change.in/hindi/"
class="langbutton langlinkfont17">हिन्दी</a></li>
</ul>
</div> </div>
<!-- <div style="float: right;">
<script async src="https://cse.google.com/cse.js?cx=18b4f2e0f11bed3dd"></script>
<div class="gcse-search"></div>
</div> -->
<div class="search-block" style=" margin-left: 8px; margin-right: 7px;">
<form method="get" id="searchform" name="searchform"
action="https://im4change.in/search"
onsubmit="return searchvalidate();">
<button class="search-button" type="submit" value="Search"></button>
<input type="text" id="s" name="qryStr" value=""
onfocus="if (this.value == 'Search...') {this.value = '';}"
onblur="if (this.value == '') {this.value = 'Search...';}">
</form>
</div>
</nav>
</header>
<div class="container">
<div id="main-content" class=" main1 container fade-in animated3 sidebar-narrow-left">
<div class="content-wrap">
<div class="content" style="width: 900px;min-height: 500px;">
<section class="cat-box recent-box innerCatRecent">
<h1 class="cat-box-title">How Women Pay the Price for Population Control -Ruhi Kandhari</h1>
<a href="JavaScript:void(0);" onclick="return shareArticle(26095);">
<img src="https://im4change.in/images/email.png?1582080630" border="0" width="24" align="right" alt="Share this article"/> </a>
<a href="https://im4change.in/latest-news-updates/how-women-pay-the-price-for-population-control-ruhi-kandhari-4674133/print"
rel="nofollow">
<img src="https://im4change.in/images/icon-print.png?1582080630" border="0" width="24" align="right" alt="Share this article"/>
</a>
</section>
<section class="recent-box innerCatRecent">
<small class="pb-1"><span class="dateIcn">
<img src="https://im4change.in/images/published.svg?1582080666" alt="published"/>
Published on</span><span class="text-date"> Oct 7, 2014</span>
<span
class="dateIcn">
<img src="https://im4change.in/images/modified.svg?1582080666" alt="modified"/> Modified on </span><span class="text-date"> Oct 7, 2014</span>
</small>
</section>
<div class="clear"></div>
<div style="padding-top: 10px;">
<div class="innerLineHeight">
<div class="middleContent innerInput latest-news-updates">
<table>
<tr>
<td>
<div>
<div align="justify">-Tehelka</div><p align="justify"><em>Despite the serious toll it takes on women's health, female sterilisation remains the most prevalent form of contraception in India. </em></p><p align="justify">While memories of the 21 months of Emergency in 1975-77, imposed by the then prime minister Indira Gandhi, survives even today in the minds of Indian men as the fear of forced sterilisation, the country's population control policies have shifted over the years since then to target the politically less powerful and vulnerable poor women. Almost the entire burden of what is euphemistically called "family planning" is today borne by women. And it has taken a toll on the health of large sections of women in the country.</p><p align="justify"><img src="https://im4change.in/siteadmin/tinymce/uploaded/Contraception.jpg" alt="Contraception" width="660" height="508" /> </p><p align="justify">In fact, the mainstay of our population control strategy comprises two methods targeted at women - tubectomy (female sterilisation surgery) and insertion of an intrauterine device (IUD) also known as Copper-T. Neither method is known to be suitable for all women. Yet, in the rush to meet targets, these methods are widely promoted and their adverse effects on women ignored. The public health infrastructure is not geared to manage contraception, the staff is not trained in counselling women or seek their informed consent, and pain is considered an acceptable side-effect.</p><p align="justify">According to the latest National Family Health Survey, conducted in 2005-06, a third of the women in the reproductive age group have undergone surgery for sterilisation and thousands have been inserted with IUDs, with or without their consent, at some point in their lives. After months of suffering pain, many women have to visit private clinics to get the IUDs removed as the government hospitals largely refuse to do so.</p><p align="justify">The World Contraception Day was observed on 26 September. The time is apt to take a hard look at India's population control policies from the perspective of the women who are forced to suffer its consequences.</p><p align="justify">Take the case of 30-year-old Rajkumari from New Delhi, who underwent tubectomy five years ago. In five years of marriage, she had three children, followed by three abortions. A social health worker appointed by the state government had convinced her that this was the only way to avoid pregnancy. Her husband, however, was never counselled to use contraception.</p><p align="justify">Since the surgery, Rajkumari has not been able to sleep peacefully on most nights. She often suffers from recurring headaches, hot flashes, night sweats and stabbing pain in her abdomen. In the month following her surgery, she visited the government hospital several times, but the doctors only prescribed her medicines to control the symptoms. "The medicines only offered temporary relief. My life has been a curse for the past five years with constant suffering," she says.</p><p align="justify">Her neighbour, 23-year-old Pushpa, also narrates a similar tale of pain. The nurse at a public health facility inserted her with an IUD after she delivered her first child. Her consent was not sought. The procedure was done after getting the consent form signed by her husband, a daily wage labourer who had studied up to Class V. He wasn't explained what an IUD is and what the form was for.</p><p align="justify">Pushpa was dizzy when she returned home. She bled profusely, became pale over time and stayed bed-ridden. Her periods lasted up to two weeks sometimes. She lost her appetite, became weak and was unable to feed her baby on most days. When she went back to the hospital, she was prescribed antibiotics and painkillers. But she continued to bleed and suffered from pain in her abdomen. It took her three months to save enough money to get the IUD removed at a private clinic.</p><p align="justify">The common known side-effects of IUDs are nausea, changes in menstrual bleeding and severe cramps. Sterilisation, on the other hand, is a risky surgery that may lead to internal infection or bleeding, injury to internal organs and even death.</p><p align="justify">There are thousands of women like Rajkumari and Pushpa who have suffered the terrible side-effects of tubectomy and IUDs.</p><p align="justify">Stuck on a wall in the lobby of the office of New Delhi-based NGO Centre for Health and Social Justice (CHSJ) is a clipping of a June 2013 article by the Bloomberg news service headlined ‘Pushing Indian Women toward Sterilisation'. It tells the story of Sumati Devi, who underwent sterilisation on an "operating table with bloody sheets". The operation was done with a rusted scalpel and she was neither counselled nor asked for her consent.</p><p align="justify">Instead, she was given some cash as an "incentive".</p><p align="justify">The article threw light on how 10 times more women than men undergo sterilisation surgeries in filthy "sterilisation camps", even though female sterilisation involves a more complicated operation than male vasectomy.</p><p align="justify">Another clipping from February 2012 headlined ‘Pregnant woman bleeds to death after sterilisation' (The Times of India) told the story of a 35-year-old pregnant woman who bled to death in Balaghat district of Madhya Pradesh while the doctors were trying to sterilise her.</p><p align="justify">She had been pregnant with twins - both girls - for 12 weeks when the operation was conducted. She died a few hours after she began bleeding on the operation table because the doctors did not follow the basic protocol of medically screening women before the sterilisation operation.</p><p align="justify">There was also a clipping of a January 2012 story titled ‘Barrack-room surgery in Bihar's backwaters' about a sterilisation camp conducted by an NGO in a hamlet in Araria district without any operation theatre, where 61 tubectomy surgeries were carried out at a breakneck speed using expired medicines.</p><p align="justify">Another clipping on display was of a March 2012 article titled ‘Freebies lengthen sterilisation queues' (The Deccan Herald) talked of how a district administration won a Tata Nano car for meeting sterilisation targets. Giving LPG connections to every family from which a woman underwent tubectomy, the administration had got over 2,000 tubectomy surgeries carried out in just three days.</p><p align="justify">According to the most recent data collected in 2012-13 under the District Level Household and Facility Survey, state governments increasingly prefer female sterilisation as a mode of family planning even though it is one of the most risky contraception methods. In Andhra Pradesh, for example, 63 percent women in the fertile age range had been operated upon in 2012-13 as compared to 60 percent in 2007-08. During the same period, the number of men who underwent sterilisation dropped from 4 to 2 percent. Similarly, in Maharashtra, the percentage of women who underwent sterilisation increased from 52 to 54 percent, while the corresponding figure for men dropped from 3 to 1 percent. In Haryana and Punjab, one-third of the women in the reproductive age range have been sterilised.</p><p align="justify">Although tubectomies involve a serious chance of surgical infections and post-operative complications, state governments continue to promote "camps" where these are conducted on thousands of women without any proper health infrastructure and in unsanitary conditions, in a hurry to meet targets. This is despite the fact that vasectomy for men is a relatively non-invasive procedure with little risk of surgical infections and the men undergoing the procedure are usually fit enough to walk only minutes later.</p><p align="justify">"The government's focus is only on terminal methods targeted at women. Men are hardly involved in the family planning programme. They need to be involved, not as targets for non-scalpel vasectomy but as partners within a gender- equality paradigm," says Dr Abhijeet Das, director of CHSJ and an assistant professor at the Department of Global Health, University of Washington, Seattle, USA. For the past two decades, Das has been observing persuasive population control programmes, advising the government and is also part of various national and international networks, including the National Alliance on Maternal Health and Human Rights, Healthwatch Forum and MenEngage, a global alliance on men and gender equality.</p><p align="justify">The 2012-13 survey also shows indicators that define the "quality of family planning services" remain abysmally low. Most women are unaware of other means of contraception and the known side-effects of sterilisation. Even when they are counselled, the counselling is manipulative as the staff has already decided which contraceptive method a woman needs. In Maharashtra, only 17 percent of the women were told about the side-effects, while the figure was 14 percent in Punjab and 11 percent in Andhra Pradesh and Haryana. According to the District Level Household & Facility Survey 2007-08, 40 percent of the women who underwent tubectomy in public health facilities across India were illiterate, indicating that tubectomy was not the "chosen" form of contraception.</p><p align="justify">Despite the problems associated with tubectomies, state governments continue to set targets for sterilisation surgeries. The reply to an RTI query showed that around 1,000 women were targeted for tubectomy in just west Delhi over the months of January, February and March this year.</p><p align="justify">The two extremes of the debate on how to stabilise the population are represented by the coercive sterilisation drive associated with Indira Gandhi's son Sanjay Gandhi during the Emergency, on the one hand, and senior Congress politician Karan Singh's statement at the 1974 World Population Conference in Bucharest, Romania, that "development is the best contraceptive", on the other. For a long time, the dominant thinking globally was in favour of coercive policies.</p><p align="justify">Internationally, this debate came to rest at the International Conference on Population and Development 1994 (ICPD 94) in Cairo, Egypt. At ICPD 94, civil society activists from around the world shared experiences of coercive population policies and convinced 179 national governments to see "population" as people, not a number. Economists like Amartya Sen had also proved by then that improvements in women's education and healthcare automatically result in smaller families without any need for authoritative population control policies.</p><p align="justify">ICPD 94 brought about a "paradigm shift". The governments agreed to abide by reproductive rights and honour gender equality while providing universal access to family planning, sexual and reproductive health services. The Indian government, too, grudgingly committed to place individuals at the centre of development. However, the state governments in India by and large do not follow this principle in practice and it is not uncommon for politicians, bureaucrats, judges and the educated, urban middle class to blame India's large population for nearly all the problems plaguing the country and favour force over cooperation.</p><p align="justify">Until ICPD 94, population was considered a dirty word - a dangerous "bomb" that would explode if not controlled. In the early 1950s, more babies were surviving in the newly-independent countries and fewer children were being born in the richer countries, leading to a fear of "overpopulation" in the Global South. This led to the formation in 1952 of two NGOs - the Population Council and the International Planned Parenthood Federation (IPPF) - in New York and Bombay, respectively. They were set up with the purpose of influencing the US government to orient the US Agency for International Development (USAID) towards population control in the Third World, alerting Americans to the danger of population "explosion" and raising funds for international birth control programmes.</p><p align="justify">An advertisement for a joint campaign by the two NGOs read: "A world of mass starvation in underdeveloped countries will be a world of chaos, riots and war. And a perfect breeding ground for communism... Our own national interests demand that we go all out to help the underdeveloped countries control their populations."</p><p align="justify">The political agenda was reinforced and validated by Stanford University Professor Paul R Ehrlich, who authored The Population Bomb in 1968. He emphasised birth control at any cost with the use of contraceptives, mass sterilisation and pre-natal sex determination (so that parents can design the family sex composition). The US government was soon convinced. In 1974, National Security Study Memorandum 200 of the National Security Council asserted that population growth in poor countries posed a problem for the security of the US. That is how the US and other industrialised countries, which had achieved lower birth rates due to improvements in education, healthcare and incomes, without any coercive population control policies, became the biggest proponents of the latter.</p><p align="justify">India could not remain unaffected by the discourse. In 1970, JRD Tata formed the Population Foundation of India with money from the Ford Foundation for population control advocacy in India. While the country's population initially focussed on vasectomy of men and stayed clear of female sterilisation, considering the risk of infection, the tide had turned by the 1980s. The infamous coercive male sterilisation drives of the Emergency period gave way to the setting of targets for female sterilisation, which continues to dominate the population control policy.</p><p align="justify">In 1992, a study by Dr Rani Bang and Dr Abhay Bang demonstrated that women had more faith in indigenous methods of contraception than the modern ones because they commonly associated the latter with adverse effects such as backache, abdominal pain, weakness and irregular or excessive menstruation. Women also found that healthcare professionals were often insensitive to these complaints and regarded them as minor and insignificant side-effects that should be ignored.</p><p align="justify">ICPD 94 was the culmination of the coming together of academics, activists and the medical community in efforts to propose an alternative perspective on population control policies. They showed how a policy of targets, incentives and disincentives under the National Family Planning Programme had made women mute recipients suffering quietly.</p><p align="justify">Among the participants at ICPD 94 was an IAS officer, AR Nanda, who was then the secretary at the Union Ministry of Health. After he returned from Cairo, he took up the mantle to reorient the population policy. The second half of the 1990s saw a new target-free approach, which focussed on combining contraception needs with providing reproductive and child health. Nanda also drafted the landmark National Population Policy (NPP) 2000, which stressed on improvements in human development, gender equality and reproductive health to stabilise population growth.</p><p align="justify">"In 1999, when I proposed the NPP, a few MPs supported the two pillars of the policy - informed choice and informed consent - but it was largely criticised in Parliament," says Nanda, who has since retired from the government, but continues to advise the National Coalition Against Two-Child Norm, an advocacy group of NGOs, academics and activists concerned with promoting policies that empower people to exercise their reproductive rights and choice.</p><p align="justify">The NPP 2000 begins with a statement that "the overriding objective of economic and social development is to improve (the) quality of life that people lead, to enhance their well-being and to provide them with opportunities and choices to become productive assets in society". The policy recommended the empowerment of women through enhanced access to education, employment opportunities and quality healthcare.</p><p align="justify">The policy, however, failed to influence a large section of politicians who continued to see population as a problem. In May 2000, when India's population crossed the one-billion mark, the then prime minister Atal Bihari Vajpayee said: "This is a serious matter that is both cause for concern and introspection - concern over the impact that a runaway population growth is bound to have on the nation's economic, natural and other resources; introspection over where we went wrong and how we can stabilise our population... If the present growth rate of our population remains unchecked, India will become the world's most populous country by the middle of this century, with people clamouring for a share of shrinking natural resources."</p><p align="justify">Opposition to NPP 2000 continued even after it was adopted. Population being a subject on the Concurrent List, the state governments are not obliged to follow anything that the Centre prescribes on population control. They have their own policies that in most cases go against NPP 2000. For instance, Uttar Pradesh introduced contraceptives such as injectables and implants, which are proven to be unsafe for women; Rajasthan promoted a lottery scheme for those who opt for sterilisation; and Bihar contracted out tubectomy surgeries to private operators and NGOs.</p><p align="justify">"The language used in talking about population stabilisation changed after ICPD 94 but the mindset remained more or less the same," says Nanda. "Even at the national level, male responsibility and gender equity were largely ignored. The state governments favour setting of targets and promoting terminal methods because the results are easy to measure."</p><p align="justify">Clearly, despite all the talk of empowering women, their reproductive autonomy - the right to choose whether to have children or not and the freedom to choose the methods of fertility management based on access to proper information - has been largely ignored in the policies and practices promoted by various governments in India.</p><p align="justify">Unfortunately, India has seen a reduced prevalence of condom use with women remaining unequal targets of the family planning burden. As the dominant, irreversible methods of population control take a toll on women's health, there is indeed a need for reorienting it towards the promotion of temporary and reversible methods such as condoms, which also provide a barrier against sexually transmitted diseases.</p><p align="justify">--</p><p align="justify">The downside of contraception</p><p align="justify">Disadvantages and side-effects of various contraceptive methods</p><p align="justify">Oral Contraceptive Pill: Nausea, mild headaches, tender breasts, spotting between periods, irregular bleeding, moodiness, vomiting within two hours of taking a pill, severe diarrhoea and vomiting for more than 24 hours</p><p align="justify">Copper-bearing IUDs: Menstrual changes in early months, longer and heavy menstrual periods, bleeding or spotting between periods, more cramps or pain during period. Uncommon sideeffects include severe cramps and pain beyond first three-five days of insertion, heavy menstrual bleeding or bleeding between periods, possibly contributing to anaemia and possibility of perforation if not inserted properly. It does not protect against sexually transmitted diseases (STDs) including HIV/AIDs. Medical procedure, including pelvic examination, is needed to insert the IUD. Occasionally, a woman faints during the insertion procedure. A trained healthcare provider must remove the IUD. The IUD may come out of the uterus possibly without the woman knowing about it (more common when the IUD is inserted soon after childbirth)</p><p align="justify">Vasectomy: Uncomfortable for two or three days, pain in scrotum, swelling and bruising and brief feeling of faintness after the procedure. Rare complications of surgery include bleeding or infection at the incision site or inside the incision, blood clots in the scrotum. No protection against STDs, including HIV/AIDs</p><p align="justify">Tubectomy: Uncommon complications include infection or bleeding at the incision, internal infection or bleeding, injury to internal organs and anaesthesia risk. No protection against STDs</p><p align="justify">Male Condom: Latex condoms may cause itching for a few people who are allergic to latex. Also, some people may be allergic to the lubricant on some brands of condoms. Small possibility that condom might slip off or break during sexual intercourse</p><p align="justify">(Source: Government reference manual)</p>
</div>
</td>
</tr>
</table>
</div>
</div>
</div>
<div class="clear"></div>
<br><a href="http://www.tehelka.com/how-women-pay-the-price-for-population-control-iod-birth-control-health-female-sterilisation/" class="re" target="_blank">Tehelka Magazine, Volume 11, Issue 41, 11 October 2014, http://www.tehelka.com/how-women-pay-the-price-for-population-control-iod-birth-control-health-female-sterilisation/</a><div class="clear"></div>
<div style="padding-top: 18px;">
<p class="post-tag">Tagged with:
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=gender discrimination"
title="gender discrimination">
gender discrimination </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Gender Equality"
title="Gender Equality">
Gender Equality </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Reproductive Health"
title="Reproductive Health">
Reproductive Health </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Contraception"
title="Contraception">
Contraception </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Population Control"
title="Population Control">
Population Control </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Health"
title="Health">
Health </a>
</p>
</div>
<div class="clear"></div>
<br><br>
<div class="widget-top">
<h4>Related Articles</h4>
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<ul id="recentcomments">
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/fifth-report-from-gambia-implicates-indian-drug-maker-for-contaminated-syrups-banjot-kaur.html"
title="Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur">
Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-may-have-seen-steepest-dip-in-multidimensional-poverty-among-110-nations-as-per-undp-data-nikhil-rampal.html"
title="India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal">
India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/health-among-top-three-priorities-for-indian-voters-after-jobs-and-education-survey-shows-oliver-heath-jyoti-mishra-louise-tillin-sandhya-venkateswaran.html"
title="Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran">
Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/prevalence-of-zero-food-among-infants-and-young-children-in-india-patterns-of-change-across-the-states-and-union-territories-of-india-1993-2021-the-lancet.html"
title="Prevalence of Zero-Food among infants and young children in India - The Lancet ">
Prevalence of Zero-Food among infants and young children in India - The Lancet </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-s-sustainability-goals-at-risk-because-of-extreme-heatwaves-carbon-copy.html"
title="India's Sustainability Goals at Risk Because of Extreme Heatwaves - Carbon Copy">
India's Sustainability Goals at Risk Because of Extreme Heatwaves - Carbon Copy </a>
</li>
</ul>
</div>
<div class="comment-respond" id="respond">
<a name="commentbox"> </a>
<h3 class="comment-reply-title" id="reply-title">Write Comments</h3>
<form method="post" accept-charset="utf-8" role="form" action="/latest-news-updates/how-women-pay-the-price-for-population-control-ruhi-kandhari-4674133.html"><div style="display:none;"><input type="hidden" name="_method" value="POST"/></div> <form class="comment-form" id="commentform" method="post" action="#commentbox" onSubmit="return validate()"
name="cmtform">
<input type="hidden" name="cmttype" value="articlecmt"/>
<input type="hidden" name="article_id" value="26095"/>
<p class="comment-notes">Your email address will not be published. Required fields are marked <span
class="required">*</span></p>
<p class="comment-form-author">
<label for="commenterName">Name</label>
<span class="required">*</span>
<input type="text" aria-required="true" size="30"
value=""
name="commenterName" id="commenterName" required="true">
</p>
<p class="comment-form-email">
<label for="commenterEmail">Email</label> <span class="required">*</span>
<input aria-required="true" size="30" name="commenterEmail" id="commenterEmail" type="email"
value=""
required="true">
</p>
<p class="comment-form-contact">
<label for="commenterPh">Contact No.</label>
<input type="text" size="30"
value=""
name="commenterPh" id="commenterPh">
</p>
<p class="comment-form-comment">
<label for="comment">Comment</label>
<textarea aria-required="true" required="true" rows="8" cols="45" name="comment"
id="comment"></textarea>
</p>
<p class="comment-form-comment">
<label for="comment">Type the characters you see in the image below <span class="required">*</span><br><img
class="captchaImg"
src="https://im4change.in/securimage_show_art.php?tk=1115961128" alt="captcha"/>
</label>
</p>
<input type="text" name="vrcode" required="true"/>
<p class="form-submit" style="width: 200px;">
<input type="submit" value="Post Comment" id="submit" name="submit">
</p></form>
</div>
<style>
.ui-widget-content {
height: auto !important;
}
</style>
<div id="share-modal"></div>
<style>
.middleContent a{
background-color: rgba(108,172,228,.2);
}
.middleContent a:hover{
background-color: #418fde;
border-color: #418fde;
color: #000;
}
</style>
<script>
function shareArticle(article_id) {
var options = {
modal: true,
height: 'auto',
width: 600 + 'px'
};
$('#share-modal').html("");
$('#share-modal').load('https://im4change.in/share_article?article_id=' + article_id).dialog(options).dialog('open');
}
function postShare() {
var param = 'article_id=' + $("#article_id").val();
param = param + '&y_name=' + $("#y_name").val();
param = param + '&y_email=' + $("#y_email").val();
param = param + '&f_name=' + $("#f_name").val();
param = param + '&f_email=' + $("#f_email").val();
param = param + '&y_msg=' + $("#y_msg").val();
$.ajax({
type: "POST",
url: 'https://im4change.in/post_share_article',
data: param,
success: function (response) {
$('#share-modal').html("Thank You, Your message posted to ");
}
});
return false;
}
</script> </div>
</div>
<!-- Right Side Section Start -->
<!-- MAP Section START -->
<aside class="sidebar indexMarg">
<div class="ad-cell">
<a href="https://im4change.in/statemap.php" title="">
<img src="https://im4change.in/images/map_new_version.png?1582080666" alt="India State Map" class="indiamap" width="232" height="252"/> </a>
<div class="rightmapbox">
<div id="sideOne" class="docltitle"><a href="https://im4change.in/state-report/india/36" target="_blank">DOCUMENTS/
REPORTS</a></div>
<div id="sideTwo" class="statetitle"><a href="https://im4change.in/states.php"target="_blank">STATE DATA/
HDRs.</a></div>
</div>
<div class="widget widgePadTop"></div>
</div>
</aside>
<!-- MAP Section END -->
<aside class="sidebar sidePadbottom">
<div class="rightsmlbox1" >
<a href="https://im4change.in/knowledge_gateway" target="_blank" style="color: #035588;
font-size: 17px;">
KNOWLEDGE GATEWAY
</a>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/newsletter" target="_blank">
NEWSLETTER
</a>
</p>
</div>
</div>
<div class="rightsmlbox1" style="height: 325px;">
<div>
<p class="rightsmlbox1_title">
Interview with Prof. Ravi Srivastava
</p>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/video/interview-with-prof-ravi-srivastava-on-current-economic-crisis">
<img width="250" height="200" src="/images/interview_video_home.jpg" alt="Interview with Prof. Ravi Srivastava"/>
</a>
<!--
<iframe width="250" height="200" src="https://www.youtube.com/embed/MmaTlntk-wc" frameborder="0" allow="accelerometer; autoplay; encrypted-media; gyroscope; picture-in-picture" allowfullscreen=""></iframe>-->
</p>
<a href="https://im4change.in/videogallery" class="more-link CatArchalAnch1" target="_blank">
More videos
</a>
</div>
</div>
<div class="rightsmlbox1">
<div>
<!--div id="sstory" class="rightboxicons"></div--->
<p class="rightsmlbox1_title"><a href="https://im4change.in/list-success-stories" target="_blank">Success Stories</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/interviews" target="_blank">Interviews</a>
</p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a href="https://www.commoncause.in/page.php?id=10" >Donate</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/marquee"
class="isf_link more-link" title="India Focus?" style="border: 4px solid #fdd922;width: 90%;background-color: #fdd922;text-align: center;color: #000000;font-size:18px" target="_blank">India Focus</a></p> </div>
</div>
<div class="rightsmlbox1" style="height: 104px !important;">
<a href="https://im4change.in/quarterly_reports.php" target="_blank">
Quarterly Reports on Effect of Economic Slowdown on Employment in India (2008 - 2015)
</a>
</div>
<!-- <div class="rightsmlbox1">
<a href="https://play.google.com/store/apps/details?id=com.im4.im4change" target="_blank">
</a></div> -->
<!-- <section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">Most Visited</h2>
</section> -->
<!-- accordion Starts here -->
<!-- <div id="accordion" class="accordMarg">
</div> -->
<!-- accordion ends here -->
<!-- Widget Tag Cloud Starts here -->
<div id="tag_cloud-2" class="widget widget_tag_cloud">
<section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">MOST VISITED TAGS</h2>
</section>
<div class="widget-top wiPdTp">
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<div class="tagcloud">
<a href="https://im4change.in/search?qryStr=Agriculture"
target="_blank" class="tag-link-4 font4">Agriculture</a>
<a href="https://im4change.in/search?qryStr=Food Security"
target="_blank" class="tag-link-4 font4">Food Security</a>
<a href="https://im4change.in/search?qryStr=Law and Justice"
target="_blank" class="tag-link-4 font4">Law and Justice</a>
<a href="https://im4change.in/search?qryStr=Health"
target="_blank" class="tag-link-4 font4">Health</a>
<a href="https://im4change.in/search?qryStr=Right to Food"
target="_blank" class="tag-link-4 font4">Right to Food</a>
<a href="https://im4change.in/search?qryStr=Corruption"
target="_blank" class="tag-link-4 font4">Corruption</a>
<a href="https://im4change.in/search?qryStr=farming"
target="_blank" class="tag-link-4 font4">farming</a>
<a href="https://im4change.in/search?qryStr=Environment"
target="_blank" class="tag-link-4 font4">Environment</a>
<a href="https://im4change.in/search?qryStr=Right to Information"
target="_blank" class="tag-link-4 font4">Right to Information</a>
<a href="https://im4change.in/search?qryStr=NREGS"
target="_blank" class="tag-link-4 font4">NREGS</a>
<a href="https://im4change.in/search?qryStr=Human Rights"
target="_blank" class="tag-link-4 font4">Human Rights</a>
<a href="https://im4change.in/search?qryStr=Governance"
target="_blank" class="tag-link-4 font4">Governance</a>
<a href="https://im4change.in/search?qryStr=PDS"
target="_blank" class="tag-link-4 font4">PDS</a>
<a href="https://im4change.in/search?qryStr=COVID-19"
target="_blank" class="tag-link-4 font4">COVID-19</a>
<a href="https://im4change.in/search?qryStr=Land Acquisition"
target="_blank" class="tag-link-4 font4">Land Acquisition</a>
<a href="https://im4change.in/search?qryStr=mgnrega"
target="_blank" class="tag-link-4 font4">mgnrega</a>
<a href="https://im4change.in/search?qryStr=Farmers"
target="_blank" class="tag-link-4 font4">Farmers</a>
<a href="https://im4change.in/search?qryStr=transparency"
target="_blank" class="tag-link-4 font4">transparency</a>
<a href="https://im4change.in/search?qryStr=Gender"
target="_blank" class="tag-link-4 font4">Gender</a>
<a href="https://im4change.in/search?qryStr=Poverty"
target="_blank" class="tag-link-4 font4">Poverty</a>
<a href="https://im4change.in/search?qryStr=Farm Laws" target="_blank" class="tag-link-4 font4">Farm Laws
</a>
<a href="https://im4change.in/search?qryStr=Citizenship Amendment Act" target="_blank" class="tag-link-4 font4">Citizenship Amendment Act
</a>
<a href="https://im4change.in/search?qryStr=CAA NPR NRIC" target="_blank" class="tag-link-4 font4">CAA NPR NRIC
</a>
<a href="https://im4change.in/search?qryStr=Job Losses" target="_blank" class="tag-link-4 font4">Job Losses
</a>
<a href="https://im4change.in/search?qryStr=Migrant Workers" target="_blank" class="tag-link-4 font4">Migrant Workers
</a>
<a href="https://im4change.in/search?qryStr=Unemployment" target="_blank" class="tag-link-4 font4">Unemployment
</a>
<a href="https://im4change.in/search?qryStr=PMGKAY" target="_blank" class="tag-link-4 font4">PMGKAY
</a>
<a href="https://im4change.in/search?qryStr=PM-KISAN" target="_blank" class="tag-link-4 font4">PM-KISAN
</a>
<a href="https://im4change.in/search?qryStr=PM-CARES" target="_blank" class="tag-link-4 font4">PM-CARES
</a>
<a href="https://im4change.in/search?qryStr=LFPR" target="_blank" class="tag-link-4 font4">LFPR
</a>
</div>
</div>
</div>
<!-- Widget Tag Cloud Ends here -->
</aside>
<!-- Right Side Section End -->
</div>
<section class="cat-box cats-review-box footerSec">
<h2 class="cat-box-title vSec CatArcha">Video
Archives</h2>
<h2 class="cat-box-title CatArchaTitle">Archives</h2>
<div class="cat-box-content">
<div class="reviews-cat">
<div class="CatArchaDiv1">
<div class="CatArchaDiv2">
<ul>
<li>
<a href="https://im4change.in/news-alerts-57/moving-upstream-luni-fellowship.html" target="_blank">
Moving Upstream: Luni – Fellowship </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/135-million-indians-exited-multidimensional-poverty-as-per-government-figures-is-that-the-same-as-poverty-reduction.html" target="_blank">
135 Million Indians Exited “Multidimensional" Poverty as per Government... </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/explainer-why-are-tomato-prices-on-fire.html" target="_blank">
Explainer: Why are Tomato Prices on Fire? </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/nsso-survey-only-39-1-of-all-households-have-drinking-water-within-dwelling-46-7-of-rural-households-use-firewood-for-cooking.html" target="_blank">
NSSO Survey: Only 39.1% of all Households have Drinking... </a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/news-alerts-57"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/I51LYnP8BOk/1.jpg"
alt=" Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Short-Video-on-im4change-Hindi-website-Inclusive-Media-for-Change" target="_blank">
Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/kNqha-SwfIY/1.jpg"
alt=" "Session 1: Scope of IDEA and AgriStack" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-1- Scope-of-IDEA-and-AgriStack-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 1: Scope of IDEA and AgriStack" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/6kIVjlgZItk/1.jpg"
alt=" "Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-2-Farmer-Centric-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/2BeHTu0y7xc/1.jpg"
alt=" "Session 3: Future of Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-3-Future-of-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 3: Future of Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="divWidth">
<ul class="divWidthMarg">
<li>
<a href="https://im4change.in/video/Public-Spending-on-Agriculture-in-India-Source-Foundation-for-Agrarian-Studies"
title="Public Spending on Agriculture in India (Source: Foundation for Agrarian Studies)" target="_blank">
Public Spending on Agriculture in India (Source: Foundation for...</a>
</li>
<li>
<a href="https://im4change.in/video/Agrarian-Change-Seminar-Protests-against-the-New-Farm-Laws-in-India-by-Prof-Vikas-Rawal-JNU-Source-Journal-Of-Agrarian-Change"
title="Agrarian Change Seminar: 'Protests against the New Farm Laws in India' by Prof. Vikas Rawal, JNU (Source: Journal Of Agrarian Change) " target="_blank">
Agrarian Change Seminar: 'Protests against the New Farm Laws...</a>
</li>
<li>
<a href="https://im4change.in/video/Webinar-Ramrao-The-Story-of-India-Farm-Crisis-Source-Azim-Premji-University"
title="Webinar: Ramrao - The Story of India's Farm Crisis (Source: Azim Premji University)" target="_blank">
Webinar: Ramrao - The Story of India's Farm Crisis...</a>
</li>
<li>
<a href="https://im4change.in/video/water-and-agricultural-transformation-in-India"
title="Water and Agricultural Transformation in India: A Symbiotic Relationship (Source: IGIDR)" target="_blank">
Water and Agricultural Transformation in India: A Symbiotic Relationship...</a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/videogallery"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
</div>
</div>
</div>
</section> </div>
<div class="clear"></div>
<!-- Footer option Starts here -->
<div class="footer-bottom fade-in animated4">
<div class="container">
<div class="social-icons icon_flat">
<p class="SocialMargTop"> Website Developed by <a target="_blank" title="Web Development"
class="wot right"
href="http://www.ravinderkhurana.com/" rel="nofollow">
RAVINDErkHURANA.com</a></p>
</div>
<div class="alignleft">
<a
target="_blank" href="https://im4change.in/objectives-8.html"
class="link"
title="Objectives">Objectives</a> | <a
target="_blank" href="https://im4change.in/about-us-9.html"
class="link" title="About Us">About Us</a> | <a
target="_blank" href="https://im4change.in/media-workshops.php"
class="ucwords">Workshops</a> | <a
target="_blank" href="https://im4change.in/disclaimer/disclaimer-149.html"
title="Disclaimer">Disclaimer</a> </div>
</div>
</div>
<!-- Footer option ends here -->
</div>
<div id="connect">
<a target="_blank"
href="http://www.facebook.com/sharer.php?u=https://im4change.in/latest-news-updates/how-women-pay-the-price-for-population-control-ruhi-kandhari-4674133.html"
title="Share on Facebook">
<img src="https://im4change.in/images/Facebook.png?1582080640" alt="share on Facebook" class="ImgBorder"/>
</a><br/>
<a target="_blank"
href="http://twitter.com/share?text=Im4change&url=https://im4change.in/latest-news-updates/how-women-pay-the-price-for-population-control-ruhi-kandhari-4674133.html"
title="Share on Twitter">
<img src="https://im4change.in/images/twitter.png?1582080632" alt="Twitter" class="ImgBorder"/> </a>
<br/>
<a href="/feeds" title="RSS Feed" target="_blank">
<img src="https://im4change.in/images/rss.png?1582080632" alt="RSS" class="ImgBorder"/>
</a>
<br/>
<a class="feedback-link" id="feedbackFormLink" href="#">
<img src="https://im4change.in/images/feedback.png?1582080630" alt="Feedback" class="ImgBorder"/>
</a> <br/>
<a href="javascript:function iprl5(){var d=document,z=d.createElement('scr'+'ipt'),b=d.body,l=d.location;try{if(!b)throw(0);d.title='(Saving...) '+d.title;z.setAttribute('src',l.protocol+'//www.instapaper.com/j/WKrH3R7ORD5p?u='+encodeURIComponent(l.href)+'&t='+(new Date().getTime()));b.appendChild(z);}catch(e){alert('Please wait until the page has loaded.');}}iprl5();void(0)"
class="bookmarklet" onclick="return explain_bookmarklet();">
<img src="https://im4change.in/images/read-it-later.png?1582080632" alt="Read Later" class="ImgBorder"/> </a>
</div>
<!-- Feedback form Starts here -->
<div id="feedbackForm" class="overlay_form" class="ImgBorder">
<h2>Contact Form</h2>
<div id="contactform1">
<div id="formleft">
<form id="submitform" action="/contactus.php" method="post">
<input type="hidden" name="submitform" value="submitform"/>
<input type="hidden" name="salt_key" value="a0e0f2c6a0644a70e57ad2c96829709a"/>
<input type="hidden" name="ref" value="feedback"/>
<fieldset>
<label>Name :</label>
<input type="text" name="name" class="tbox" required/>
</fieldset>
<fieldset>
<label>Email :</label>
<input type="text" name="email" class="tbox" required/>
</fieldset>
<fieldset>
<label>Message :</label>
<textarea rows="5" cols="20" name="message" required></textarea>
</fieldset>
<fieldset>
Please enter security code
<div class="clear"></div>
<input type="text" name="vrcode" class="tbox"/>
</fieldset>
<fieldset>
<input type="submit" class="button" value="Submit"/>
<a href="#" id="closefeedbakcformLink">Close</a>
</fieldset>
</form>
</div>
<div class="clearfix"></div>
</div>
</div>
<div id="donate_popup" class="modal" style="max-width: 800px;">
<table width="100%" border="1">
<tr>
<td colspan="2" align="center">
<b>Support im4change</b>
</td>
</tr>
<tr>
<td width="25%" valign="middle">
<img src="https://im4change.in/images/logo2.jpg?1582080632" alt="" width="100%"/> </td>
<td style="padding-left:10px;padding-top:10px;">
<form action="https://im4change.in/donate" method="get">
<table width="100%" cellpadding="2" cellspacing="2">
<tr>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
10
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
100
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
1000
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
50
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
500
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
<input type="text" name="price" placeholder="?" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td colspan="3" align="right">
<input type="button" name="Pay" value="Pay"
style="width: 200px;background-color: rgb(205, 35, 36);color: #ffffff;"/>
</td>
</tr>
</table>
</form>
</td>
</tr>
</table>
</div><script type='text/javascript'>
/* <![CDATA[ */
var tievar = {'go_to': 'Go to...'};
/* ]]> */
</script>
<script src="/js/tie-scripts.js?1575549704"></script><script src="/js/bootstrap.js?1575549704"></script><script src="/js/jquery.modal.min.js?1578284310"></script><script>
$(document).ready(function() {
// tell the autocomplete function to get its data from our php script
$('#s').autocomplete({
source: "/autocomplete"
});
});
</script>
<script src="/vj-main-sw-register.js" async></script>
<script>function init(){var imgDefer=document.getElementsByTagName('img');for(var i=0;i<imgDefer.length;i++){if(imgDefer[i].getAttribute('data-src')){imgDefer[i].setAttribute('src',imgDefer[i].getAttribute('data-src'))}}}
window.onload=init;</script>
</body>
</html>'
}
$maxBufferLength = (int) 8192
$file = '/home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php'
$line = (int) 853
$message = 'Unable to emit headers. Headers sent in file=/home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php line=853'
Cake\Http\ResponseEmitter::emit() - CORE/src/Http/ResponseEmitter.php, line 48
Cake\Http\Server::emit() - CORE/src/Http/Server.php, line 141
[main] - ROOT/webroot/index.php, line 39
Warning (2): Cannot modify header information - headers already sent by (output started at /home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php:853) [CORE/src/Http/ResponseEmitter.php, line 148]
$response = object(Cake\Http\Response) {
'status' => (int) 200,
'contentType' => 'text/html',
'headers' => [
'Content-Type' => [
[maximum depth reached]
]
],
'file' => null,
'fileRange' => [],
'cookies' => object(Cake\Http\Cookie\CookieCollection) {},
'cacheDirectives' => [],
'body' => '<!DOCTYPE html>
<!--[if lt IE 7 ]>
<html class="ie ie6" lang='en'> <![endif]-->
<!--[if IE 7 ]>
<html class="ie ie7" lang='en'> <![endif]-->
<!--[if IE 8 ]>
<html class="ie ie8" lang='en'> <![endif]-->
<!--[if (gte IE 9)|!(IE)]><!-->
<html lang='en'>
<!--<![endif]-->
<head><meta http-equiv="Content-Type" content="text/html; charset=utf-8">
<title>
LATEST NEWS UPDATES | How Women Pay the Price for Population Control -Ruhi Kandhari </title>
<meta name="description" content="
-Tehelka
Despite the serious toll it takes on women's health, female sterilisation remains the most prevalent form of contraception in India.
While memories of the 21 months of Emergency in 1975-77, imposed by the then prime minister Indira Gandhi, survives even..."/>
<meta name="keywords" content="gender discrimination,Gender Equality,Reproductive Health,Contraception,Population Control,Health"/>
<meta name="news_keywords" content="gender discrimination,Gender Equality,Reproductive Health,Contraception,Population Control,Health">
<link rel="alternate" type="application/rss+xml" title="ROR" href="/ror.xml"/>
<link rel="alternate" type="application/rss+xml" title="RSS 2.0" href="/feeds/"/>
<link rel="stylesheet" href="/css/bootstrap.min.css?1697864993"/> <link rel="stylesheet" href="/css/style.css?v=1.1.2"/> <link rel="stylesheet" href="/css/style-inner.css?1577045210"/> <link rel="stylesheet" id="Oswald-css"
href="https://fonts.googleapis.com/css?family=Oswald%3Aregular%2C700&ver=3.8.1" type="text/css"
media="all">
<link rel="stylesheet" href="/css/jquery.modal.min.css?1578285302"/> <script src="/js/jquery-1.10.2.js?1575549704"></script> <script src="/js/jquery-migrate.min.js?1575549704"></script> <link rel="shortcut icon" href="/favicon.ico" title="Favicon">
<link rel="stylesheet" href="/css/jquery-ui.css?1580720609"/> <script src="/js/jquery-ui.js?1575549704"></script> <link rel="preload" as="style" href="https://www.im4change.org/css/custom.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery.modal.min.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery-ui.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/li-scroller.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<!-- <link rel="preload" as="style" href="https://www.im4change.org/css/style.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous"> -->
<link rel="preload" as="style" href="https://www.im4change.org/css/style-inner.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel='dns-prefetch' href="//im4change.org/css/custom.css" crossorigin >
<link rel="preload" as="script" href="https://www.im4change.org/js/bootstrap.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.li-scroller.1.0.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.modal.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.ui.totop.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-1.10.2.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-migrate.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-ui.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/setting.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/tie-scripts.js">
<!--[if IE]>
<script type="text/javascript">jQuery(document).ready(function () {
jQuery(".menu-item").has("ul").children("a").attr("aria-haspopup", "true");
});</script>
<![endif]-->
<!--[if lt IE 9]>
<script src="/js/html5.js"></script>
<script src="/js/selectivizr-min.js"></script>
<![endif]-->
<!--[if IE 8]>
<link rel="stylesheet" type="text/css" media="all" href="/css/ie8.css"/>
<![endif]-->
<meta property="og:title" content="LATEST NEWS UPDATES | How Women Pay the Price for Population Control -Ruhi Kandhari" />
<meta property="og:url" content="https://im4change.in/latest-news-updates/how-women-pay-the-price-for-population-control-ruhi-kandhari-4674133.html" />
<meta property="og:type" content="article" />
<meta property="og:description" content="
-Tehelka
Despite the serious toll it takes on women's health, female sterilisation remains the most prevalent form of contraception in India.
While memories of the 21 months of Emergency in 1975-77, imposed by the then prime minister Indira Gandhi, survives even..." />
<meta property="og:image" content="" />
<meta property="fb:app_id" content="0" />
<meta name="viewport" content="width=device-width, initial-scale=1, maximum-scale=1, user-scalable=no">
<link rel="apple-touch-icon-precomposed" sizes="144x144" href="https://im4change.in/images/apple1.png">
<link rel="apple-touch-icon-precomposed" sizes="120x120" href="https://im4change.in/images/apple2.png">
<link rel="apple-touch-icon-precomposed" sizes="72x72" href="https://im4change.in/images/apple3.png">
<link rel="apple-touch-icon-precomposed" href="https://im4change.in/images/apple4.png">
<style>
.gsc-results-wrapper-overlay{
top: 38% !important;
height: 50% !important;
}
.gsc-search-button-v2{
border-color: #035588 !important;
background-color: #035588 !important;
}
.gsib_a{
height: 30px !important;
padding: 2px 8px 1px 6px !important;
}
.gsc-search-button-v2{
height: 41px !important;
}
input.gsc-input{
background: none !important;
}
@media only screen and (max-width: 600px) {
.gsc-results-wrapper-overlay{
top: 11% !important;
width: 87% !important;
left: 9% !important;
height: 43% !important;
}
.gsc-search-button-v2{
padding: 10px 10px !important;
}
.gsc-input-box{
height: 28px !important;
}
/* .gsib_a {
padding: 0px 9px 4px 9px !important;
}*/
}
@media only screen and (min-width: 1200px) and (max-width: 1920px) {
table.gsc-search-box{
width: 15% !important;
float: right !important;
margin-top: -118px !important;
}
.gsc-search-button-v2 {
padding: 6px !important;
}
}
</style>
<script>
$(function () {
$("#accordion").accordion({
event: "click hoverintent"
});
});
/*
* hoverIntent | Copyright 2011 Brian Cherne
* http://cherne.net/brian/resources/jquery.hoverIntent.html
* modified by the jQuery UI team
*/
$.event.special.hoverintent = {
setup: function () {
$(this).bind("mouseover", jQuery.event.special.hoverintent.handler);
},
teardown: function () {
$(this).unbind("mouseover", jQuery.event.special.hoverintent.handler);
},
handler: function (event) {
var currentX, currentY, timeout,
args = arguments,
target = $(event.target),
previousX = event.pageX,
previousY = event.pageY;
function track(event) {
currentX = event.pageX;
currentY = event.pageY;
}
;
function clear() {
target
.unbind("mousemove", track)
.unbind("mouseout", clear);
clearTimeout(timeout);
}
function handler() {
var prop,
orig = event;
if ((Math.abs(previousX - currentX) +
Math.abs(previousY - currentY)) < 7) {
clear();
event = $.Event("hoverintent");
for (prop in orig) {
if (!(prop in event)) {
event[prop] = orig[prop];
}
}
// Prevent accessing the original event since the new event
// is fired asynchronously and the old event is no longer
// usable (#6028)
delete event.originalEvent;
target.trigger(event);
} else {
previousX = currentX;
previousY = currentY;
timeout = setTimeout(handler, 100);
}
}
timeout = setTimeout(handler, 100);
target.bind({
mousemove: track,
mouseout: clear
});
}
};
</script>
<script type="text/javascript">
var _gaq = _gaq || [];
_gaq.push(['_setAccount', 'UA-472075-3']);
_gaq.push(['_trackPageview']);
(function () {
var ga = document.createElement('script');
ga.type = 'text/javascript';
ga.async = true;
ga.src = ('https:' == document.location.protocol ? 'https://ssl' : 'http://www') + '.google-analytics.com/ga.js';
var s = document.getElementsByTagName('script')[0];
s.parentNode.insertBefore(ga, s);
})();
</script>
<link rel="stylesheet" href="/css/custom.css?v=1.16"/> <script src="/js/jquery.ui.totop.js?1575549704"></script> <script src="/js/setting.js?1575549704"></script> <link rel="manifest" href="/manifest.json">
<meta name="theme-color" content="#616163" />
<meta name="apple-mobile-web-app-capable" content="yes">
<meta name="apple-mobile-web-app-status-bar-style" content="black">
<meta name="apple-mobile-web-app-title" content="im4change">
<link rel="apple-touch-icon" href="/icons/logo-192x192.png">
</head>
<body id="top" class="home inner blog">
<div class="background-cover"></div>
<div class="wrapper animated">
<header id="theme-header" class="header_inner" style="position: relative;">
<div class="logo inner_logo" style="left:20px !important">
<a title="Home" href="https://im4change.in/">
<img src="https://im4change.in/images/logo2.jpg?1582080632" class="logo_image" alt="im4change"/> </a>
</div>
<div class="langhindi" style="color: #000;display:none;"
href="https://im4change.in/">
<a class="more-link" href="https://im4change.in/">Home</a>
<a href="https://im4change.in/hindi/" class="langbutton ">हिन्दी</a>
</div>
<nav class="fade-in animated2" id="main-nav">
<div class="container">
<div class="main-menu">
<ul class="menu" id="menu-main">
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
style="left: -40px;"><a
target="_blank" href="https://im4change.in/">Home</a>
</li>
<li class="menu-item mega-menu menu-item-type-taxonomy mega-menu menu-item-object-category mega-menu menu-item-has-children parent-list"
style=" margin-left: -40px;"><a href="#">KNOWLEDGE GATEWAY <span class="sub-indicator"></span>
</a>
<div class="mega-menu-block background_menu" style="padding-top:25px;">
<div class="container">
<div class="mega-menu-content">
<div class="mega-menu-item">
<h3><b>Farm Crisis</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/farmers039-suicides-14.html"
class="left postionrel">Farm Suicides </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/unemployment-30.html"
class="left postionrel">Unemployment </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/rural-distress-70.html"
class="left postionrel">Rural distress </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/migration-34.html"
class="left postionrel">Migration </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/key-facts-72.html"
class="left postionrel">Key Facts </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/debt-trap-15.html"
class="left postionrel">Debt Trap </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Empowerment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/union-budget-73.html"
class="left postionrel">Union Budget And Other Economic Policies </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/forest-and-tribal-rights-61.html"
class="left postionrel">Forest and Tribal Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-education-60.html"
class="left postionrel">Right to Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-food-59.html"
class="left postionrel">Right to Food </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/displacement-3279.html"
class="left postionrel">Displacement </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-work-mg-nrega-39.html"
class="left postionrel">Right to Work (MG-NREGA) </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/gender-3280.html"
class="left postionrel">GENDER </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-information-58.html"
class="left postionrel">Right to Information </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/social-audit-48.html"
class="left postionrel">Social Audit </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Hunger / HDI</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/poverty-and-inequality-20499.html"
class="left postionrel">Poverty and inequality </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/malnutrition-41.html"
class="left postionrel">Malnutrition </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/public-health-51.html"
class="left postionrel">Public Health </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/education-50.html"
class="left postionrel">Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hunger-overview-40.html"
class="left postionrel">Hunger Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hdi-overview-45.html"
class="left postionrel">HDI Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/pds-ration-food-security-42.html"
class="left postionrel">PDS/ Ration/ Food Security </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/sdgs-113.html"
class="left postionrel">SDGs </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/mid-day-meal-scheme-mdms-53.html"
class="left postionrel">Mid Day Meal Scheme (MDMS) </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Environment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/time-bomb-ticking-52.html"
class="left postionrel">Time Bomb Ticking </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/water-and-sanitation-55.html"
class="left postionrel">Water and Sanitation </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/impact-on-agriculture-54.html"
class="left postionrel">Impact on Agriculture </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Law & Justice</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/social-justice-20500.html"
class="left postionrel">Social Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/access-to-justice-47.html"
class="left postionrel">Access to Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/human-rights-56.html"
class="left postionrel">Human Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/corruption-35.html"
class="left postionrel">Corruption </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/general-insecurity-46.html"
class="left postionrel">General Insecurity </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/disaster-relief-49.html"
class="left postionrel">Disaster & Relief </a>
</p>
</div>
</div>
</div>
</div>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page "><a target="_blank" href="https://im4change.in/nceus_reports.php">NCEUS reports</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children parent-list ">
<a target="_blank" href="https://im4change.in/about-us-9.html">About Us <span
class="sub-indicator"></span></a>
<ul class="sub-menu aboutmenu">
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/objectives-8.html">Objectives</a>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/contactus.php">Contact
Us</a></li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/about-us-9.html">About
Us</a></li>
</ul>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children ">
<a target="_blank" href="https://im4change.in/fellowships.php" title="Fellowships">Fellowships</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/media-workshops.php">Workshops</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/research.php">Research</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/links-64">Partners</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
id="menu-item-539"><a target="_blank" href="https://im4change.in/hindi/"
class="langbutton langlinkfont17">हिन्दी</a></li>
</ul>
</div> </div>
<!-- <div style="float: right;">
<script async src="https://cse.google.com/cse.js?cx=18b4f2e0f11bed3dd"></script>
<div class="gcse-search"></div>
</div> -->
<div class="search-block" style=" margin-left: 8px; margin-right: 7px;">
<form method="get" id="searchform" name="searchform"
action="https://im4change.in/search"
onsubmit="return searchvalidate();">
<button class="search-button" type="submit" value="Search"></button>
<input type="text" id="s" name="qryStr" value=""
onfocus="if (this.value == 'Search...') {this.value = '';}"
onblur="if (this.value == '') {this.value = 'Search...';}">
</form>
</div>
</nav>
</header>
<div class="container">
<div id="main-content" class=" main1 container fade-in animated3 sidebar-narrow-left">
<div class="content-wrap">
<div class="content" style="width: 900px;min-height: 500px;">
<section class="cat-box recent-box innerCatRecent">
<h1 class="cat-box-title">How Women Pay the Price for Population Control -Ruhi Kandhari</h1>
<a href="JavaScript:void(0);" onclick="return shareArticle(26095);">
<img src="https://im4change.in/images/email.png?1582080630" border="0" width="24" align="right" alt="Share this article"/> </a>
<a href="https://im4change.in/latest-news-updates/how-women-pay-the-price-for-population-control-ruhi-kandhari-4674133/print"
rel="nofollow">
<img src="https://im4change.in/images/icon-print.png?1582080630" border="0" width="24" align="right" alt="Share this article"/>
</a>
</section>
<section class="recent-box innerCatRecent">
<small class="pb-1"><span class="dateIcn">
<img src="https://im4change.in/images/published.svg?1582080666" alt="published"/>
Published on</span><span class="text-date"> Oct 7, 2014</span>
<span
class="dateIcn">
<img src="https://im4change.in/images/modified.svg?1582080666" alt="modified"/> Modified on </span><span class="text-date"> Oct 7, 2014</span>
</small>
</section>
<div class="clear"></div>
<div style="padding-top: 10px;">
<div class="innerLineHeight">
<div class="middleContent innerInput latest-news-updates">
<table>
<tr>
<td>
<div>
<div align="justify">-Tehelka</div><p align="justify"><em>Despite the serious toll it takes on women's health, female sterilisation remains the most prevalent form of contraception in India. </em></p><p align="justify">While memories of the 21 months of Emergency in 1975-77, imposed by the then prime minister Indira Gandhi, survives even today in the minds of Indian men as the fear of forced sterilisation, the country's population control policies have shifted over the years since then to target the politically less powerful and vulnerable poor women. Almost the entire burden of what is euphemistically called "family planning" is today borne by women. And it has taken a toll on the health of large sections of women in the country.</p><p align="justify"><img src="https://im4change.in/siteadmin/tinymce/uploaded/Contraception.jpg" alt="Contraception" width="660" height="508" /> </p><p align="justify">In fact, the mainstay of our population control strategy comprises two methods targeted at women - tubectomy (female sterilisation surgery) and insertion of an intrauterine device (IUD) also known as Copper-T. Neither method is known to be suitable for all women. Yet, in the rush to meet targets, these methods are widely promoted and their adverse effects on women ignored. The public health infrastructure is not geared to manage contraception, the staff is not trained in counselling women or seek their informed consent, and pain is considered an acceptable side-effect.</p><p align="justify">According to the latest National Family Health Survey, conducted in 2005-06, a third of the women in the reproductive age group have undergone surgery for sterilisation and thousands have been inserted with IUDs, with or without their consent, at some point in their lives. After months of suffering pain, many women have to visit private clinics to get the IUDs removed as the government hospitals largely refuse to do so.</p><p align="justify">The World Contraception Day was observed on 26 September. The time is apt to take a hard look at India's population control policies from the perspective of the women who are forced to suffer its consequences.</p><p align="justify">Take the case of 30-year-old Rajkumari from New Delhi, who underwent tubectomy five years ago. In five years of marriage, she had three children, followed by three abortions. A social health worker appointed by the state government had convinced her that this was the only way to avoid pregnancy. Her husband, however, was never counselled to use contraception.</p><p align="justify">Since the surgery, Rajkumari has not been able to sleep peacefully on most nights. She often suffers from recurring headaches, hot flashes, night sweats and stabbing pain in her abdomen. In the month following her surgery, she visited the government hospital several times, but the doctors only prescribed her medicines to control the symptoms. "The medicines only offered temporary relief. My life has been a curse for the past five years with constant suffering," she says.</p><p align="justify">Her neighbour, 23-year-old Pushpa, also narrates a similar tale of pain. The nurse at a public health facility inserted her with an IUD after she delivered her first child. Her consent was not sought. The procedure was done after getting the consent form signed by her husband, a daily wage labourer who had studied up to Class V. He wasn't explained what an IUD is and what the form was for.</p><p align="justify">Pushpa was dizzy when she returned home. She bled profusely, became pale over time and stayed bed-ridden. Her periods lasted up to two weeks sometimes. She lost her appetite, became weak and was unable to feed her baby on most days. When she went back to the hospital, she was prescribed antibiotics and painkillers. But she continued to bleed and suffered from pain in her abdomen. It took her three months to save enough money to get the IUD removed at a private clinic.</p><p align="justify">The common known side-effects of IUDs are nausea, changes in menstrual bleeding and severe cramps. Sterilisation, on the other hand, is a risky surgery that may lead to internal infection or bleeding, injury to internal organs and even death.</p><p align="justify">There are thousands of women like Rajkumari and Pushpa who have suffered the terrible side-effects of tubectomy and IUDs.</p><p align="justify">Stuck on a wall in the lobby of the office of New Delhi-based NGO Centre for Health and Social Justice (CHSJ) is a clipping of a June 2013 article by the Bloomberg news service headlined ‘Pushing Indian Women toward Sterilisation'. It tells the story of Sumati Devi, who underwent sterilisation on an "operating table with bloody sheets". The operation was done with a rusted scalpel and she was neither counselled nor asked for her consent.</p><p align="justify">Instead, she was given some cash as an "incentive".</p><p align="justify">The article threw light on how 10 times more women than men undergo sterilisation surgeries in filthy "sterilisation camps", even though female sterilisation involves a more complicated operation than male vasectomy.</p><p align="justify">Another clipping from February 2012 headlined ‘Pregnant woman bleeds to death after sterilisation' (The Times of India) told the story of a 35-year-old pregnant woman who bled to death in Balaghat district of Madhya Pradesh while the doctors were trying to sterilise her.</p><p align="justify">She had been pregnant with twins - both girls - for 12 weeks when the operation was conducted. She died a few hours after she began bleeding on the operation table because the doctors did not follow the basic protocol of medically screening women before the sterilisation operation.</p><p align="justify">There was also a clipping of a January 2012 story titled ‘Barrack-room surgery in Bihar's backwaters' about a sterilisation camp conducted by an NGO in a hamlet in Araria district without any operation theatre, where 61 tubectomy surgeries were carried out at a breakneck speed using expired medicines.</p><p align="justify">Another clipping on display was of a March 2012 article titled ‘Freebies lengthen sterilisation queues' (The Deccan Herald) talked of how a district administration won a Tata Nano car for meeting sterilisation targets. Giving LPG connections to every family from which a woman underwent tubectomy, the administration had got over 2,000 tubectomy surgeries carried out in just three days.</p><p align="justify">According to the most recent data collected in 2012-13 under the District Level Household and Facility Survey, state governments increasingly prefer female sterilisation as a mode of family planning even though it is one of the most risky contraception methods. In Andhra Pradesh, for example, 63 percent women in the fertile age range had been operated upon in 2012-13 as compared to 60 percent in 2007-08. During the same period, the number of men who underwent sterilisation dropped from 4 to 2 percent. Similarly, in Maharashtra, the percentage of women who underwent sterilisation increased from 52 to 54 percent, while the corresponding figure for men dropped from 3 to 1 percent. In Haryana and Punjab, one-third of the women in the reproductive age range have been sterilised.</p><p align="justify">Although tubectomies involve a serious chance of surgical infections and post-operative complications, state governments continue to promote "camps" where these are conducted on thousands of women without any proper health infrastructure and in unsanitary conditions, in a hurry to meet targets. This is despite the fact that vasectomy for men is a relatively non-invasive procedure with little risk of surgical infections and the men undergoing the procedure are usually fit enough to walk only minutes later.</p><p align="justify">"The government's focus is only on terminal methods targeted at women. Men are hardly involved in the family planning programme. They need to be involved, not as targets for non-scalpel vasectomy but as partners within a gender- equality paradigm," says Dr Abhijeet Das, director of CHSJ and an assistant professor at the Department of Global Health, University of Washington, Seattle, USA. For the past two decades, Das has been observing persuasive population control programmes, advising the government and is also part of various national and international networks, including the National Alliance on Maternal Health and Human Rights, Healthwatch Forum and MenEngage, a global alliance on men and gender equality.</p><p align="justify">The 2012-13 survey also shows indicators that define the "quality of family planning services" remain abysmally low. Most women are unaware of other means of contraception and the known side-effects of sterilisation. Even when they are counselled, the counselling is manipulative as the staff has already decided which contraceptive method a woman needs. In Maharashtra, only 17 percent of the women were told about the side-effects, while the figure was 14 percent in Punjab and 11 percent in Andhra Pradesh and Haryana. According to the District Level Household & Facility Survey 2007-08, 40 percent of the women who underwent tubectomy in public health facilities across India were illiterate, indicating that tubectomy was not the "chosen" form of contraception.</p><p align="justify">Despite the problems associated with tubectomies, state governments continue to set targets for sterilisation surgeries. The reply to an RTI query showed that around 1,000 women were targeted for tubectomy in just west Delhi over the months of January, February and March this year.</p><p align="justify">The two extremes of the debate on how to stabilise the population are represented by the coercive sterilisation drive associated with Indira Gandhi's son Sanjay Gandhi during the Emergency, on the one hand, and senior Congress politician Karan Singh's statement at the 1974 World Population Conference in Bucharest, Romania, that "development is the best contraceptive", on the other. For a long time, the dominant thinking globally was in favour of coercive policies.</p><p align="justify">Internationally, this debate came to rest at the International Conference on Population and Development 1994 (ICPD 94) in Cairo, Egypt. At ICPD 94, civil society activists from around the world shared experiences of coercive population policies and convinced 179 national governments to see "population" as people, not a number. Economists like Amartya Sen had also proved by then that improvements in women's education and healthcare automatically result in smaller families without any need for authoritative population control policies.</p><p align="justify">ICPD 94 brought about a "paradigm shift". The governments agreed to abide by reproductive rights and honour gender equality while providing universal access to family planning, sexual and reproductive health services. The Indian government, too, grudgingly committed to place individuals at the centre of development. However, the state governments in India by and large do not follow this principle in practice and it is not uncommon for politicians, bureaucrats, judges and the educated, urban middle class to blame India's large population for nearly all the problems plaguing the country and favour force over cooperation.</p><p align="justify">Until ICPD 94, population was considered a dirty word - a dangerous "bomb" that would explode if not controlled. In the early 1950s, more babies were surviving in the newly-independent countries and fewer children were being born in the richer countries, leading to a fear of "overpopulation" in the Global South. This led to the formation in 1952 of two NGOs - the Population Council and the International Planned Parenthood Federation (IPPF) - in New York and Bombay, respectively. They were set up with the purpose of influencing the US government to orient the US Agency for International Development (USAID) towards population control in the Third World, alerting Americans to the danger of population "explosion" and raising funds for international birth control programmes.</p><p align="justify">An advertisement for a joint campaign by the two NGOs read: "A world of mass starvation in underdeveloped countries will be a world of chaos, riots and war. And a perfect breeding ground for communism... Our own national interests demand that we go all out to help the underdeveloped countries control their populations."</p><p align="justify">The political agenda was reinforced and validated by Stanford University Professor Paul R Ehrlich, who authored The Population Bomb in 1968. He emphasised birth control at any cost with the use of contraceptives, mass sterilisation and pre-natal sex determination (so that parents can design the family sex composition). The US government was soon convinced. In 1974, National Security Study Memorandum 200 of the National Security Council asserted that population growth in poor countries posed a problem for the security of the US. That is how the US and other industrialised countries, which had achieved lower birth rates due to improvements in education, healthcare and incomes, without any coercive population control policies, became the biggest proponents of the latter.</p><p align="justify">India could not remain unaffected by the discourse. In 1970, JRD Tata formed the Population Foundation of India with money from the Ford Foundation for population control advocacy in India. While the country's population initially focussed on vasectomy of men and stayed clear of female sterilisation, considering the risk of infection, the tide had turned by the 1980s. The infamous coercive male sterilisation drives of the Emergency period gave way to the setting of targets for female sterilisation, which continues to dominate the population control policy.</p><p align="justify">In 1992, a study by Dr Rani Bang and Dr Abhay Bang demonstrated that women had more faith in indigenous methods of contraception than the modern ones because they commonly associated the latter with adverse effects such as backache, abdominal pain, weakness and irregular or excessive menstruation. Women also found that healthcare professionals were often insensitive to these complaints and regarded them as minor and insignificant side-effects that should be ignored.</p><p align="justify">ICPD 94 was the culmination of the coming together of academics, activists and the medical community in efforts to propose an alternative perspective on population control policies. They showed how a policy of targets, incentives and disincentives under the National Family Planning Programme had made women mute recipients suffering quietly.</p><p align="justify">Among the participants at ICPD 94 was an IAS officer, AR Nanda, who was then the secretary at the Union Ministry of Health. After he returned from Cairo, he took up the mantle to reorient the population policy. The second half of the 1990s saw a new target-free approach, which focussed on combining contraception needs with providing reproductive and child health. Nanda also drafted the landmark National Population Policy (NPP) 2000, which stressed on improvements in human development, gender equality and reproductive health to stabilise population growth.</p><p align="justify">"In 1999, when I proposed the NPP, a few MPs supported the two pillars of the policy - informed choice and informed consent - but it was largely criticised in Parliament," says Nanda, who has since retired from the government, but continues to advise the National Coalition Against Two-Child Norm, an advocacy group of NGOs, academics and activists concerned with promoting policies that empower people to exercise their reproductive rights and choice.</p><p align="justify">The NPP 2000 begins with a statement that "the overriding objective of economic and social development is to improve (the) quality of life that people lead, to enhance their well-being and to provide them with opportunities and choices to become productive assets in society". The policy recommended the empowerment of women through enhanced access to education, employment opportunities and quality healthcare.</p><p align="justify">The policy, however, failed to influence a large section of politicians who continued to see population as a problem. In May 2000, when India's population crossed the one-billion mark, the then prime minister Atal Bihari Vajpayee said: "This is a serious matter that is both cause for concern and introspection - concern over the impact that a runaway population growth is bound to have on the nation's economic, natural and other resources; introspection over where we went wrong and how we can stabilise our population... If the present growth rate of our population remains unchecked, India will become the world's most populous country by the middle of this century, with people clamouring for a share of shrinking natural resources."</p><p align="justify">Opposition to NPP 2000 continued even after it was adopted. Population being a subject on the Concurrent List, the state governments are not obliged to follow anything that the Centre prescribes on population control. They have their own policies that in most cases go against NPP 2000. For instance, Uttar Pradesh introduced contraceptives such as injectables and implants, which are proven to be unsafe for women; Rajasthan promoted a lottery scheme for those who opt for sterilisation; and Bihar contracted out tubectomy surgeries to private operators and NGOs.</p><p align="justify">"The language used in talking about population stabilisation changed after ICPD 94 but the mindset remained more or less the same," says Nanda. "Even at the national level, male responsibility and gender equity were largely ignored. The state governments favour setting of targets and promoting terminal methods because the results are easy to measure."</p><p align="justify">Clearly, despite all the talk of empowering women, their reproductive autonomy - the right to choose whether to have children or not and the freedom to choose the methods of fertility management based on access to proper information - has been largely ignored in the policies and practices promoted by various governments in India.</p><p align="justify">Unfortunately, India has seen a reduced prevalence of condom use with women remaining unequal targets of the family planning burden. As the dominant, irreversible methods of population control take a toll on women's health, there is indeed a need for reorienting it towards the promotion of temporary and reversible methods such as condoms, which also provide a barrier against sexually transmitted diseases.</p><p align="justify">--</p><p align="justify">The downside of contraception</p><p align="justify">Disadvantages and side-effects of various contraceptive methods</p><p align="justify">Oral Contraceptive Pill: Nausea, mild headaches, tender breasts, spotting between periods, irregular bleeding, moodiness, vomiting within two hours of taking a pill, severe diarrhoea and vomiting for more than 24 hours</p><p align="justify">Copper-bearing IUDs: Menstrual changes in early months, longer and heavy menstrual periods, bleeding or spotting between periods, more cramps or pain during period. Uncommon sideeffects include severe cramps and pain beyond first three-five days of insertion, heavy menstrual bleeding or bleeding between periods, possibly contributing to anaemia and possibility of perforation if not inserted properly. It does not protect against sexually transmitted diseases (STDs) including HIV/AIDs. Medical procedure, including pelvic examination, is needed to insert the IUD. Occasionally, a woman faints during the insertion procedure. A trained healthcare provider must remove the IUD. The IUD may come out of the uterus possibly without the woman knowing about it (more common when the IUD is inserted soon after childbirth)</p><p align="justify">Vasectomy: Uncomfortable for two or three days, pain in scrotum, swelling and bruising and brief feeling of faintness after the procedure. Rare complications of surgery include bleeding or infection at the incision site or inside the incision, blood clots in the scrotum. No protection against STDs, including HIV/AIDs</p><p align="justify">Tubectomy: Uncommon complications include infection or bleeding at the incision, internal infection or bleeding, injury to internal organs and anaesthesia risk. No protection against STDs</p><p align="justify">Male Condom: Latex condoms may cause itching for a few people who are allergic to latex. Also, some people may be allergic to the lubricant on some brands of condoms. Small possibility that condom might slip off or break during sexual intercourse</p><p align="justify">(Source: Government reference manual)</p>
</div>
</td>
</tr>
</table>
</div>
</div>
</div>
<div class="clear"></div>
<br><a href="http://www.tehelka.com/how-women-pay-the-price-for-population-control-iod-birth-control-health-female-sterilisation/" class="re" target="_blank">Tehelka Magazine, Volume 11, Issue 41, 11 October 2014, http://www.tehelka.com/how-women-pay-the-price-for-population-control-iod-birth-control-health-female-sterilisation/</a><div class="clear"></div>
<div style="padding-top: 18px;">
<p class="post-tag">Tagged with:
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=gender discrimination"
title="gender discrimination">
gender discrimination </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Gender Equality"
title="Gender Equality">
Gender Equality </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Reproductive Health"
title="Reproductive Health">
Reproductive Health </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Contraception"
title="Contraception">
Contraception </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Population Control"
title="Population Control">
Population Control </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Health"
title="Health">
Health </a>
</p>
</div>
<div class="clear"></div>
<br><br>
<div class="widget-top">
<h4>Related Articles</h4>
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<ul id="recentcomments">
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/fifth-report-from-gambia-implicates-indian-drug-maker-for-contaminated-syrups-banjot-kaur.html"
title="Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur">
Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-may-have-seen-steepest-dip-in-multidimensional-poverty-among-110-nations-as-per-undp-data-nikhil-rampal.html"
title="India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal">
India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/health-among-top-three-priorities-for-indian-voters-after-jobs-and-education-survey-shows-oliver-heath-jyoti-mishra-louise-tillin-sandhya-venkateswaran.html"
title="Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran">
Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/prevalence-of-zero-food-among-infants-and-young-children-in-india-patterns-of-change-across-the-states-and-union-territories-of-india-1993-2021-the-lancet.html"
title="Prevalence of Zero-Food among infants and young children in India - The Lancet ">
Prevalence of Zero-Food among infants and young children in India - The Lancet </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-s-sustainability-goals-at-risk-because-of-extreme-heatwaves-carbon-copy.html"
title="India's Sustainability Goals at Risk Because of Extreme Heatwaves - Carbon Copy">
India's Sustainability Goals at Risk Because of Extreme Heatwaves - Carbon Copy </a>
</li>
</ul>
</div>
<div class="comment-respond" id="respond">
<a name="commentbox"> </a>
<h3 class="comment-reply-title" id="reply-title">Write Comments</h3>
<form method="post" accept-charset="utf-8" role="form" action="/latest-news-updates/how-women-pay-the-price-for-population-control-ruhi-kandhari-4674133.html"><div style="display:none;"><input type="hidden" name="_method" value="POST"/></div> <form class="comment-form" id="commentform" method="post" action="#commentbox" onSubmit="return validate()"
name="cmtform">
<input type="hidden" name="cmttype" value="articlecmt"/>
<input type="hidden" name="article_id" value="26095"/>
<p class="comment-notes">Your email address will not be published. Required fields are marked <span
class="required">*</span></p>
<p class="comment-form-author">
<label for="commenterName">Name</label>
<span class="required">*</span>
<input type="text" aria-required="true" size="30"
value=""
name="commenterName" id="commenterName" required="true">
</p>
<p class="comment-form-email">
<label for="commenterEmail">Email</label> <span class="required">*</span>
<input aria-required="true" size="30" name="commenterEmail" id="commenterEmail" type="email"
value=""
required="true">
</p>
<p class="comment-form-contact">
<label for="commenterPh">Contact No.</label>
<input type="text" size="30"
value=""
name="commenterPh" id="commenterPh">
</p>
<p class="comment-form-comment">
<label for="comment">Comment</label>
<textarea aria-required="true" required="true" rows="8" cols="45" name="comment"
id="comment"></textarea>
</p>
<p class="comment-form-comment">
<label for="comment">Type the characters you see in the image below <span class="required">*</span><br><img
class="captchaImg"
src="https://im4change.in/securimage_show_art.php?tk=1115961128" alt="captcha"/>
</label>
</p>
<input type="text" name="vrcode" required="true"/>
<p class="form-submit" style="width: 200px;">
<input type="submit" value="Post Comment" id="submit" name="submit">
</p></form>
</div>
<style>
.ui-widget-content {
height: auto !important;
}
</style>
<div id="share-modal"></div>
<style>
.middleContent a{
background-color: rgba(108,172,228,.2);
}
.middleContent a:hover{
background-color: #418fde;
border-color: #418fde;
color: #000;
}
</style>
<script>
function shareArticle(article_id) {
var options = {
modal: true,
height: 'auto',
width: 600 + 'px'
};
$('#share-modal').html("");
$('#share-modal').load('https://im4change.in/share_article?article_id=' + article_id).dialog(options).dialog('open');
}
function postShare() {
var param = 'article_id=' + $("#article_id").val();
param = param + '&y_name=' + $("#y_name").val();
param = param + '&y_email=' + $("#y_email").val();
param = param + '&f_name=' + $("#f_name").val();
param = param + '&f_email=' + $("#f_email").val();
param = param + '&y_msg=' + $("#y_msg").val();
$.ajax({
type: "POST",
url: 'https://im4change.in/post_share_article',
data: param,
success: function (response) {
$('#share-modal').html("Thank You, Your message posted to ");
}
});
return false;
}
</script> </div>
</div>
<!-- Right Side Section Start -->
<!-- MAP Section START -->
<aside class="sidebar indexMarg">
<div class="ad-cell">
<a href="https://im4change.in/statemap.php" title="">
<img src="https://im4change.in/images/map_new_version.png?1582080666" alt="India State Map" class="indiamap" width="232" height="252"/> </a>
<div class="rightmapbox">
<div id="sideOne" class="docltitle"><a href="https://im4change.in/state-report/india/36" target="_blank">DOCUMENTS/
REPORTS</a></div>
<div id="sideTwo" class="statetitle"><a href="https://im4change.in/states.php"target="_blank">STATE DATA/
HDRs.</a></div>
</div>
<div class="widget widgePadTop"></div>
</div>
</aside>
<!-- MAP Section END -->
<aside class="sidebar sidePadbottom">
<div class="rightsmlbox1" >
<a href="https://im4change.in/knowledge_gateway" target="_blank" style="color: #035588;
font-size: 17px;">
KNOWLEDGE GATEWAY
</a>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/newsletter" target="_blank">
NEWSLETTER
</a>
</p>
</div>
</div>
<div class="rightsmlbox1" style="height: 325px;">
<div>
<p class="rightsmlbox1_title">
Interview with Prof. Ravi Srivastava
</p>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/video/interview-with-prof-ravi-srivastava-on-current-economic-crisis">
<img width="250" height="200" src="/images/interview_video_home.jpg" alt="Interview with Prof. Ravi Srivastava"/>
</a>
<!--
<iframe width="250" height="200" src="https://www.youtube.com/embed/MmaTlntk-wc" frameborder="0" allow="accelerometer; autoplay; encrypted-media; gyroscope; picture-in-picture" allowfullscreen=""></iframe>-->
</p>
<a href="https://im4change.in/videogallery" class="more-link CatArchalAnch1" target="_blank">
More videos
</a>
</div>
</div>
<div class="rightsmlbox1">
<div>
<!--div id="sstory" class="rightboxicons"></div--->
<p class="rightsmlbox1_title"><a href="https://im4change.in/list-success-stories" target="_blank">Success Stories</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/interviews" target="_blank">Interviews</a>
</p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a href="https://www.commoncause.in/page.php?id=10" >Donate</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/marquee"
class="isf_link more-link" title="India Focus?" style="border: 4px solid #fdd922;width: 90%;background-color: #fdd922;text-align: center;color: #000000;font-size:18px" target="_blank">India Focus</a></p> </div>
</div>
<div class="rightsmlbox1" style="height: 104px !important;">
<a href="https://im4change.in/quarterly_reports.php" target="_blank">
Quarterly Reports on Effect of Economic Slowdown on Employment in India (2008 - 2015)
</a>
</div>
<!-- <div class="rightsmlbox1">
<a href="https://play.google.com/store/apps/details?id=com.im4.im4change" target="_blank">
</a></div> -->
<!-- <section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">Most Visited</h2>
</section> -->
<!-- accordion Starts here -->
<!-- <div id="accordion" class="accordMarg">
</div> -->
<!-- accordion ends here -->
<!-- Widget Tag Cloud Starts here -->
<div id="tag_cloud-2" class="widget widget_tag_cloud">
<section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">MOST VISITED TAGS</h2>
</section>
<div class="widget-top wiPdTp">
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<div class="tagcloud">
<a href="https://im4change.in/search?qryStr=Agriculture"
target="_blank" class="tag-link-4 font4">Agriculture</a>
<a href="https://im4change.in/search?qryStr=Food Security"
target="_blank" class="tag-link-4 font4">Food Security</a>
<a href="https://im4change.in/search?qryStr=Law and Justice"
target="_blank" class="tag-link-4 font4">Law and Justice</a>
<a href="https://im4change.in/search?qryStr=Health"
target="_blank" class="tag-link-4 font4">Health</a>
<a href="https://im4change.in/search?qryStr=Right to Food"
target="_blank" class="tag-link-4 font4">Right to Food</a>
<a href="https://im4change.in/search?qryStr=Corruption"
target="_blank" class="tag-link-4 font4">Corruption</a>
<a href="https://im4change.in/search?qryStr=farming"
target="_blank" class="tag-link-4 font4">farming</a>
<a href="https://im4change.in/search?qryStr=Environment"
target="_blank" class="tag-link-4 font4">Environment</a>
<a href="https://im4change.in/search?qryStr=Right to Information"
target="_blank" class="tag-link-4 font4">Right to Information</a>
<a href="https://im4change.in/search?qryStr=NREGS"
target="_blank" class="tag-link-4 font4">NREGS</a>
<a href="https://im4change.in/search?qryStr=Human Rights"
target="_blank" class="tag-link-4 font4">Human Rights</a>
<a href="https://im4change.in/search?qryStr=Governance"
target="_blank" class="tag-link-4 font4">Governance</a>
<a href="https://im4change.in/search?qryStr=PDS"
target="_blank" class="tag-link-4 font4">PDS</a>
<a href="https://im4change.in/search?qryStr=COVID-19"
target="_blank" class="tag-link-4 font4">COVID-19</a>
<a href="https://im4change.in/search?qryStr=Land Acquisition"
target="_blank" class="tag-link-4 font4">Land Acquisition</a>
<a href="https://im4change.in/search?qryStr=mgnrega"
target="_blank" class="tag-link-4 font4">mgnrega</a>
<a href="https://im4change.in/search?qryStr=Farmers"
target="_blank" class="tag-link-4 font4">Farmers</a>
<a href="https://im4change.in/search?qryStr=transparency"
target="_blank" class="tag-link-4 font4">transparency</a>
<a href="https://im4change.in/search?qryStr=Gender"
target="_blank" class="tag-link-4 font4">Gender</a>
<a href="https://im4change.in/search?qryStr=Poverty"
target="_blank" class="tag-link-4 font4">Poverty</a>
<a href="https://im4change.in/search?qryStr=Farm Laws" target="_blank" class="tag-link-4 font4">Farm Laws
</a>
<a href="https://im4change.in/search?qryStr=Citizenship Amendment Act" target="_blank" class="tag-link-4 font4">Citizenship Amendment Act
</a>
<a href="https://im4change.in/search?qryStr=CAA NPR NRIC" target="_blank" class="tag-link-4 font4">CAA NPR NRIC
</a>
<a href="https://im4change.in/search?qryStr=Job Losses" target="_blank" class="tag-link-4 font4">Job Losses
</a>
<a href="https://im4change.in/search?qryStr=Migrant Workers" target="_blank" class="tag-link-4 font4">Migrant Workers
</a>
<a href="https://im4change.in/search?qryStr=Unemployment" target="_blank" class="tag-link-4 font4">Unemployment
</a>
<a href="https://im4change.in/search?qryStr=PMGKAY" target="_blank" class="tag-link-4 font4">PMGKAY
</a>
<a href="https://im4change.in/search?qryStr=PM-KISAN" target="_blank" class="tag-link-4 font4">PM-KISAN
</a>
<a href="https://im4change.in/search?qryStr=PM-CARES" target="_blank" class="tag-link-4 font4">PM-CARES
</a>
<a href="https://im4change.in/search?qryStr=LFPR" target="_blank" class="tag-link-4 font4">LFPR
</a>
</div>
</div>
</div>
<!-- Widget Tag Cloud Ends here -->
</aside>
<!-- Right Side Section End -->
</div>
<section class="cat-box cats-review-box footerSec">
<h2 class="cat-box-title vSec CatArcha">Video
Archives</h2>
<h2 class="cat-box-title CatArchaTitle">Archives</h2>
<div class="cat-box-content">
<div class="reviews-cat">
<div class="CatArchaDiv1">
<div class="CatArchaDiv2">
<ul>
<li>
<a href="https://im4change.in/news-alerts-57/moving-upstream-luni-fellowship.html" target="_blank">
Moving Upstream: Luni – Fellowship </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/135-million-indians-exited-multidimensional-poverty-as-per-government-figures-is-that-the-same-as-poverty-reduction.html" target="_blank">
135 Million Indians Exited “Multidimensional" Poverty as per Government... </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/explainer-why-are-tomato-prices-on-fire.html" target="_blank">
Explainer: Why are Tomato Prices on Fire? </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/nsso-survey-only-39-1-of-all-households-have-drinking-water-within-dwelling-46-7-of-rural-households-use-firewood-for-cooking.html" target="_blank">
NSSO Survey: Only 39.1% of all Households have Drinking... </a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/news-alerts-57"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/I51LYnP8BOk/1.jpg"
alt=" Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Short-Video-on-im4change-Hindi-website-Inclusive-Media-for-Change" target="_blank">
Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/kNqha-SwfIY/1.jpg"
alt=" "Session 1: Scope of IDEA and AgriStack" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-1- Scope-of-IDEA-and-AgriStack-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 1: Scope of IDEA and AgriStack" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/6kIVjlgZItk/1.jpg"
alt=" "Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-2-Farmer-Centric-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/2BeHTu0y7xc/1.jpg"
alt=" "Session 3: Future of Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-3-Future-of-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 3: Future of Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="divWidth">
<ul class="divWidthMarg">
<li>
<a href="https://im4change.in/video/Public-Spending-on-Agriculture-in-India-Source-Foundation-for-Agrarian-Studies"
title="Public Spending on Agriculture in India (Source: Foundation for Agrarian Studies)" target="_blank">
Public Spending on Agriculture in India (Source: Foundation for...</a>
</li>
<li>
<a href="https://im4change.in/video/Agrarian-Change-Seminar-Protests-against-the-New-Farm-Laws-in-India-by-Prof-Vikas-Rawal-JNU-Source-Journal-Of-Agrarian-Change"
title="Agrarian Change Seminar: 'Protests against the New Farm Laws in India' by Prof. Vikas Rawal, JNU (Source: Journal Of Agrarian Change) " target="_blank">
Agrarian Change Seminar: 'Protests against the New Farm Laws...</a>
</li>
<li>
<a href="https://im4change.in/video/Webinar-Ramrao-The-Story-of-India-Farm-Crisis-Source-Azim-Premji-University"
title="Webinar: Ramrao - The Story of India's Farm Crisis (Source: Azim Premji University)" target="_blank">
Webinar: Ramrao - The Story of India's Farm Crisis...</a>
</li>
<li>
<a href="https://im4change.in/video/water-and-agricultural-transformation-in-India"
title="Water and Agricultural Transformation in India: A Symbiotic Relationship (Source: IGIDR)" target="_blank">
Water and Agricultural Transformation in India: A Symbiotic Relationship...</a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/videogallery"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
</div>
</div>
</div>
</section> </div>
<div class="clear"></div>
<!-- Footer option Starts here -->
<div class="footer-bottom fade-in animated4">
<div class="container">
<div class="social-icons icon_flat">
<p class="SocialMargTop"> Website Developed by <a target="_blank" title="Web Development"
class="wot right"
href="http://www.ravinderkhurana.com/" rel="nofollow">
RAVINDErkHURANA.com</a></p>
</div>
<div class="alignleft">
<a
target="_blank" href="https://im4change.in/objectives-8.html"
class="link"
title="Objectives">Objectives</a> | <a
target="_blank" href="https://im4change.in/about-us-9.html"
class="link" title="About Us">About Us</a> | <a
target="_blank" href="https://im4change.in/media-workshops.php"
class="ucwords">Workshops</a> | <a
target="_blank" href="https://im4change.in/disclaimer/disclaimer-149.html"
title="Disclaimer">Disclaimer</a> </div>
</div>
</div>
<!-- Footer option ends here -->
</div>
<div id="connect">
<a target="_blank"
href="http://www.facebook.com/sharer.php?u=https://im4change.in/latest-news-updates/how-women-pay-the-price-for-population-control-ruhi-kandhari-4674133.html"
title="Share on Facebook">
<img src="https://im4change.in/images/Facebook.png?1582080640" alt="share on Facebook" class="ImgBorder"/>
</a><br/>
<a target="_blank"
href="http://twitter.com/share?text=Im4change&url=https://im4change.in/latest-news-updates/how-women-pay-the-price-for-population-control-ruhi-kandhari-4674133.html"
title="Share on Twitter">
<img src="https://im4change.in/images/twitter.png?1582080632" alt="Twitter" class="ImgBorder"/> </a>
<br/>
<a href="/feeds" title="RSS Feed" target="_blank">
<img src="https://im4change.in/images/rss.png?1582080632" alt="RSS" class="ImgBorder"/>
</a>
<br/>
<a class="feedback-link" id="feedbackFormLink" href="#">
<img src="https://im4change.in/images/feedback.png?1582080630" alt="Feedback" class="ImgBorder"/>
</a> <br/>
<a href="javascript:function iprl5(){var d=document,z=d.createElement('scr'+'ipt'),b=d.body,l=d.location;try{if(!b)throw(0);d.title='(Saving...) '+d.title;z.setAttribute('src',l.protocol+'//www.instapaper.com/j/WKrH3R7ORD5p?u='+encodeURIComponent(l.href)+'&t='+(new Date().getTime()));b.appendChild(z);}catch(e){alert('Please wait until the page has loaded.');}}iprl5();void(0)"
class="bookmarklet" onclick="return explain_bookmarklet();">
<img src="https://im4change.in/images/read-it-later.png?1582080632" alt="Read Later" class="ImgBorder"/> </a>
</div>
<!-- Feedback form Starts here -->
<div id="feedbackForm" class="overlay_form" class="ImgBorder">
<h2>Contact Form</h2>
<div id="contactform1">
<div id="formleft">
<form id="submitform" action="/contactus.php" method="post">
<input type="hidden" name="submitform" value="submitform"/>
<input type="hidden" name="salt_key" value="a0e0f2c6a0644a70e57ad2c96829709a"/>
<input type="hidden" name="ref" value="feedback"/>
<fieldset>
<label>Name :</label>
<input type="text" name="name" class="tbox" required/>
</fieldset>
<fieldset>
<label>Email :</label>
<input type="text" name="email" class="tbox" required/>
</fieldset>
<fieldset>
<label>Message :</label>
<textarea rows="5" cols="20" name="message" required></textarea>
</fieldset>
<fieldset>
Please enter security code
<div class="clear"></div>
<input type="text" name="vrcode" class="tbox"/>
</fieldset>
<fieldset>
<input type="submit" class="button" value="Submit"/>
<a href="#" id="closefeedbakcformLink">Close</a>
</fieldset>
</form>
</div>
<div class="clearfix"></div>
</div>
</div>
<div id="donate_popup" class="modal" style="max-width: 800px;">
<table width="100%" border="1">
<tr>
<td colspan="2" align="center">
<b>Support im4change</b>
</td>
</tr>
<tr>
<td width="25%" valign="middle">
<img src="https://im4change.in/images/logo2.jpg?1582080632" alt="" width="100%"/> </td>
<td style="padding-left:10px;padding-top:10px;">
<form action="https://im4change.in/donate" method="get">
<table width="100%" cellpadding="2" cellspacing="2">
<tr>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
10
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
100
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
1000
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
50
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
500
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
<input type="text" name="price" placeholder="?" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td colspan="3" align="right">
<input type="button" name="Pay" value="Pay"
style="width: 200px;background-color: rgb(205, 35, 36);color: #ffffff;"/>
</td>
</tr>
</table>
</form>
</td>
</tr>
</table>
</div><script type='text/javascript'>
/* <![CDATA[ */
var tievar = {'go_to': 'Go to...'};
/* ]]> */
</script>
<script src="/js/tie-scripts.js?1575549704"></script><script src="/js/bootstrap.js?1575549704"></script><script src="/js/jquery.modal.min.js?1578284310"></script><script>
$(document).ready(function() {
// tell the autocomplete function to get its data from our php script
$('#s').autocomplete({
source: "/autocomplete"
});
});
</script>
<script src="/vj-main-sw-register.js" async></script>
<script>function init(){var imgDefer=document.getElementsByTagName('img');for(var i=0;i<imgDefer.length;i++){if(imgDefer[i].getAttribute('data-src')){imgDefer[i].setAttribute('src',imgDefer[i].getAttribute('data-src'))}}}
window.onload=init;</script>
</body>
</html>'
}
$reasonPhrase = 'OK'
header - [internal], line ??
Cake\Http\ResponseEmitter::emitStatusLine() - CORE/src/Http/ResponseEmitter.php, line 148
Cake\Http\ResponseEmitter::emit() - CORE/src/Http/ResponseEmitter.php, line 54
Cake\Http\Server::emit() - CORE/src/Http/Server.php, line 141
[main] - ROOT/webroot/index.php, line 39
Warning (2): Cannot modify header information - headers already sent by (output started at /home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php:853) [CORE/src/Http/ResponseEmitter.php, line 181]
$response = object(Cake\Http\Response) {
'status' => (int) 200,
'contentType' => 'text/html',
'headers' => [
'Content-Type' => [
[maximum depth reached]
]
],
'file' => null,
'fileRange' => [],
'cookies' => object(Cake\Http\Cookie\CookieCollection) {},
'cacheDirectives' => [],
'body' => '<!DOCTYPE html>
<!--[if lt IE 7 ]>
<html class="ie ie6" lang='en'> <![endif]-->
<!--[if IE 7 ]>
<html class="ie ie7" lang='en'> <![endif]-->
<!--[if IE 8 ]>
<html class="ie ie8" lang='en'> <![endif]-->
<!--[if (gte IE 9)|!(IE)]><!-->
<html lang='en'>
<!--<![endif]-->
<head><meta http-equiv="Content-Type" content="text/html; charset=utf-8">
<title>
LATEST NEWS UPDATES | How Women Pay the Price for Population Control -Ruhi Kandhari </title>
<meta name="description" content="
-Tehelka
Despite the serious toll it takes on women's health, female sterilisation remains the most prevalent form of contraception in India.
While memories of the 21 months of Emergency in 1975-77, imposed by the then prime minister Indira Gandhi, survives even..."/>
<meta name="keywords" content="gender discrimination,Gender Equality,Reproductive Health,Contraception,Population Control,Health"/>
<meta name="news_keywords" content="gender discrimination,Gender Equality,Reproductive Health,Contraception,Population Control,Health">
<link rel="alternate" type="application/rss+xml" title="ROR" href="/ror.xml"/>
<link rel="alternate" type="application/rss+xml" title="RSS 2.0" href="/feeds/"/>
<link rel="stylesheet" href="/css/bootstrap.min.css?1697864993"/> <link rel="stylesheet" href="/css/style.css?v=1.1.2"/> <link rel="stylesheet" href="/css/style-inner.css?1577045210"/> <link rel="stylesheet" id="Oswald-css"
href="https://fonts.googleapis.com/css?family=Oswald%3Aregular%2C700&ver=3.8.1" type="text/css"
media="all">
<link rel="stylesheet" href="/css/jquery.modal.min.css?1578285302"/> <script src="/js/jquery-1.10.2.js?1575549704"></script> <script src="/js/jquery-migrate.min.js?1575549704"></script> <link rel="shortcut icon" href="/favicon.ico" title="Favicon">
<link rel="stylesheet" href="/css/jquery-ui.css?1580720609"/> <script src="/js/jquery-ui.js?1575549704"></script> <link rel="preload" as="style" href="https://www.im4change.org/css/custom.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery.modal.min.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery-ui.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/li-scroller.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<!-- <link rel="preload" as="style" href="https://www.im4change.org/css/style.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous"> -->
<link rel="preload" as="style" href="https://www.im4change.org/css/style-inner.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel='dns-prefetch' href="//im4change.org/css/custom.css" crossorigin >
<link rel="preload" as="script" href="https://www.im4change.org/js/bootstrap.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.li-scroller.1.0.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.modal.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.ui.totop.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-1.10.2.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-migrate.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-ui.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/setting.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/tie-scripts.js">
<!--[if IE]>
<script type="text/javascript">jQuery(document).ready(function () {
jQuery(".menu-item").has("ul").children("a").attr("aria-haspopup", "true");
});</script>
<![endif]-->
<!--[if lt IE 9]>
<script src="/js/html5.js"></script>
<script src="/js/selectivizr-min.js"></script>
<![endif]-->
<!--[if IE 8]>
<link rel="stylesheet" type="text/css" media="all" href="/css/ie8.css"/>
<![endif]-->
<meta property="og:title" content="LATEST NEWS UPDATES | How Women Pay the Price for Population Control -Ruhi Kandhari" />
<meta property="og:url" content="https://im4change.in/latest-news-updates/how-women-pay-the-price-for-population-control-ruhi-kandhari-4674133.html" />
<meta property="og:type" content="article" />
<meta property="og:description" content="
-Tehelka
Despite the serious toll it takes on women's health, female sterilisation remains the most prevalent form of contraception in India.
While memories of the 21 months of Emergency in 1975-77, imposed by the then prime minister Indira Gandhi, survives even..." />
<meta property="og:image" content="" />
<meta property="fb:app_id" content="0" />
<meta name="viewport" content="width=device-width, initial-scale=1, maximum-scale=1, user-scalable=no">
<link rel="apple-touch-icon-precomposed" sizes="144x144" href="https://im4change.in/images/apple1.png">
<link rel="apple-touch-icon-precomposed" sizes="120x120" href="https://im4change.in/images/apple2.png">
<link rel="apple-touch-icon-precomposed" sizes="72x72" href="https://im4change.in/images/apple3.png">
<link rel="apple-touch-icon-precomposed" href="https://im4change.in/images/apple4.png">
<style>
.gsc-results-wrapper-overlay{
top: 38% !important;
height: 50% !important;
}
.gsc-search-button-v2{
border-color: #035588 !important;
background-color: #035588 !important;
}
.gsib_a{
height: 30px !important;
padding: 2px 8px 1px 6px !important;
}
.gsc-search-button-v2{
height: 41px !important;
}
input.gsc-input{
background: none !important;
}
@media only screen and (max-width: 600px) {
.gsc-results-wrapper-overlay{
top: 11% !important;
width: 87% !important;
left: 9% !important;
height: 43% !important;
}
.gsc-search-button-v2{
padding: 10px 10px !important;
}
.gsc-input-box{
height: 28px !important;
}
/* .gsib_a {
padding: 0px 9px 4px 9px !important;
}*/
}
@media only screen and (min-width: 1200px) and (max-width: 1920px) {
table.gsc-search-box{
width: 15% !important;
float: right !important;
margin-top: -118px !important;
}
.gsc-search-button-v2 {
padding: 6px !important;
}
}
</style>
<script>
$(function () {
$("#accordion").accordion({
event: "click hoverintent"
});
});
/*
* hoverIntent | Copyright 2011 Brian Cherne
* http://cherne.net/brian/resources/jquery.hoverIntent.html
* modified by the jQuery UI team
*/
$.event.special.hoverintent = {
setup: function () {
$(this).bind("mouseover", jQuery.event.special.hoverintent.handler);
},
teardown: function () {
$(this).unbind("mouseover", jQuery.event.special.hoverintent.handler);
},
handler: function (event) {
var currentX, currentY, timeout,
args = arguments,
target = $(event.target),
previousX = event.pageX,
previousY = event.pageY;
function track(event) {
currentX = event.pageX;
currentY = event.pageY;
}
;
function clear() {
target
.unbind("mousemove", track)
.unbind("mouseout", clear);
clearTimeout(timeout);
}
function handler() {
var prop,
orig = event;
if ((Math.abs(previousX - currentX) +
Math.abs(previousY - currentY)) < 7) {
clear();
event = $.Event("hoverintent");
for (prop in orig) {
if (!(prop in event)) {
event[prop] = orig[prop];
}
}
// Prevent accessing the original event since the new event
// is fired asynchronously and the old event is no longer
// usable (#6028)
delete event.originalEvent;
target.trigger(event);
} else {
previousX = currentX;
previousY = currentY;
timeout = setTimeout(handler, 100);
}
}
timeout = setTimeout(handler, 100);
target.bind({
mousemove: track,
mouseout: clear
});
}
};
</script>
<script type="text/javascript">
var _gaq = _gaq || [];
_gaq.push(['_setAccount', 'UA-472075-3']);
_gaq.push(['_trackPageview']);
(function () {
var ga = document.createElement('script');
ga.type = 'text/javascript';
ga.async = true;
ga.src = ('https:' == document.location.protocol ? 'https://ssl' : 'http://www') + '.google-analytics.com/ga.js';
var s = document.getElementsByTagName('script')[0];
s.parentNode.insertBefore(ga, s);
})();
</script>
<link rel="stylesheet" href="/css/custom.css?v=1.16"/> <script src="/js/jquery.ui.totop.js?1575549704"></script> <script src="/js/setting.js?1575549704"></script> <link rel="manifest" href="/manifest.json">
<meta name="theme-color" content="#616163" />
<meta name="apple-mobile-web-app-capable" content="yes">
<meta name="apple-mobile-web-app-status-bar-style" content="black">
<meta name="apple-mobile-web-app-title" content="im4change">
<link rel="apple-touch-icon" href="/icons/logo-192x192.png">
</head>
<body id="top" class="home inner blog">
<div class="background-cover"></div>
<div class="wrapper animated">
<header id="theme-header" class="header_inner" style="position: relative;">
<div class="logo inner_logo" style="left:20px !important">
<a title="Home" href="https://im4change.in/">
<img src="https://im4change.in/images/logo2.jpg?1582080632" class="logo_image" alt="im4change"/> </a>
</div>
<div class="langhindi" style="color: #000;display:none;"
href="https://im4change.in/">
<a class="more-link" href="https://im4change.in/">Home</a>
<a href="https://im4change.in/hindi/" class="langbutton ">हिन्दी</a>
</div>
<nav class="fade-in animated2" id="main-nav">
<div class="container">
<div class="main-menu">
<ul class="menu" id="menu-main">
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
style="left: -40px;"><a
target="_blank" href="https://im4change.in/">Home</a>
</li>
<li class="menu-item mega-menu menu-item-type-taxonomy mega-menu menu-item-object-category mega-menu menu-item-has-children parent-list"
style=" margin-left: -40px;"><a href="#">KNOWLEDGE GATEWAY <span class="sub-indicator"></span>
</a>
<div class="mega-menu-block background_menu" style="padding-top:25px;">
<div class="container">
<div class="mega-menu-content">
<div class="mega-menu-item">
<h3><b>Farm Crisis</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/farmers039-suicides-14.html"
class="left postionrel">Farm Suicides </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/unemployment-30.html"
class="left postionrel">Unemployment </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/rural-distress-70.html"
class="left postionrel">Rural distress </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/migration-34.html"
class="left postionrel">Migration </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/key-facts-72.html"
class="left postionrel">Key Facts </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/debt-trap-15.html"
class="left postionrel">Debt Trap </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Empowerment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/union-budget-73.html"
class="left postionrel">Union Budget And Other Economic Policies </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/forest-and-tribal-rights-61.html"
class="left postionrel">Forest and Tribal Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-education-60.html"
class="left postionrel">Right to Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-food-59.html"
class="left postionrel">Right to Food </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/displacement-3279.html"
class="left postionrel">Displacement </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-work-mg-nrega-39.html"
class="left postionrel">Right to Work (MG-NREGA) </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/gender-3280.html"
class="left postionrel">GENDER </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-information-58.html"
class="left postionrel">Right to Information </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/social-audit-48.html"
class="left postionrel">Social Audit </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Hunger / HDI</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/poverty-and-inequality-20499.html"
class="left postionrel">Poverty and inequality </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/malnutrition-41.html"
class="left postionrel">Malnutrition </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/public-health-51.html"
class="left postionrel">Public Health </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/education-50.html"
class="left postionrel">Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hunger-overview-40.html"
class="left postionrel">Hunger Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hdi-overview-45.html"
class="left postionrel">HDI Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/pds-ration-food-security-42.html"
class="left postionrel">PDS/ Ration/ Food Security </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/sdgs-113.html"
class="left postionrel">SDGs </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/mid-day-meal-scheme-mdms-53.html"
class="left postionrel">Mid Day Meal Scheme (MDMS) </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Environment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/time-bomb-ticking-52.html"
class="left postionrel">Time Bomb Ticking </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/water-and-sanitation-55.html"
class="left postionrel">Water and Sanitation </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/impact-on-agriculture-54.html"
class="left postionrel">Impact on Agriculture </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Law & Justice</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/social-justice-20500.html"
class="left postionrel">Social Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/access-to-justice-47.html"
class="left postionrel">Access to Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/human-rights-56.html"
class="left postionrel">Human Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/corruption-35.html"
class="left postionrel">Corruption </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/general-insecurity-46.html"
class="left postionrel">General Insecurity </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/disaster-relief-49.html"
class="left postionrel">Disaster & Relief </a>
</p>
</div>
</div>
</div>
</div>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page "><a target="_blank" href="https://im4change.in/nceus_reports.php">NCEUS reports</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children parent-list ">
<a target="_blank" href="https://im4change.in/about-us-9.html">About Us <span
class="sub-indicator"></span></a>
<ul class="sub-menu aboutmenu">
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/objectives-8.html">Objectives</a>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/contactus.php">Contact
Us</a></li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/about-us-9.html">About
Us</a></li>
</ul>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children ">
<a target="_blank" href="https://im4change.in/fellowships.php" title="Fellowships">Fellowships</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/media-workshops.php">Workshops</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/research.php">Research</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/links-64">Partners</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
id="menu-item-539"><a target="_blank" href="https://im4change.in/hindi/"
class="langbutton langlinkfont17">हिन्दी</a></li>
</ul>
</div> </div>
<!-- <div style="float: right;">
<script async src="https://cse.google.com/cse.js?cx=18b4f2e0f11bed3dd"></script>
<div class="gcse-search"></div>
</div> -->
<div class="search-block" style=" margin-left: 8px; margin-right: 7px;">
<form method="get" id="searchform" name="searchform"
action="https://im4change.in/search"
onsubmit="return searchvalidate();">
<button class="search-button" type="submit" value="Search"></button>
<input type="text" id="s" name="qryStr" value=""
onfocus="if (this.value == 'Search...') {this.value = '';}"
onblur="if (this.value == '') {this.value = 'Search...';}">
</form>
</div>
</nav>
</header>
<div class="container">
<div id="main-content" class=" main1 container fade-in animated3 sidebar-narrow-left">
<div class="content-wrap">
<div class="content" style="width: 900px;min-height: 500px;">
<section class="cat-box recent-box innerCatRecent">
<h1 class="cat-box-title">How Women Pay the Price for Population Control -Ruhi Kandhari</h1>
<a href="JavaScript:void(0);" onclick="return shareArticle(26095);">
<img src="https://im4change.in/images/email.png?1582080630" border="0" width="24" align="right" alt="Share this article"/> </a>
<a href="https://im4change.in/latest-news-updates/how-women-pay-the-price-for-population-control-ruhi-kandhari-4674133/print"
rel="nofollow">
<img src="https://im4change.in/images/icon-print.png?1582080630" border="0" width="24" align="right" alt="Share this article"/>
</a>
</section>
<section class="recent-box innerCatRecent">
<small class="pb-1"><span class="dateIcn">
<img src="https://im4change.in/images/published.svg?1582080666" alt="published"/>
Published on</span><span class="text-date"> Oct 7, 2014</span>
<span
class="dateIcn">
<img src="https://im4change.in/images/modified.svg?1582080666" alt="modified"/> Modified on </span><span class="text-date"> Oct 7, 2014</span>
</small>
</section>
<div class="clear"></div>
<div style="padding-top: 10px;">
<div class="innerLineHeight">
<div class="middleContent innerInput latest-news-updates">
<table>
<tr>
<td>
<div>
<div align="justify">-Tehelka</div><p align="justify"><em>Despite the serious toll it takes on women's health, female sterilisation remains the most prevalent form of contraception in India. </em></p><p align="justify">While memories of the 21 months of Emergency in 1975-77, imposed by the then prime minister Indira Gandhi, survives even today in the minds of Indian men as the fear of forced sterilisation, the country's population control policies have shifted over the years since then to target the politically less powerful and vulnerable poor women. Almost the entire burden of what is euphemistically called "family planning" is today borne by women. And it has taken a toll on the health of large sections of women in the country.</p><p align="justify"><img src="https://im4change.in/siteadmin/tinymce/uploaded/Contraception.jpg" alt="Contraception" width="660" height="508" /> </p><p align="justify">In fact, the mainstay of our population control strategy comprises two methods targeted at women - tubectomy (female sterilisation surgery) and insertion of an intrauterine device (IUD) also known as Copper-T. Neither method is known to be suitable for all women. Yet, in the rush to meet targets, these methods are widely promoted and their adverse effects on women ignored. The public health infrastructure is not geared to manage contraception, the staff is not trained in counselling women or seek their informed consent, and pain is considered an acceptable side-effect.</p><p align="justify">According to the latest National Family Health Survey, conducted in 2005-06, a third of the women in the reproductive age group have undergone surgery for sterilisation and thousands have been inserted with IUDs, with or without their consent, at some point in their lives. After months of suffering pain, many women have to visit private clinics to get the IUDs removed as the government hospitals largely refuse to do so.</p><p align="justify">The World Contraception Day was observed on 26 September. The time is apt to take a hard look at India's population control policies from the perspective of the women who are forced to suffer its consequences.</p><p align="justify">Take the case of 30-year-old Rajkumari from New Delhi, who underwent tubectomy five years ago. In five years of marriage, she had three children, followed by three abortions. A social health worker appointed by the state government had convinced her that this was the only way to avoid pregnancy. Her husband, however, was never counselled to use contraception.</p><p align="justify">Since the surgery, Rajkumari has not been able to sleep peacefully on most nights. She often suffers from recurring headaches, hot flashes, night sweats and stabbing pain in her abdomen. In the month following her surgery, she visited the government hospital several times, but the doctors only prescribed her medicines to control the symptoms. "The medicines only offered temporary relief. My life has been a curse for the past five years with constant suffering," she says.</p><p align="justify">Her neighbour, 23-year-old Pushpa, also narrates a similar tale of pain. The nurse at a public health facility inserted her with an IUD after she delivered her first child. Her consent was not sought. The procedure was done after getting the consent form signed by her husband, a daily wage labourer who had studied up to Class V. He wasn't explained what an IUD is and what the form was for.</p><p align="justify">Pushpa was dizzy when she returned home. She bled profusely, became pale over time and stayed bed-ridden. Her periods lasted up to two weeks sometimes. She lost her appetite, became weak and was unable to feed her baby on most days. When she went back to the hospital, she was prescribed antibiotics and painkillers. But she continued to bleed and suffered from pain in her abdomen. It took her three months to save enough money to get the IUD removed at a private clinic.</p><p align="justify">The common known side-effects of IUDs are nausea, changes in menstrual bleeding and severe cramps. Sterilisation, on the other hand, is a risky surgery that may lead to internal infection or bleeding, injury to internal organs and even death.</p><p align="justify">There are thousands of women like Rajkumari and Pushpa who have suffered the terrible side-effects of tubectomy and IUDs.</p><p align="justify">Stuck on a wall in the lobby of the office of New Delhi-based NGO Centre for Health and Social Justice (CHSJ) is a clipping of a June 2013 article by the Bloomberg news service headlined ‘Pushing Indian Women toward Sterilisation'. It tells the story of Sumati Devi, who underwent sterilisation on an "operating table with bloody sheets". The operation was done with a rusted scalpel and she was neither counselled nor asked for her consent.</p><p align="justify">Instead, she was given some cash as an "incentive".</p><p align="justify">The article threw light on how 10 times more women than men undergo sterilisation surgeries in filthy "sterilisation camps", even though female sterilisation involves a more complicated operation than male vasectomy.</p><p align="justify">Another clipping from February 2012 headlined ‘Pregnant woman bleeds to death after sterilisation' (The Times of India) told the story of a 35-year-old pregnant woman who bled to death in Balaghat district of Madhya Pradesh while the doctors were trying to sterilise her.</p><p align="justify">She had been pregnant with twins - both girls - for 12 weeks when the operation was conducted. She died a few hours after she began bleeding on the operation table because the doctors did not follow the basic protocol of medically screening women before the sterilisation operation.</p><p align="justify">There was also a clipping of a January 2012 story titled ‘Barrack-room surgery in Bihar's backwaters' about a sterilisation camp conducted by an NGO in a hamlet in Araria district without any operation theatre, where 61 tubectomy surgeries were carried out at a breakneck speed using expired medicines.</p><p align="justify">Another clipping on display was of a March 2012 article titled ‘Freebies lengthen sterilisation queues' (The Deccan Herald) talked of how a district administration won a Tata Nano car for meeting sterilisation targets. Giving LPG connections to every family from which a woman underwent tubectomy, the administration had got over 2,000 tubectomy surgeries carried out in just three days.</p><p align="justify">According to the most recent data collected in 2012-13 under the District Level Household and Facility Survey, state governments increasingly prefer female sterilisation as a mode of family planning even though it is one of the most risky contraception methods. In Andhra Pradesh, for example, 63 percent women in the fertile age range had been operated upon in 2012-13 as compared to 60 percent in 2007-08. During the same period, the number of men who underwent sterilisation dropped from 4 to 2 percent. Similarly, in Maharashtra, the percentage of women who underwent sterilisation increased from 52 to 54 percent, while the corresponding figure for men dropped from 3 to 1 percent. In Haryana and Punjab, one-third of the women in the reproductive age range have been sterilised.</p><p align="justify">Although tubectomies involve a serious chance of surgical infections and post-operative complications, state governments continue to promote "camps" where these are conducted on thousands of women without any proper health infrastructure and in unsanitary conditions, in a hurry to meet targets. This is despite the fact that vasectomy for men is a relatively non-invasive procedure with little risk of surgical infections and the men undergoing the procedure are usually fit enough to walk only minutes later.</p><p align="justify">"The government's focus is only on terminal methods targeted at women. Men are hardly involved in the family planning programme. They need to be involved, not as targets for non-scalpel vasectomy but as partners within a gender- equality paradigm," says Dr Abhijeet Das, director of CHSJ and an assistant professor at the Department of Global Health, University of Washington, Seattle, USA. For the past two decades, Das has been observing persuasive population control programmes, advising the government and is also part of various national and international networks, including the National Alliance on Maternal Health and Human Rights, Healthwatch Forum and MenEngage, a global alliance on men and gender equality.</p><p align="justify">The 2012-13 survey also shows indicators that define the "quality of family planning services" remain abysmally low. Most women are unaware of other means of contraception and the known side-effects of sterilisation. Even when they are counselled, the counselling is manipulative as the staff has already decided which contraceptive method a woman needs. In Maharashtra, only 17 percent of the women were told about the side-effects, while the figure was 14 percent in Punjab and 11 percent in Andhra Pradesh and Haryana. According to the District Level Household & Facility Survey 2007-08, 40 percent of the women who underwent tubectomy in public health facilities across India were illiterate, indicating that tubectomy was not the "chosen" form of contraception.</p><p align="justify">Despite the problems associated with tubectomies, state governments continue to set targets for sterilisation surgeries. The reply to an RTI query showed that around 1,000 women were targeted for tubectomy in just west Delhi over the months of January, February and March this year.</p><p align="justify">The two extremes of the debate on how to stabilise the population are represented by the coercive sterilisation drive associated with Indira Gandhi's son Sanjay Gandhi during the Emergency, on the one hand, and senior Congress politician Karan Singh's statement at the 1974 World Population Conference in Bucharest, Romania, that "development is the best contraceptive", on the other. For a long time, the dominant thinking globally was in favour of coercive policies.</p><p align="justify">Internationally, this debate came to rest at the International Conference on Population and Development 1994 (ICPD 94) in Cairo, Egypt. At ICPD 94, civil society activists from around the world shared experiences of coercive population policies and convinced 179 national governments to see "population" as people, not a number. Economists like Amartya Sen had also proved by then that improvements in women's education and healthcare automatically result in smaller families without any need for authoritative population control policies.</p><p align="justify">ICPD 94 brought about a "paradigm shift". The governments agreed to abide by reproductive rights and honour gender equality while providing universal access to family planning, sexual and reproductive health services. The Indian government, too, grudgingly committed to place individuals at the centre of development. However, the state governments in India by and large do not follow this principle in practice and it is not uncommon for politicians, bureaucrats, judges and the educated, urban middle class to blame India's large population for nearly all the problems plaguing the country and favour force over cooperation.</p><p align="justify">Until ICPD 94, population was considered a dirty word - a dangerous "bomb" that would explode if not controlled. In the early 1950s, more babies were surviving in the newly-independent countries and fewer children were being born in the richer countries, leading to a fear of "overpopulation" in the Global South. This led to the formation in 1952 of two NGOs - the Population Council and the International Planned Parenthood Federation (IPPF) - in New York and Bombay, respectively. They were set up with the purpose of influencing the US government to orient the US Agency for International Development (USAID) towards population control in the Third World, alerting Americans to the danger of population "explosion" and raising funds for international birth control programmes.</p><p align="justify">An advertisement for a joint campaign by the two NGOs read: "A world of mass starvation in underdeveloped countries will be a world of chaos, riots and war. And a perfect breeding ground for communism... Our own national interests demand that we go all out to help the underdeveloped countries control their populations."</p><p align="justify">The political agenda was reinforced and validated by Stanford University Professor Paul R Ehrlich, who authored The Population Bomb in 1968. He emphasised birth control at any cost with the use of contraceptives, mass sterilisation and pre-natal sex determination (so that parents can design the family sex composition). The US government was soon convinced. In 1974, National Security Study Memorandum 200 of the National Security Council asserted that population growth in poor countries posed a problem for the security of the US. That is how the US and other industrialised countries, which had achieved lower birth rates due to improvements in education, healthcare and incomes, without any coercive population control policies, became the biggest proponents of the latter.</p><p align="justify">India could not remain unaffected by the discourse. In 1970, JRD Tata formed the Population Foundation of India with money from the Ford Foundation for population control advocacy in India. While the country's population initially focussed on vasectomy of men and stayed clear of female sterilisation, considering the risk of infection, the tide had turned by the 1980s. The infamous coercive male sterilisation drives of the Emergency period gave way to the setting of targets for female sterilisation, which continues to dominate the population control policy.</p><p align="justify">In 1992, a study by Dr Rani Bang and Dr Abhay Bang demonstrated that women had more faith in indigenous methods of contraception than the modern ones because they commonly associated the latter with adverse effects such as backache, abdominal pain, weakness and irregular or excessive menstruation. Women also found that healthcare professionals were often insensitive to these complaints and regarded them as minor and insignificant side-effects that should be ignored.</p><p align="justify">ICPD 94 was the culmination of the coming together of academics, activists and the medical community in efforts to propose an alternative perspective on population control policies. They showed how a policy of targets, incentives and disincentives under the National Family Planning Programme had made women mute recipients suffering quietly.</p><p align="justify">Among the participants at ICPD 94 was an IAS officer, AR Nanda, who was then the secretary at the Union Ministry of Health. After he returned from Cairo, he took up the mantle to reorient the population policy. The second half of the 1990s saw a new target-free approach, which focussed on combining contraception needs with providing reproductive and child health. Nanda also drafted the landmark National Population Policy (NPP) 2000, which stressed on improvements in human development, gender equality and reproductive health to stabilise population growth.</p><p align="justify">"In 1999, when I proposed the NPP, a few MPs supported the two pillars of the policy - informed choice and informed consent - but it was largely criticised in Parliament," says Nanda, who has since retired from the government, but continues to advise the National Coalition Against Two-Child Norm, an advocacy group of NGOs, academics and activists concerned with promoting policies that empower people to exercise their reproductive rights and choice.</p><p align="justify">The NPP 2000 begins with a statement that "the overriding objective of economic and social development is to improve (the) quality of life that people lead, to enhance their well-being and to provide them with opportunities and choices to become productive assets in society". The policy recommended the empowerment of women through enhanced access to education, employment opportunities and quality healthcare.</p><p align="justify">The policy, however, failed to influence a large section of politicians who continued to see population as a problem. In May 2000, when India's population crossed the one-billion mark, the then prime minister Atal Bihari Vajpayee said: "This is a serious matter that is both cause for concern and introspection - concern over the impact that a runaway population growth is bound to have on the nation's economic, natural and other resources; introspection over where we went wrong and how we can stabilise our population... If the present growth rate of our population remains unchecked, India will become the world's most populous country by the middle of this century, with people clamouring for a share of shrinking natural resources."</p><p align="justify">Opposition to NPP 2000 continued even after it was adopted. Population being a subject on the Concurrent List, the state governments are not obliged to follow anything that the Centre prescribes on population control. They have their own policies that in most cases go against NPP 2000. For instance, Uttar Pradesh introduced contraceptives such as injectables and implants, which are proven to be unsafe for women; Rajasthan promoted a lottery scheme for those who opt for sterilisation; and Bihar contracted out tubectomy surgeries to private operators and NGOs.</p><p align="justify">"The language used in talking about population stabilisation changed after ICPD 94 but the mindset remained more or less the same," says Nanda. "Even at the national level, male responsibility and gender equity were largely ignored. The state governments favour setting of targets and promoting terminal methods because the results are easy to measure."</p><p align="justify">Clearly, despite all the talk of empowering women, their reproductive autonomy - the right to choose whether to have children or not and the freedom to choose the methods of fertility management based on access to proper information - has been largely ignored in the policies and practices promoted by various governments in India.</p><p align="justify">Unfortunately, India has seen a reduced prevalence of condom use with women remaining unequal targets of the family planning burden. As the dominant, irreversible methods of population control take a toll on women's health, there is indeed a need for reorienting it towards the promotion of temporary and reversible methods such as condoms, which also provide a barrier against sexually transmitted diseases.</p><p align="justify">--</p><p align="justify">The downside of contraception</p><p align="justify">Disadvantages and side-effects of various contraceptive methods</p><p align="justify">Oral Contraceptive Pill: Nausea, mild headaches, tender breasts, spotting between periods, irregular bleeding, moodiness, vomiting within two hours of taking a pill, severe diarrhoea and vomiting for more than 24 hours</p><p align="justify">Copper-bearing IUDs: Menstrual changes in early months, longer and heavy menstrual periods, bleeding or spotting between periods, more cramps or pain during period. Uncommon sideeffects include severe cramps and pain beyond first three-five days of insertion, heavy menstrual bleeding or bleeding between periods, possibly contributing to anaemia and possibility of perforation if not inserted properly. It does not protect against sexually transmitted diseases (STDs) including HIV/AIDs. Medical procedure, including pelvic examination, is needed to insert the IUD. Occasionally, a woman faints during the insertion procedure. A trained healthcare provider must remove the IUD. The IUD may come out of the uterus possibly without the woman knowing about it (more common when the IUD is inserted soon after childbirth)</p><p align="justify">Vasectomy: Uncomfortable for two or three days, pain in scrotum, swelling and bruising and brief feeling of faintness after the procedure. Rare complications of surgery include bleeding or infection at the incision site or inside the incision, blood clots in the scrotum. No protection against STDs, including HIV/AIDs</p><p align="justify">Tubectomy: Uncommon complications include infection or bleeding at the incision, internal infection or bleeding, injury to internal organs and anaesthesia risk. No protection against STDs</p><p align="justify">Male Condom: Latex condoms may cause itching for a few people who are allergic to latex. Also, some people may be allergic to the lubricant on some brands of condoms. Small possibility that condom might slip off or break during sexual intercourse</p><p align="justify">(Source: Government reference manual)</p>
</div>
</td>
</tr>
</table>
</div>
</div>
</div>
<div class="clear"></div>
<br><a href="http://www.tehelka.com/how-women-pay-the-price-for-population-control-iod-birth-control-health-female-sterilisation/" class="re" target="_blank">Tehelka Magazine, Volume 11, Issue 41, 11 October 2014, http://www.tehelka.com/how-women-pay-the-price-for-population-control-iod-birth-control-health-female-sterilisation/</a><div class="clear"></div>
<div style="padding-top: 18px;">
<p class="post-tag">Tagged with:
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=gender discrimination"
title="gender discrimination">
gender discrimination </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Gender Equality"
title="Gender Equality">
Gender Equality </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Reproductive Health"
title="Reproductive Health">
Reproductive Health </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Contraception"
title="Contraception">
Contraception </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Population Control"
title="Population Control">
Population Control </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Health"
title="Health">
Health </a>
</p>
</div>
<div class="clear"></div>
<br><br>
<div class="widget-top">
<h4>Related Articles</h4>
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<ul id="recentcomments">
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/fifth-report-from-gambia-implicates-indian-drug-maker-for-contaminated-syrups-banjot-kaur.html"
title="Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur">
Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-may-have-seen-steepest-dip-in-multidimensional-poverty-among-110-nations-as-per-undp-data-nikhil-rampal.html"
title="India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal">
India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/health-among-top-three-priorities-for-indian-voters-after-jobs-and-education-survey-shows-oliver-heath-jyoti-mishra-louise-tillin-sandhya-venkateswaran.html"
title="Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran">
Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/prevalence-of-zero-food-among-infants-and-young-children-in-india-patterns-of-change-across-the-states-and-union-territories-of-india-1993-2021-the-lancet.html"
title="Prevalence of Zero-Food among infants and young children in India - The Lancet ">
Prevalence of Zero-Food among infants and young children in India - The Lancet </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-s-sustainability-goals-at-risk-because-of-extreme-heatwaves-carbon-copy.html"
title="India's Sustainability Goals at Risk Because of Extreme Heatwaves - Carbon Copy">
India's Sustainability Goals at Risk Because of Extreme Heatwaves - Carbon Copy </a>
</li>
</ul>
</div>
<div class="comment-respond" id="respond">
<a name="commentbox"> </a>
<h3 class="comment-reply-title" id="reply-title">Write Comments</h3>
<form method="post" accept-charset="utf-8" role="form" action="/latest-news-updates/how-women-pay-the-price-for-population-control-ruhi-kandhari-4674133.html"><div style="display:none;"><input type="hidden" name="_method" value="POST"/></div> <form class="comment-form" id="commentform" method="post" action="#commentbox" onSubmit="return validate()"
name="cmtform">
<input type="hidden" name="cmttype" value="articlecmt"/>
<input type="hidden" name="article_id" value="26095"/>
<p class="comment-notes">Your email address will not be published. Required fields are marked <span
class="required">*</span></p>
<p class="comment-form-author">
<label for="commenterName">Name</label>
<span class="required">*</span>
<input type="text" aria-required="true" size="30"
value=""
name="commenterName" id="commenterName" required="true">
</p>
<p class="comment-form-email">
<label for="commenterEmail">Email</label> <span class="required">*</span>
<input aria-required="true" size="30" name="commenterEmail" id="commenterEmail" type="email"
value=""
required="true">
</p>
<p class="comment-form-contact">
<label for="commenterPh">Contact No.</label>
<input type="text" size="30"
value=""
name="commenterPh" id="commenterPh">
</p>
<p class="comment-form-comment">
<label for="comment">Comment</label>
<textarea aria-required="true" required="true" rows="8" cols="45" name="comment"
id="comment"></textarea>
</p>
<p class="comment-form-comment">
<label for="comment">Type the characters you see in the image below <span class="required">*</span><br><img
class="captchaImg"
src="https://im4change.in/securimage_show_art.php?tk=1115961128" alt="captcha"/>
</label>
</p>
<input type="text" name="vrcode" required="true"/>
<p class="form-submit" style="width: 200px;">
<input type="submit" value="Post Comment" id="submit" name="submit">
</p></form>
</div>
<style>
.ui-widget-content {
height: auto !important;
}
</style>
<div id="share-modal"></div>
<style>
.middleContent a{
background-color: rgba(108,172,228,.2);
}
.middleContent a:hover{
background-color: #418fde;
border-color: #418fde;
color: #000;
}
</style>
<script>
function shareArticle(article_id) {
var options = {
modal: true,
height: 'auto',
width: 600 + 'px'
};
$('#share-modal').html("");
$('#share-modal').load('https://im4change.in/share_article?article_id=' + article_id).dialog(options).dialog('open');
}
function postShare() {
var param = 'article_id=' + $("#article_id").val();
param = param + '&y_name=' + $("#y_name").val();
param = param + '&y_email=' + $("#y_email").val();
param = param + '&f_name=' + $("#f_name").val();
param = param + '&f_email=' + $("#f_email").val();
param = param + '&y_msg=' + $("#y_msg").val();
$.ajax({
type: "POST",
url: 'https://im4change.in/post_share_article',
data: param,
success: function (response) {
$('#share-modal').html("Thank You, Your message posted to ");
}
});
return false;
}
</script> </div>
</div>
<!-- Right Side Section Start -->
<!-- MAP Section START -->
<aside class="sidebar indexMarg">
<div class="ad-cell">
<a href="https://im4change.in/statemap.php" title="">
<img src="https://im4change.in/images/map_new_version.png?1582080666" alt="India State Map" class="indiamap" width="232" height="252"/> </a>
<div class="rightmapbox">
<div id="sideOne" class="docltitle"><a href="https://im4change.in/state-report/india/36" target="_blank">DOCUMENTS/
REPORTS</a></div>
<div id="sideTwo" class="statetitle"><a href="https://im4change.in/states.php"target="_blank">STATE DATA/
HDRs.</a></div>
</div>
<div class="widget widgePadTop"></div>
</div>
</aside>
<!-- MAP Section END -->
<aside class="sidebar sidePadbottom">
<div class="rightsmlbox1" >
<a href="https://im4change.in/knowledge_gateway" target="_blank" style="color: #035588;
font-size: 17px;">
KNOWLEDGE GATEWAY
</a>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/newsletter" target="_blank">
NEWSLETTER
</a>
</p>
</div>
</div>
<div class="rightsmlbox1" style="height: 325px;">
<div>
<p class="rightsmlbox1_title">
Interview with Prof. Ravi Srivastava
</p>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/video/interview-with-prof-ravi-srivastava-on-current-economic-crisis">
<img width="250" height="200" src="/images/interview_video_home.jpg" alt="Interview with Prof. Ravi Srivastava"/>
</a>
<!--
<iframe width="250" height="200" src="https://www.youtube.com/embed/MmaTlntk-wc" frameborder="0" allow="accelerometer; autoplay; encrypted-media; gyroscope; picture-in-picture" allowfullscreen=""></iframe>-->
</p>
<a href="https://im4change.in/videogallery" class="more-link CatArchalAnch1" target="_blank">
More videos
</a>
</div>
</div>
<div class="rightsmlbox1">
<div>
<!--div id="sstory" class="rightboxicons"></div--->
<p class="rightsmlbox1_title"><a href="https://im4change.in/list-success-stories" target="_blank">Success Stories</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/interviews" target="_blank">Interviews</a>
</p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a href="https://www.commoncause.in/page.php?id=10" >Donate</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/marquee"
class="isf_link more-link" title="India Focus?" style="border: 4px solid #fdd922;width: 90%;background-color: #fdd922;text-align: center;color: #000000;font-size:18px" target="_blank">India Focus</a></p> </div>
</div>
<div class="rightsmlbox1" style="height: 104px !important;">
<a href="https://im4change.in/quarterly_reports.php" target="_blank">
Quarterly Reports on Effect of Economic Slowdown on Employment in India (2008 - 2015)
</a>
</div>
<!-- <div class="rightsmlbox1">
<a href="https://play.google.com/store/apps/details?id=com.im4.im4change" target="_blank">
</a></div> -->
<!-- <section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">Most Visited</h2>
</section> -->
<!-- accordion Starts here -->
<!-- <div id="accordion" class="accordMarg">
</div> -->
<!-- accordion ends here -->
<!-- Widget Tag Cloud Starts here -->
<div id="tag_cloud-2" class="widget widget_tag_cloud">
<section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">MOST VISITED TAGS</h2>
</section>
<div class="widget-top wiPdTp">
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<div class="tagcloud">
<a href="https://im4change.in/search?qryStr=Agriculture"
target="_blank" class="tag-link-4 font4">Agriculture</a>
<a href="https://im4change.in/search?qryStr=Food Security"
target="_blank" class="tag-link-4 font4">Food Security</a>
<a href="https://im4change.in/search?qryStr=Law and Justice"
target="_blank" class="tag-link-4 font4">Law and Justice</a>
<a href="https://im4change.in/search?qryStr=Health"
target="_blank" class="tag-link-4 font4">Health</a>
<a href="https://im4change.in/search?qryStr=Right to Food"
target="_blank" class="tag-link-4 font4">Right to Food</a>
<a href="https://im4change.in/search?qryStr=Corruption"
target="_blank" class="tag-link-4 font4">Corruption</a>
<a href="https://im4change.in/search?qryStr=farming"
target="_blank" class="tag-link-4 font4">farming</a>
<a href="https://im4change.in/search?qryStr=Environment"
target="_blank" class="tag-link-4 font4">Environment</a>
<a href="https://im4change.in/search?qryStr=Right to Information"
target="_blank" class="tag-link-4 font4">Right to Information</a>
<a href="https://im4change.in/search?qryStr=NREGS"
target="_blank" class="tag-link-4 font4">NREGS</a>
<a href="https://im4change.in/search?qryStr=Human Rights"
target="_blank" class="tag-link-4 font4">Human Rights</a>
<a href="https://im4change.in/search?qryStr=Governance"
target="_blank" class="tag-link-4 font4">Governance</a>
<a href="https://im4change.in/search?qryStr=PDS"
target="_blank" class="tag-link-4 font4">PDS</a>
<a href="https://im4change.in/search?qryStr=COVID-19"
target="_blank" class="tag-link-4 font4">COVID-19</a>
<a href="https://im4change.in/search?qryStr=Land Acquisition"
target="_blank" class="tag-link-4 font4">Land Acquisition</a>
<a href="https://im4change.in/search?qryStr=mgnrega"
target="_blank" class="tag-link-4 font4">mgnrega</a>
<a href="https://im4change.in/search?qryStr=Farmers"
target="_blank" class="tag-link-4 font4">Farmers</a>
<a href="https://im4change.in/search?qryStr=transparency"
target="_blank" class="tag-link-4 font4">transparency</a>
<a href="https://im4change.in/search?qryStr=Gender"
target="_blank" class="tag-link-4 font4">Gender</a>
<a href="https://im4change.in/search?qryStr=Poverty"
target="_blank" class="tag-link-4 font4">Poverty</a>
<a href="https://im4change.in/search?qryStr=Farm Laws" target="_blank" class="tag-link-4 font4">Farm Laws
</a>
<a href="https://im4change.in/search?qryStr=Citizenship Amendment Act" target="_blank" class="tag-link-4 font4">Citizenship Amendment Act
</a>
<a href="https://im4change.in/search?qryStr=CAA NPR NRIC" target="_blank" class="tag-link-4 font4">CAA NPR NRIC
</a>
<a href="https://im4change.in/search?qryStr=Job Losses" target="_blank" class="tag-link-4 font4">Job Losses
</a>
<a href="https://im4change.in/search?qryStr=Migrant Workers" target="_blank" class="tag-link-4 font4">Migrant Workers
</a>
<a href="https://im4change.in/search?qryStr=Unemployment" target="_blank" class="tag-link-4 font4">Unemployment
</a>
<a href="https://im4change.in/search?qryStr=PMGKAY" target="_blank" class="tag-link-4 font4">PMGKAY
</a>
<a href="https://im4change.in/search?qryStr=PM-KISAN" target="_blank" class="tag-link-4 font4">PM-KISAN
</a>
<a href="https://im4change.in/search?qryStr=PM-CARES" target="_blank" class="tag-link-4 font4">PM-CARES
</a>
<a href="https://im4change.in/search?qryStr=LFPR" target="_blank" class="tag-link-4 font4">LFPR
</a>
</div>
</div>
</div>
<!-- Widget Tag Cloud Ends here -->
</aside>
<!-- Right Side Section End -->
</div>
<section class="cat-box cats-review-box footerSec">
<h2 class="cat-box-title vSec CatArcha">Video
Archives</h2>
<h2 class="cat-box-title CatArchaTitle">Archives</h2>
<div class="cat-box-content">
<div class="reviews-cat">
<div class="CatArchaDiv1">
<div class="CatArchaDiv2">
<ul>
<li>
<a href="https://im4change.in/news-alerts-57/moving-upstream-luni-fellowship.html" target="_blank">
Moving Upstream: Luni – Fellowship </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/135-million-indians-exited-multidimensional-poverty-as-per-government-figures-is-that-the-same-as-poverty-reduction.html" target="_blank">
135 Million Indians Exited “Multidimensional" Poverty as per Government... </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/explainer-why-are-tomato-prices-on-fire.html" target="_blank">
Explainer: Why are Tomato Prices on Fire? </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/nsso-survey-only-39-1-of-all-households-have-drinking-water-within-dwelling-46-7-of-rural-households-use-firewood-for-cooking.html" target="_blank">
NSSO Survey: Only 39.1% of all Households have Drinking... </a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/news-alerts-57"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/I51LYnP8BOk/1.jpg"
alt=" Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Short-Video-on-im4change-Hindi-website-Inclusive-Media-for-Change" target="_blank">
Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/kNqha-SwfIY/1.jpg"
alt=" "Session 1: Scope of IDEA and AgriStack" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-1- Scope-of-IDEA-and-AgriStack-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 1: Scope of IDEA and AgriStack" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/6kIVjlgZItk/1.jpg"
alt=" "Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-2-Farmer-Centric-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/2BeHTu0y7xc/1.jpg"
alt=" "Session 3: Future of Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-3-Future-of-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 3: Future of Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="divWidth">
<ul class="divWidthMarg">
<li>
<a href="https://im4change.in/video/Public-Spending-on-Agriculture-in-India-Source-Foundation-for-Agrarian-Studies"
title="Public Spending on Agriculture in India (Source: Foundation for Agrarian Studies)" target="_blank">
Public Spending on Agriculture in India (Source: Foundation for...</a>
</li>
<li>
<a href="https://im4change.in/video/Agrarian-Change-Seminar-Protests-against-the-New-Farm-Laws-in-India-by-Prof-Vikas-Rawal-JNU-Source-Journal-Of-Agrarian-Change"
title="Agrarian Change Seminar: 'Protests against the New Farm Laws in India' by Prof. Vikas Rawal, JNU (Source: Journal Of Agrarian Change) " target="_blank">
Agrarian Change Seminar: 'Protests against the New Farm Laws...</a>
</li>
<li>
<a href="https://im4change.in/video/Webinar-Ramrao-The-Story-of-India-Farm-Crisis-Source-Azim-Premji-University"
title="Webinar: Ramrao - The Story of India's Farm Crisis (Source: Azim Premji University)" target="_blank">
Webinar: Ramrao - The Story of India's Farm Crisis...</a>
</li>
<li>
<a href="https://im4change.in/video/water-and-agricultural-transformation-in-India"
title="Water and Agricultural Transformation in India: A Symbiotic Relationship (Source: IGIDR)" target="_blank">
Water and Agricultural Transformation in India: A Symbiotic Relationship...</a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/videogallery"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
</div>
</div>
</div>
</section> </div>
<div class="clear"></div>
<!-- Footer option Starts here -->
<div class="footer-bottom fade-in animated4">
<div class="container">
<div class="social-icons icon_flat">
<p class="SocialMargTop"> Website Developed by <a target="_blank" title="Web Development"
class="wot right"
href="http://www.ravinderkhurana.com/" rel="nofollow">
RAVINDErkHURANA.com</a></p>
</div>
<div class="alignleft">
<a
target="_blank" href="https://im4change.in/objectives-8.html"
class="link"
title="Objectives">Objectives</a> | <a
target="_blank" href="https://im4change.in/about-us-9.html"
class="link" title="About Us">About Us</a> | <a
target="_blank" href="https://im4change.in/media-workshops.php"
class="ucwords">Workshops</a> | <a
target="_blank" href="https://im4change.in/disclaimer/disclaimer-149.html"
title="Disclaimer">Disclaimer</a> </div>
</div>
</div>
<!-- Footer option ends here -->
</div>
<div id="connect">
<a target="_blank"
href="http://www.facebook.com/sharer.php?u=https://im4change.in/latest-news-updates/how-women-pay-the-price-for-population-control-ruhi-kandhari-4674133.html"
title="Share on Facebook">
<img src="https://im4change.in/images/Facebook.png?1582080640" alt="share on Facebook" class="ImgBorder"/>
</a><br/>
<a target="_blank"
href="http://twitter.com/share?text=Im4change&url=https://im4change.in/latest-news-updates/how-women-pay-the-price-for-population-control-ruhi-kandhari-4674133.html"
title="Share on Twitter">
<img src="https://im4change.in/images/twitter.png?1582080632" alt="Twitter" class="ImgBorder"/> </a>
<br/>
<a href="/feeds" title="RSS Feed" target="_blank">
<img src="https://im4change.in/images/rss.png?1582080632" alt="RSS" class="ImgBorder"/>
</a>
<br/>
<a class="feedback-link" id="feedbackFormLink" href="#">
<img src="https://im4change.in/images/feedback.png?1582080630" alt="Feedback" class="ImgBorder"/>
</a> <br/>
<a href="javascript:function iprl5(){var d=document,z=d.createElement('scr'+'ipt'),b=d.body,l=d.location;try{if(!b)throw(0);d.title='(Saving...) '+d.title;z.setAttribute('src',l.protocol+'//www.instapaper.com/j/WKrH3R7ORD5p?u='+encodeURIComponent(l.href)+'&t='+(new Date().getTime()));b.appendChild(z);}catch(e){alert('Please wait until the page has loaded.');}}iprl5();void(0)"
class="bookmarklet" onclick="return explain_bookmarklet();">
<img src="https://im4change.in/images/read-it-later.png?1582080632" alt="Read Later" class="ImgBorder"/> </a>
</div>
<!-- Feedback form Starts here -->
<div id="feedbackForm" class="overlay_form" class="ImgBorder">
<h2>Contact Form</h2>
<div id="contactform1">
<div id="formleft">
<form id="submitform" action="/contactus.php" method="post">
<input type="hidden" name="submitform" value="submitform"/>
<input type="hidden" name="salt_key" value="a0e0f2c6a0644a70e57ad2c96829709a"/>
<input type="hidden" name="ref" value="feedback"/>
<fieldset>
<label>Name :</label>
<input type="text" name="name" class="tbox" required/>
</fieldset>
<fieldset>
<label>Email :</label>
<input type="text" name="email" class="tbox" required/>
</fieldset>
<fieldset>
<label>Message :</label>
<textarea rows="5" cols="20" name="message" required></textarea>
</fieldset>
<fieldset>
Please enter security code
<div class="clear"></div>
<input type="text" name="vrcode" class="tbox"/>
</fieldset>
<fieldset>
<input type="submit" class="button" value="Submit"/>
<a href="#" id="closefeedbakcformLink">Close</a>
</fieldset>
</form>
</div>
<div class="clearfix"></div>
</div>
</div>
<div id="donate_popup" class="modal" style="max-width: 800px;">
<table width="100%" border="1">
<tr>
<td colspan="2" align="center">
<b>Support im4change</b>
</td>
</tr>
<tr>
<td width="25%" valign="middle">
<img src="https://im4change.in/images/logo2.jpg?1582080632" alt="" width="100%"/> </td>
<td style="padding-left:10px;padding-top:10px;">
<form action="https://im4change.in/donate" method="get">
<table width="100%" cellpadding="2" cellspacing="2">
<tr>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
10
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
100
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
1000
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
50
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
500
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
<input type="text" name="price" placeholder="?" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td colspan="3" align="right">
<input type="button" name="Pay" value="Pay"
style="width: 200px;background-color: rgb(205, 35, 36);color: #ffffff;"/>
</td>
</tr>
</table>
</form>
</td>
</tr>
</table>
</div><script type='text/javascript'>
/* <![CDATA[ */
var tievar = {'go_to': 'Go to...'};
/* ]]> */
</script>
<script src="/js/tie-scripts.js?1575549704"></script><script src="/js/bootstrap.js?1575549704"></script><script src="/js/jquery.modal.min.js?1578284310"></script><script>
$(document).ready(function() {
// tell the autocomplete function to get its data from our php script
$('#s').autocomplete({
source: "/autocomplete"
});
});
</script>
<script src="/vj-main-sw-register.js" async></script>
<script>function init(){var imgDefer=document.getElementsByTagName('img');for(var i=0;i<imgDefer.length;i++){if(imgDefer[i].getAttribute('data-src')){imgDefer[i].setAttribute('src',imgDefer[i].getAttribute('data-src'))}}}
window.onload=init;</script>
</body>
</html>'
}
$cookies = []
$values = [
(int) 0 => 'text/html; charset=UTF-8'
]
$name = 'Content-Type'
$first = true
$value = 'text/html; charset=UTF-8'
header - [internal], line ??
Cake\Http\ResponseEmitter::emitHeaders() - CORE/src/Http/ResponseEmitter.php, line 181
Cake\Http\ResponseEmitter::emit() - CORE/src/Http/ResponseEmitter.php, line 55
Cake\Http\Server::emit() - CORE/src/Http/Server.php, line 141
[main] - ROOT/webroot/index.php, line 39
LATEST NEWS UPDATES | How Women Pay the Price for Population Control -Ruhi Kandhari
How Women Pay the Price for Population Control -Ruhi Kandhari
Published on Oct 7, 2014 Modified on Oct 7, 2014
-Tehelka
Despite the serious toll it takes on women's health, female sterilisation remains the most prevalent form of contraception in India.
While memories of the 21 months of Emergency in 1975-77, imposed by the then prime minister Indira Gandhi, survives even today in the minds of Indian men as the fear of forced sterilisation, the country's population control policies have shifted over the years since then to target the politically less powerful and vulnerable poor women. Almost the entire burden of what is euphemistically called "family planning" is today borne by women. And it has taken a toll on the health of large sections of women in the country.
In fact, the mainstay of our population control strategy comprises two methods targeted at women - tubectomy (female sterilisation surgery) and insertion of an intrauterine device (IUD) also known as Copper-T. Neither method is known to be suitable for all women. Yet, in the rush to meet targets, these methods are widely promoted and their adverse effects on women ignored. The public health infrastructure is not geared to manage contraception, the staff is not trained in counselling women or seek their informed consent, and pain is considered an acceptable side-effect.
According to the latest National Family Health Survey, conducted in 2005-06, a third of the women in the reproductive age group have undergone surgery for sterilisation and thousands have been inserted with IUDs, with or without their consent, at some point in their lives. After months of suffering pain, many women have to visit private clinics to get the IUDs removed as the government hospitals largely refuse to do so.
The World Contraception Day was observed on 26 September. The time is apt to take a hard look at India's population control policies from the perspective of the women who are forced to suffer its consequences.
Take the case of 30-year-old Rajkumari from New Delhi, who underwent tubectomy five years ago. In five years of marriage, she had three children, followed by three abortions. A social health worker appointed by the state government had convinced her that this was the only way to avoid pregnancy. Her husband, however, was never counselled to use contraception.
Since the surgery, Rajkumari has not been able to sleep peacefully on most nights. She often suffers from recurring headaches, hot flashes, night sweats and stabbing pain in her abdomen. In the month following her surgery, she visited the government hospital several times, but the doctors only prescribed her medicines to control the symptoms. "The medicines only offered temporary relief. My life has been a curse for the past five years with constant suffering," she says.
Her neighbour, 23-year-old Pushpa, also narrates a similar tale of pain. The nurse at a public health facility inserted her with an IUD after she delivered her first child. Her consent was not sought. The procedure was done after getting the consent form signed by her husband, a daily wage labourer who had studied up to Class V. He wasn't explained what an IUD is and what the form was for.
Pushpa was dizzy when she returned home. She bled profusely, became pale over time and stayed bed-ridden. Her periods lasted up to two weeks sometimes. She lost her appetite, became weak and was unable to feed her baby on most days. When she went back to the hospital, she was prescribed antibiotics and painkillers. But she continued to bleed and suffered from pain in her abdomen. It took her three months to save enough money to get the IUD removed at a private clinic.
The common known side-effects of IUDs are nausea, changes in menstrual bleeding and severe cramps. Sterilisation, on the other hand, is a risky surgery that may lead to internal infection or bleeding, injury to internal organs and even death.
There are thousands of women like Rajkumari and Pushpa who have suffered the terrible side-effects of tubectomy and IUDs.
Stuck on a wall in the lobby of the office of New Delhi-based NGO Centre for Health and Social Justice (CHSJ) is a clipping of a June 2013 article by the Bloomberg news service headlined ‘Pushing Indian Women toward Sterilisation'. It tells the story of Sumati Devi, who underwent sterilisation on an "operating table with bloody sheets". The operation was done with a rusted scalpel and she was neither counselled nor asked for her consent.
Instead, she was given some cash as an "incentive".
The article threw light on how 10 times more women than men undergo sterilisation surgeries in filthy "sterilisation camps", even though female sterilisation involves a more complicated operation than male vasectomy.
Another clipping from February 2012 headlined ‘Pregnant woman bleeds to death after sterilisation' (The Times of India) told the story of a 35-year-old pregnant woman who bled to death in Balaghat district of Madhya Pradesh while the doctors were trying to sterilise her.
She had been pregnant with twins - both girls - for 12 weeks when the operation was conducted. She died a few hours after she began bleeding on the operation table because the doctors did not follow the basic protocol of medically screening women before the sterilisation operation.
There was also a clipping of a January 2012 story titled ‘Barrack-room surgery in Bihar's backwaters' about a sterilisation camp conducted by an NGO in a hamlet in Araria district without any operation theatre, where 61 tubectomy surgeries were carried out at a breakneck speed using expired medicines.
Another clipping on display was of a March 2012 article titled ‘Freebies lengthen sterilisation queues' (The Deccan Herald) talked of how a district administration won a Tata Nano car for meeting sterilisation targets. Giving LPG connections to every family from which a woman underwent tubectomy, the administration had got over 2,000 tubectomy surgeries carried out in just three days.
According to the most recent data collected in 2012-13 under the District Level Household and Facility Survey, state governments increasingly prefer female sterilisation as a mode of family planning even though it is one of the most risky contraception methods. In Andhra Pradesh, for example, 63 percent women in the fertile age range had been operated upon in 2012-13 as compared to 60 percent in 2007-08. During the same period, the number of men who underwent sterilisation dropped from 4 to 2 percent. Similarly, in Maharashtra, the percentage of women who underwent sterilisation increased from 52 to 54 percent, while the corresponding figure for men dropped from 3 to 1 percent. In Haryana and Punjab, one-third of the women in the reproductive age range have been sterilised.
Although tubectomies involve a serious chance of surgical infections and post-operative complications, state governments continue to promote "camps" where these are conducted on thousands of women without any proper health infrastructure and in unsanitary conditions, in a hurry to meet targets. This is despite the fact that vasectomy for men is a relatively non-invasive procedure with little risk of surgical infections and the men undergoing the procedure are usually fit enough to walk only minutes later.
"The government's focus is only on terminal methods targeted at women. Men are hardly involved in the family planning programme. They need to be involved, not as targets for non-scalpel vasectomy but as partners within a gender- equality paradigm," says Dr Abhijeet Das, director of CHSJ and an assistant professor at the Department of Global Health, University of Washington, Seattle, USA. For the past two decades, Das has been observing persuasive population control programmes, advising the government and is also part of various national and international networks, including the National Alliance on Maternal Health and Human Rights, Healthwatch Forum and MenEngage, a global alliance on men and gender equality.
The 2012-13 survey also shows indicators that define the "quality of family planning services" remain abysmally low. Most women are unaware of other means of contraception and the known side-effects of sterilisation. Even when they are counselled, the counselling is manipulative as the staff has already decided which contraceptive method a woman needs. In Maharashtra, only 17 percent of the women were told about the side-effects, while the figure was 14 percent in Punjab and 11 percent in Andhra Pradesh and Haryana. According to the District Level Household & Facility Survey 2007-08, 40 percent of the women who underwent tubectomy in public health facilities across India were illiterate, indicating that tubectomy was not the "chosen" form of contraception.
Despite the problems associated with tubectomies, state governments continue to set targets for sterilisation surgeries. The reply to an RTI query showed that around 1,000 women were targeted for tubectomy in just west Delhi over the months of January, February and March this year.
The two extremes of the debate on how to stabilise the population are represented by the coercive sterilisation drive associated with Indira Gandhi's son Sanjay Gandhi during the Emergency, on the one hand, and senior Congress politician Karan Singh's statement at the 1974 World Population Conference in Bucharest, Romania, that "development is the best contraceptive", on the other. For a long time, the dominant thinking globally was in favour of coercive policies.
Internationally, this debate came to rest at the International Conference on Population and Development 1994 (ICPD 94) in Cairo, Egypt. At ICPD 94, civil society activists from around the world shared experiences of coercive population policies and convinced 179 national governments to see "population" as people, not a number. Economists like Amartya Sen had also proved by then that improvements in women's education and healthcare automatically result in smaller families without any need for authoritative population control policies.
ICPD 94 brought about a "paradigm shift". The governments agreed to abide by reproductive rights and honour gender equality while providing universal access to family planning, sexual and reproductive health services. The Indian government, too, grudgingly committed to place individuals at the centre of development. However, the state governments in India by and large do not follow this principle in practice and it is not uncommon for politicians, bureaucrats, judges and the educated, urban middle class to blame India's large population for nearly all the problems plaguing the country and favour force over cooperation.
Until ICPD 94, population was considered a dirty word - a dangerous "bomb" that would explode if not controlled. In the early 1950s, more babies were surviving in the newly-independent countries and fewer children were being born in the richer countries, leading to a fear of "overpopulation" in the Global South. This led to the formation in 1952 of two NGOs - the Population Council and the International Planned Parenthood Federation (IPPF) - in New York and Bombay, respectively. They were set up with the purpose of influencing the US government to orient the US Agency for International Development (USAID) towards population control in the Third World, alerting Americans to the danger of population "explosion" and raising funds for international birth control programmes.
An advertisement for a joint campaign by the two NGOs read: "A world of mass starvation in underdeveloped countries will be a world of chaos, riots and war. And a perfect breeding ground for communism... Our own national interests demand that we go all out to help the underdeveloped countries control their populations."
The political agenda was reinforced and validated by Stanford University Professor Paul R Ehrlich, who authored The Population Bomb in 1968. He emphasised birth control at any cost with the use of contraceptives, mass sterilisation and pre-natal sex determination (so that parents can design the family sex composition). The US government was soon convinced. In 1974, National Security Study Memorandum 200 of the National Security Council asserted that population growth in poor countries posed a problem for the security of the US. That is how the US and other industrialised countries, which had achieved lower birth rates due to improvements in education, healthcare and incomes, without any coercive population control policies, became the biggest proponents of the latter.
India could not remain unaffected by the discourse. In 1970, JRD Tata formed the Population Foundation of India with money from the Ford Foundation for population control advocacy in India. While the country's population initially focussed on vasectomy of men and stayed clear of female sterilisation, considering the risk of infection, the tide had turned by the 1980s. The infamous coercive male sterilisation drives of the Emergency period gave way to the setting of targets for female sterilisation, which continues to dominate the population control policy.
In 1992, a study by Dr Rani Bang and Dr Abhay Bang demonstrated that women had more faith in indigenous methods of contraception than the modern ones because they commonly associated the latter with adverse effects such as backache, abdominal pain, weakness and irregular or excessive menstruation. Women also found that healthcare professionals were often insensitive to these complaints and regarded them as minor and insignificant side-effects that should be ignored.
ICPD 94 was the culmination of the coming together of academics, activists and the medical community in efforts to propose an alternative perspective on population control policies. They showed how a policy of targets, incentives and disincentives under the National Family Planning Programme had made women mute recipients suffering quietly.
Among the participants at ICPD 94 was an IAS officer, AR Nanda, who was then the secretary at the Union Ministry of Health. After he returned from Cairo, he took up the mantle to reorient the population policy. The second half of the 1990s saw a new target-free approach, which focussed on combining contraception needs with providing reproductive and child health. Nanda also drafted the landmark National Population Policy (NPP) 2000, which stressed on improvements in human development, gender equality and reproductive health to stabilise population growth.
"In 1999, when I proposed the NPP, a few MPs supported the two pillars of the policy - informed choice and informed consent - but it was largely criticised in Parliament," says Nanda, who has since retired from the government, but continues to advise the National Coalition Against Two-Child Norm, an advocacy group of NGOs, academics and activists concerned with promoting policies that empower people to exercise their reproductive rights and choice.
The NPP 2000 begins with a statement that "the overriding objective of economic and social development is to improve (the) quality of life that people lead, to enhance their well-being and to provide them with opportunities and choices to become productive assets in society". The policy recommended the empowerment of women through enhanced access to education, employment opportunities and quality healthcare.
The policy, however, failed to influence a large section of politicians who continued to see population as a problem. In May 2000, when India's population crossed the one-billion mark, the then prime minister Atal Bihari Vajpayee said: "This is a serious matter that is both cause for concern and introspection - concern over the impact that a runaway population growth is bound to have on the nation's economic, natural and other resources; introspection over where we went wrong and how we can stabilise our population... If the present growth rate of our population remains unchecked, India will become the world's most populous country by the middle of this century, with people clamouring for a share of shrinking natural resources."
Opposition to NPP 2000 continued even after it was adopted. Population being a subject on the Concurrent List, the state governments are not obliged to follow anything that the Centre prescribes on population control. They have their own policies that in most cases go against NPP 2000. For instance, Uttar Pradesh introduced contraceptives such as injectables and implants, which are proven to be unsafe for women; Rajasthan promoted a lottery scheme for those who opt for sterilisation; and Bihar contracted out tubectomy surgeries to private operators and NGOs.
"The language used in talking about population stabilisation changed after ICPD 94 but the mindset remained more or less the same," says Nanda. "Even at the national level, male responsibility and gender equity were largely ignored. The state governments favour setting of targets and promoting terminal methods because the results are easy to measure."
Clearly, despite all the talk of empowering women, their reproductive autonomy - the right to choose whether to have children or not and the freedom to choose the methods of fertility management based on access to proper information - has been largely ignored in the policies and practices promoted by various governments in India.
Unfortunately, India has seen a reduced prevalence of condom use with women remaining unequal targets of the family planning burden. As the dominant, irreversible methods of population control take a toll on women's health, there is indeed a need for reorienting it towards the promotion of temporary and reversible methods such as condoms, which also provide a barrier against sexually transmitted diseases.
--
The downside of contraception
Disadvantages and side-effects of various contraceptive methods
Oral Contraceptive Pill: Nausea, mild headaches, tender breasts, spotting between periods, irregular bleeding, moodiness, vomiting within two hours of taking a pill, severe diarrhoea and vomiting for more than 24 hours
Copper-bearing IUDs: Menstrual changes in early months, longer and heavy menstrual periods, bleeding or spotting between periods, more cramps or pain during period. Uncommon sideeffects include severe cramps and pain beyond first three-five days of insertion, heavy menstrual bleeding or bleeding between periods, possibly contributing to anaemia and possibility of perforation if not inserted properly. It does not protect against sexually transmitted diseases (STDs) including HIV/AIDs. Medical procedure, including pelvic examination, is needed to insert the IUD. Occasionally, a woman faints during the insertion procedure. A trained healthcare provider must remove the IUD. The IUD may come out of the uterus possibly without the woman knowing about it (more common when the IUD is inserted soon after childbirth)
Vasectomy: Uncomfortable for two or three days, pain in scrotum, swelling and bruising and brief feeling of faintness after the procedure. Rare complications of surgery include bleeding or infection at the incision site or inside the incision, blood clots in the scrotum. No protection against STDs, including HIV/AIDs
Tubectomy: Uncommon complications include infection or bleeding at the incision, internal infection or bleeding, injury to internal organs and anaesthesia risk. No protection against STDs
Male Condom: Latex condoms may cause itching for a few people who are allergic to latex. Also, some people may be allergic to the lubricant on some brands of condoms. Small possibility that condom might slip off or break during sexual intercourse
 Published on Oct 7, 2014
Published on Oct 7, 2014
 Modified on Oct 7, 2014
Modified on Oct 7, 2014
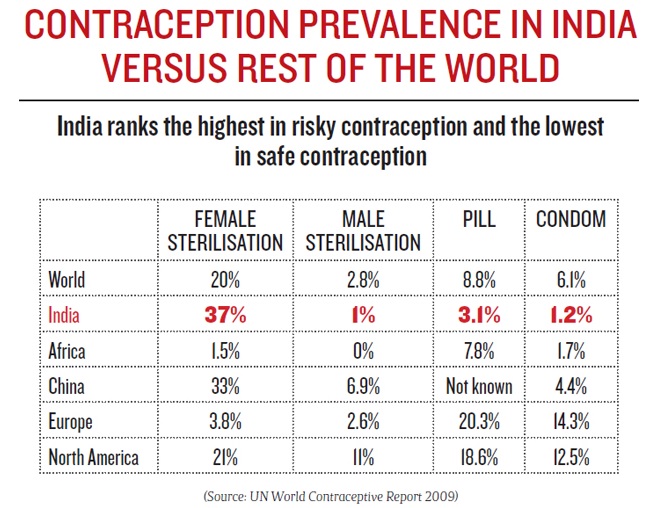









Write Comments