Deprecated (16384): The ArrayAccess methods will be removed in 4.0.0.Use getParam(), getData() and getQuery() instead. - /home/brlfuser/public_html/src/Controller/ArtileDetailController.php, line: 150
You can disable deprecation warnings by setting `Error.errorLevel` to `E_ALL & ~E_USER_DEPRECATED` in your config/app.php. [CORE/src/Core/functions.php, line 311]
deprecationWarning - CORE/src/Core/functions.php, line 311
Cake\Http\ServerRequest::offsetGet() - CORE/src/Http/ServerRequest.php, line 2421
App\Controller\ArtileDetailController::index() - APP/Controller/ArtileDetailController.php, line 150
Cake\Controller\Controller::invokeAction() - CORE/src/Controller/Controller.php, line 610
Cake\Http\ActionDispatcher::_invoke() - CORE/src/Http/ActionDispatcher.php, line 120
Cake\Http\ActionDispatcher::dispatch() - CORE/src/Http/ActionDispatcher.php, line 94
Cake\Http\BaseApplication::__invoke() - CORE/src/Http/BaseApplication.php, line 235
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Routing\Middleware\RoutingMiddleware::__invoke() - CORE/src/Routing/Middleware/RoutingMiddleware.php, line 162
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Routing\Middleware\AssetMiddleware::__invoke() - CORE/src/Routing/Middleware/AssetMiddleware.php, line 97
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Error\Middleware\ErrorHandlerMiddleware::__invoke() - CORE/src/Error/Middleware/ErrorHandlerMiddleware.php, line 96
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Http\Runner::run() - CORE/src/Http/Runner.php, line 51
Cake\Http\Server::run() - CORE/src/Http/Server.php, line 98
Deprecated (16384): The ArrayAccess methods will be removed in 4.0.0.Use getParam(), getData() and getQuery() instead. - /home/brlfuser/public_html/src/Controller/ArtileDetailController.php, line: 151
You can disable deprecation warnings by setting `Error.errorLevel` to `E_ALL & ~E_USER_DEPRECATED` in your config/app.php. [CORE/src/Core/functions.php, line 311]
deprecationWarning - CORE/src/Core/functions.php, line 311
Cake\Http\ServerRequest::offsetGet() - CORE/src/Http/ServerRequest.php, line 2421
App\Controller\ArtileDetailController::index() - APP/Controller/ArtileDetailController.php, line 151
Cake\Controller\Controller::invokeAction() - CORE/src/Controller/Controller.php, line 610
Cake\Http\ActionDispatcher::_invoke() - CORE/src/Http/ActionDispatcher.php, line 120
Cake\Http\ActionDispatcher::dispatch() - CORE/src/Http/ActionDispatcher.php, line 94
Cake\Http\BaseApplication::__invoke() - CORE/src/Http/BaseApplication.php, line 235
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Routing\Middleware\RoutingMiddleware::__invoke() - CORE/src/Routing/Middleware/RoutingMiddleware.php, line 162
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Routing\Middleware\AssetMiddleware::__invoke() - CORE/src/Routing/Middleware/AssetMiddleware.php, line 97
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Error\Middleware\ErrorHandlerMiddleware::__invoke() - CORE/src/Error/Middleware/ErrorHandlerMiddleware.php, line 96
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Http\Runner::run() - CORE/src/Http/Runner.php, line 51
Cake\Http\Server::run() - CORE/src/Http/Server.php, line 98
Warning (512): Unable to emit headers. Headers sent in file=/home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php line=853 [CORE/src/Http/ResponseEmitter.php, line 48]
if (Configure::read('debug')) {
trigger_error($message, E_USER_WARNING);
} else {
$response = object(Cake\Http\Response) {
'status' => (int) 200,
'contentType' => 'text/html',
'headers' => [
'Content-Type' => [
[maximum depth reached]
]
],
'file' => null,
'fileRange' => [],
'cookies' => object(Cake\Http\Cookie\CookieCollection) {},
'cacheDirectives' => [],
'body' => '<!DOCTYPE html>
<!--[if lt IE 7 ]>
<html class="ie ie6" lang='en'> <![endif]-->
<!--[if IE 7 ]>
<html class="ie ie7" lang='en'> <![endif]-->
<!--[if IE 8 ]>
<html class="ie ie8" lang='en'> <![endif]-->
<!--[if (gte IE 9)|!(IE)]><!-->
<html lang='en'>
<!--<![endif]-->
<head><meta http-equiv="Content-Type" content="text/html; charset=utf-8">
<title>
LATEST NEWS UPDATES | Question of efficacy -Leena Menghaney </title>
<meta name="description" content="
The country is clearly shaping its legislation to promote access to medicines by fostering generic production.
INDIA'S approach to the revision of its Patents Act in 2005 is a clear example of a country shaping its legislation to promote access..."/>
<meta name="keywords" content="Health,patents,medicines"/>
<meta name="news_keywords" content="Health,patents,medicines">
<link rel="alternate" type="application/rss+xml" title="ROR" href="/ror.xml"/>
<link rel="alternate" type="application/rss+xml" title="RSS 2.0" href="/feeds/"/>
<link rel="stylesheet" href="/css/bootstrap.min.css?1697864993"/> <link rel="stylesheet" href="/css/style.css?v=1.1.2"/> <link rel="stylesheet" href="/css/style-inner.css?1577045210"/> <link rel="stylesheet" id="Oswald-css"
href="https://fonts.googleapis.com/css?family=Oswald%3Aregular%2C700&ver=3.8.1" type="text/css"
media="all">
<link rel="stylesheet" href="/css/jquery.modal.min.css?1578285302"/> <script src="/js/jquery-1.10.2.js?1575549704"></script> <script src="/js/jquery-migrate.min.js?1575549704"></script> <link rel="shortcut icon" href="/favicon.ico" title="Favicon">
<link rel="stylesheet" href="/css/jquery-ui.css?1580720609"/> <script src="/js/jquery-ui.js?1575549704"></script> <link rel="preload" as="style" href="https://www.im4change.org/css/custom.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery.modal.min.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery-ui.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/li-scroller.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<!-- <link rel="preload" as="style" href="https://www.im4change.org/css/style.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous"> -->
<link rel="preload" as="style" href="https://www.im4change.org/css/style-inner.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel='dns-prefetch' href="//im4change.org/css/custom.css" crossorigin >
<link rel="preload" as="script" href="https://www.im4change.org/js/bootstrap.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.li-scroller.1.0.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.modal.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.ui.totop.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-1.10.2.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-migrate.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-ui.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/setting.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/tie-scripts.js">
<!--[if IE]>
<script type="text/javascript">jQuery(document).ready(function () {
jQuery(".menu-item").has("ul").children("a").attr("aria-haspopup", "true");
});</script>
<![endif]-->
<!--[if lt IE 9]>
<script src="/js/html5.js"></script>
<script src="/js/selectivizr-min.js"></script>
<![endif]-->
<!--[if IE 8]>
<link rel="stylesheet" type="text/css" media="all" href="/css/ie8.css"/>
<![endif]-->
<meta property="og:title" content="LATEST NEWS UPDATES | Question of efficacy -Leena Menghaney" />
<meta property="og:url" content="https://im4change.in/latest-news-updates/question-of-efficacy-leena-menghaney-14576.html" />
<meta property="og:type" content="article" />
<meta property="og:description" content="
The country is clearly shaping its legislation to promote access to medicines by fostering generic production.
INDIA'S approach to the revision of its Patents Act in 2005 is a clear example of a country shaping its legislation to promote access..." />
<meta property="og:image" content="" />
<meta property="fb:app_id" content="0" />
<meta name="viewport" content="width=device-width, initial-scale=1, maximum-scale=1, user-scalable=no">
<link rel="apple-touch-icon-precomposed" sizes="144x144" href="https://im4change.in/images/apple1.png">
<link rel="apple-touch-icon-precomposed" sizes="120x120" href="https://im4change.in/images/apple2.png">
<link rel="apple-touch-icon-precomposed" sizes="72x72" href="https://im4change.in/images/apple3.png">
<link rel="apple-touch-icon-precomposed" href="https://im4change.in/images/apple4.png">
<style>
.gsc-results-wrapper-overlay{
top: 38% !important;
height: 50% !important;
}
.gsc-search-button-v2{
border-color: #035588 !important;
background-color: #035588 !important;
}
.gsib_a{
height: 30px !important;
padding: 2px 8px 1px 6px !important;
}
.gsc-search-button-v2{
height: 41px !important;
}
input.gsc-input{
background: none !important;
}
@media only screen and (max-width: 600px) {
.gsc-results-wrapper-overlay{
top: 11% !important;
width: 87% !important;
left: 9% !important;
height: 43% !important;
}
.gsc-search-button-v2{
padding: 10px 10px !important;
}
.gsc-input-box{
height: 28px !important;
}
/* .gsib_a {
padding: 0px 9px 4px 9px !important;
}*/
}
@media only screen and (min-width: 1200px) and (max-width: 1920px) {
table.gsc-search-box{
width: 15% !important;
float: right !important;
margin-top: -118px !important;
}
.gsc-search-button-v2 {
padding: 6px !important;
}
}
</style>
<script>
$(function () {
$("#accordion").accordion({
event: "click hoverintent"
});
});
/*
* hoverIntent | Copyright 2011 Brian Cherne
* http://cherne.net/brian/resources/jquery.hoverIntent.html
* modified by the jQuery UI team
*/
$.event.special.hoverintent = {
setup: function () {
$(this).bind("mouseover", jQuery.event.special.hoverintent.handler);
},
teardown: function () {
$(this).unbind("mouseover", jQuery.event.special.hoverintent.handler);
},
handler: function (event) {
var currentX, currentY, timeout,
args = arguments,
target = $(event.target),
previousX = event.pageX,
previousY = event.pageY;
function track(event) {
currentX = event.pageX;
currentY = event.pageY;
}
;
function clear() {
target
.unbind("mousemove", track)
.unbind("mouseout", clear);
clearTimeout(timeout);
}
function handler() {
var prop,
orig = event;
if ((Math.abs(previousX - currentX) +
Math.abs(previousY - currentY)) < 7) {
clear();
event = $.Event("hoverintent");
for (prop in orig) {
if (!(prop in event)) {
event[prop] = orig[prop];
}
}
// Prevent accessing the original event since the new event
// is fired asynchronously and the old event is no longer
// usable (#6028)
delete event.originalEvent;
target.trigger(event);
} else {
previousX = currentX;
previousY = currentY;
timeout = setTimeout(handler, 100);
}
}
timeout = setTimeout(handler, 100);
target.bind({
mousemove: track,
mouseout: clear
});
}
};
</script>
<script type="text/javascript">
var _gaq = _gaq || [];
_gaq.push(['_setAccount', 'UA-472075-3']);
_gaq.push(['_trackPageview']);
(function () {
var ga = document.createElement('script');
ga.type = 'text/javascript';
ga.async = true;
ga.src = ('https:' == document.location.protocol ? 'https://ssl' : 'http://www') + '.google-analytics.com/ga.js';
var s = document.getElementsByTagName('script')[0];
s.parentNode.insertBefore(ga, s);
})();
</script>
<link rel="stylesheet" href="/css/custom.css?v=1.16"/> <script src="/js/jquery.ui.totop.js?1575549704"></script> <script src="/js/setting.js?1575549704"></script> <link rel="manifest" href="/manifest.json">
<meta name="theme-color" content="#616163" />
<meta name="apple-mobile-web-app-capable" content="yes">
<meta name="apple-mobile-web-app-status-bar-style" content="black">
<meta name="apple-mobile-web-app-title" content="im4change">
<link rel="apple-touch-icon" href="/icons/logo-192x192.png">
</head>
<body id="top" class="home inner blog">
<div class="background-cover"></div>
<div class="wrapper animated">
<header id="theme-header" class="header_inner" style="position: relative;">
<div class="logo inner_logo" style="left:20px !important">
<a title="Home" href="https://im4change.in/">
<img src="https://im4change.in/images/logo2.jpg?1582080632" class="logo_image" alt="im4change"/> </a>
</div>
<div class="langhindi" style="color: #000;display:none;"
href="https://im4change.in/">
<a class="more-link" href="https://im4change.in/">Home</a>
<a href="https://im4change.in/hindi/" class="langbutton ">हिन्दी</a>
</div>
<nav class="fade-in animated2" id="main-nav">
<div class="container">
<div class="main-menu">
<ul class="menu" id="menu-main">
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
style="left: -40px;"><a
target="_blank" href="https://im4change.in/">Home</a>
</li>
<li class="menu-item mega-menu menu-item-type-taxonomy mega-menu menu-item-object-category mega-menu menu-item-has-children parent-list"
style=" margin-left: -40px;"><a href="#">KNOWLEDGE GATEWAY <span class="sub-indicator"></span>
</a>
<div class="mega-menu-block background_menu" style="padding-top:25px;">
<div class="container">
<div class="mega-menu-content">
<div class="mega-menu-item">
<h3><b>Farm Crisis</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/farmers039-suicides-14.html"
class="left postionrel">Farm Suicides </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/unemployment-30.html"
class="left postionrel">Unemployment </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/rural-distress-70.html"
class="left postionrel">Rural distress </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/migration-34.html"
class="left postionrel">Migration </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/key-facts-72.html"
class="left postionrel">Key Facts </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/debt-trap-15.html"
class="left postionrel">Debt Trap </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Empowerment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/union-budget-73.html"
class="left postionrel">Union Budget And Other Economic Policies </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/forest-and-tribal-rights-61.html"
class="left postionrel">Forest and Tribal Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-education-60.html"
class="left postionrel">Right to Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-food-59.html"
class="left postionrel">Right to Food </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/displacement-3279.html"
class="left postionrel">Displacement </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-work-mg-nrega-39.html"
class="left postionrel">Right to Work (MG-NREGA) </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/gender-3280.html"
class="left postionrel">GENDER </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-information-58.html"
class="left postionrel">Right to Information </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/social-audit-48.html"
class="left postionrel">Social Audit </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Hunger / HDI</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/poverty-and-inequality-20499.html"
class="left postionrel">Poverty and inequality </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/malnutrition-41.html"
class="left postionrel">Malnutrition </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/public-health-51.html"
class="left postionrel">Public Health </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/education-50.html"
class="left postionrel">Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hunger-overview-40.html"
class="left postionrel">Hunger Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hdi-overview-45.html"
class="left postionrel">HDI Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/pds-ration-food-security-42.html"
class="left postionrel">PDS/ Ration/ Food Security </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/sdgs-113.html"
class="left postionrel">SDGs </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/mid-day-meal-scheme-mdms-53.html"
class="left postionrel">Mid Day Meal Scheme (MDMS) </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Environment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/time-bomb-ticking-52.html"
class="left postionrel">Time Bomb Ticking </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/water-and-sanitation-55.html"
class="left postionrel">Water and Sanitation </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/impact-on-agriculture-54.html"
class="left postionrel">Impact on Agriculture </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Law & Justice</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/social-justice-20500.html"
class="left postionrel">Social Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/access-to-justice-47.html"
class="left postionrel">Access to Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/human-rights-56.html"
class="left postionrel">Human Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/corruption-35.html"
class="left postionrel">Corruption </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/general-insecurity-46.html"
class="left postionrel">General Insecurity </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/disaster-relief-49.html"
class="left postionrel">Disaster & Relief </a>
</p>
</div>
</div>
</div>
</div>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page "><a target="_blank" href="https://im4change.in/nceus_reports.php">NCEUS reports</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children parent-list ">
<a target="_blank" href="https://im4change.in/about-us-9.html">About Us <span
class="sub-indicator"></span></a>
<ul class="sub-menu aboutmenu">
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/objectives-8.html">Objectives</a>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/contactus.php">Contact
Us</a></li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/about-us-9.html">About
Us</a></li>
</ul>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children ">
<a target="_blank" href="https://im4change.in/fellowships.php" title="Fellowships">Fellowships</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/media-workshops.php">Workshops</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/research.php">Research</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/links-64">Partners</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
id="menu-item-539"><a target="_blank" href="https://im4change.in/hindi/"
class="langbutton langlinkfont17">हिन्दी</a></li>
</ul>
</div> </div>
<!-- <div style="float: right;">
<script async src="https://cse.google.com/cse.js?cx=18b4f2e0f11bed3dd"></script>
<div class="gcse-search"></div>
</div> -->
<div class="search-block" style=" margin-left: 8px; margin-right: 7px;">
<form method="get" id="searchform" name="searchform"
action="https://im4change.in/search"
onsubmit="return searchvalidate();">
<button class="search-button" type="submit" value="Search"></button>
<input type="text" id="s" name="qryStr" value=""
onfocus="if (this.value == 'Search...') {this.value = '';}"
onblur="if (this.value == '') {this.value = 'Search...';}">
</form>
</div>
</nav>
</header>
<div class="container">
<div id="main-content" class=" main1 container fade-in animated3 sidebar-narrow-left">
<div class="content-wrap">
<div class="content" style="width: 900px;min-height: 500px;">
<section class="cat-box recent-box innerCatRecent">
<h1 class="cat-box-title">Question of efficacy -Leena Menghaney</h1>
<a href="JavaScript:void(0);" onclick="return shareArticle(14452);">
<img src="https://im4change.in/images/email.png?1582080630" border="0" width="24" align="right" alt="Share this article"/> </a>
<a href="https://im4change.in/latest-news-updates/question-of-efficacy-leena-menghaney-14576/print"
rel="nofollow">
<img src="https://im4change.in/images/icon-print.png?1582080630" border="0" width="24" align="right" alt="Share this article"/>
</a>
</section>
<section class="recent-box innerCatRecent">
<small class="pb-1"><span class="dateIcn">
<img src="https://im4change.in/images/published.svg?1582080666" alt="published"/>
Published on</span><span class="text-date"> Apr 20, 2012</span>
<span
class="dateIcn">
<img src="https://im4change.in/images/modified.svg?1582080666" alt="modified"/> Modified on </span><span class="text-date"> Apr 20, 2012</span>
</small>
</section>
<div class="clear"></div>
<div style="padding-top: 10px;">
<div class="innerLineHeight">
<div class="middleContent innerInput latest-news-updates">
<table>
<tr>
<td>
<div>
<br /><div align="justify"><em>The country is clearly shaping its legislation to promote access to medicines by fostering generic production. <br /></em><img src="https://im4change.in/siteadmin/tinymce/uploaded/Patent 1.bmp" alt="Patent 1" /><br />INDIA'S approach to the revision of its Patents Act in 2005 is a clear example of a country shaping its legislation to promote access to medicines by fostering generic production. Although World Trade Organisation (WTO) rules made it mandatory for India to put in place a patent regime for medicines by 2005, nothing obliges developing countries such as India to replicate the patent system of wealthy countries, which involves charging the highest possible price and protecting that price through patent monopolies that extend way beyond 20 years.<br /><br />India has used important flexibilities under international law to include provisions in its domestic patent law not only to reduce the number of secondary patents but also to have a licensing mechanism that kicks in with excessive pricing of patented medicines. The application of these safeguards by the Indian patent office – benefiting patients in India and other developing countries – is increasingly inviting the ire of the multinational pharmaceutical industry and its associations.<br /><br />The Indian government is faced with court cases and the diplomatic offensive that the protectors of the pharmaceutical industry in the United States and the European Union are now launching.<br /><br />In India, the importance of generic (local) production of medicines in fostering competition and reducing prices was first recognised by lawmakers in the Patents Act of 1970, which brought in a legal regime that did not allow product patents on pharmaceuticals. In the following decades, India not only was successful in making drugs affordable but also significantly increased their availability by building domestic capacity to produce essential and life-saving drugs. It also went on to become the “pharmacy of the developing world”, supplying medicines to countries that lacked the capacity and resources to produce the drugs themselves or pay the high prices demanded by originator pharmaceutical companies.<br /><br />The production of more affordable generic medicines in India has been instrumental in driving down the price of AIDS (acquired immune deficiency syndrome) medicines by 99 per cent, and nearly six million people living with HIV have been put on treatment on Indian generic medicines in the past 10 years.<br /><br />In 2005, India was obliged to change its patent law in order to comply with its obligations as a member of the WTO, bringing into effect the TRIPS Agreement. The most significant change was the introduction of product patents for medicines. When framing the new patent legislation in 2005, Parliament sought to ensure that provisions to protect public health and access to medicines were incorporated into it. It, therefore, included explicit legal safeguards and guidance on how the patentability requirements should be applied.<br /><br />In particular, evergreening, a well-known abuse of the patent system where companies seek new monopolies or, alternatively, extend a monopoly by seeking to patent minor changes – such as new uses, new forms and other routine improvements of known medicines – was addressed. Section 3(d) of the Indian Patents Act explicitly allows the broad exclusion from patentability of new uses and new forms of known medicines. In sum, Section 3(d) gave explicit guidance to the Indian patent office on how to weed out patent claims on routine improvements of known medicines and protect the country's capacity to act as a factory for the production and supply of affordable generic medicines.<br /></div><div align="justify"> </div><div align="justify"><em>Legal challenge<br /></em><br />In 2006, in a landmark decision, the Indian patent office rejected Swiss pharmaceutical company Novartis' patent application for the life-saving anti-cancer drug imatinib mesylate. The application for a patent on a beta crystalline salt form of imatinib was rejected on the grounds that it lacked novelty, was obvious, and was un-patentable under Section 3(d) of the Patents Act. In retaliation, Novartis mounted a legal challenge to have Section 3(d) declared unconstitutional. Medecins Sans Frontieres (MSF) launched an international campaign calling on the company to drop the case, attracting close to half a million signatures. In 2007, the Madras High Court rejected Novartis' plea and in 2009 the Intellectual Property Appellate Board (IPAB) rejected its patent application on imatinib mesylate once again.<br /><img src="https://im4change.in/siteadmin/tinymce/uploaded/Patent 2.bmp" alt="Patent 2" /><br />But the company is not backing down. After failing to have Section 3(d) struck down, it is now again seeking to limit its effect. In 2009, Novartis filed a special leave petition in the Supreme Court against India in relation to the patentability criteria to be applied to imatinib mesylate.<br /><br />Under Section 3(d) of the Patents Act, new forms of already known substances cannot be patented if they fail to demonstrate the required degree of efficacy; it requires demonstration of increased efficacy for a medicine to deserve a patent. The interpretation of the definition of “efficacy” is therefore central to this case and to the future of India's role as the pharmacy of the developing world.<br /><br />In 2007, in its constitutional challenge against Section 3(d) before the Madras High Court, Novartis had argued that increased bioavailability of the salt form of imatinib meant increased efficacy, entitling it to a patent. But the High Court clarified that efficacy meant “therapeutic effect in healing a disease”.<br /><br />The IPAB, where appeals for unsuccessful patent applications are heard, subsequently applied this interpretation and held that the salt form of imatinib mesylate did not meet the test of therapeutic efficacy. It, therefore, confirmed the rejection of Novartis's patent application.<br /></div><div align="justify"> </div><div align="justify"><em>High standards crucial for tests in patent law<br /></em><br />Setting high standards for the various tests in the patent legislation, particularly the “efficacy” test of Section 3(d) and the inventive step requirement, leading to fewer patents on new forms of known medicines, is important to safeguard access to affordable generic medicines from India. Novartis has now taken its case to the Supreme Court to argue against the interpretation of “efficacy” in Section 3(d) by the Madras High Court and the IPAB. This case has the potential to severely affect access to affordable essential medicines for millions of people across the developing world. It will determine whether Section 3(d) will continue to ensure that patents are granted only on medicines that are truly new and inventive. Many developing countries rely on affordable medicines produced in India, and such medicines constitute over 80 per cent of the AIDS drugs used in the developing world. MSF is closely following the outcome of this case.<br /><br />Novartis is basing its claim for a patent on the salt of imatinib on the fact that there is a 30 per cent increase in the bioavailability of the drug in this new form. But, according to the guidelines for the examination of pharmaceutical patents developed by the World Health Organisation (WHO) and the International Centre for Trade and Sustainable Development (ICTSD), the selection of a salt of the active ingredient with the purpose to improve bioavailability is known in pharmaceutical science. It is common knowledge in the field that salts result in different solubility and, therefore, in different bioavailability.<br /><br />The final arguments in the case have started. The next date of hearing is set for July 10. If Novartis wins, many other medicines, even those that show no increased therapeutic efficacy, will be patentable in India, and the availability of affordable medicines will be threatened. If the substance is taken out of Section 3(d), abusive “evergreening” practices, where drug companies maintain artificially high prices on medicines well beyond the original patent period by securing fresh patents on minor modifications of existing drugs, will become rampant in the future.<br /><br />If, on the other hand, the high threshold for patentability is upheld, generic production will continue to drive the price of life-saving medicines down. Multinational pharmaceutical companies such as Novartis will find it difficult to argue that routine improvements – such as new forms of existing medicines that result in improved stability, enhanced bioavailability, increased solubility, improved flow properties and lower hygroscopicity – meet the efficacy requirements of Section 3(d). In addition, the improved therapeutic efficacy would have to be supported with actual clinical data that demonstrate this effect.<br /><br />The Supreme Court case is the final act in a legal battle that stretches back over six years between Novartis and the Indian government. The government, hopefully, will argue for a strict interpretation of “efficacy” so that patents on new forms of known medicines – such as the one on the cancer drug imatinib mesylate – are not granted as a matter of routine by the country's patent office. Novartis has lined up very senior and very expensive lawyers, including two former Solicitors General, to argue its case. But there appears to be no information on whether the government has appointed its own top lawyer, the Attorney General, in this case.<br /></div><div align="justify"> </div><div align="justify"><em>Opening the door for compulsory licensing<br /></em><br />In another test case on access to treatment, seven years after India revised its 1970 Patents Act, the Controller General of Patents issued the first-ever compulsory licence (CL) to the Hyderabad-based company Natco to produce an affordable version of a patented anti-cancer medicine (sorafenib tosylate) of the German pharmaceutical company Bayer Corporation, marketed under the brand name of Nexavar. The generic version produced by Natco, which will pay 6 per cent royalty on net sales to Bayer, will be 97 per cent cheaper.<br /><br />The decision was made on the basis of the fact that not only had the patentee, Bayer, failed to price sorafenib tosylate at a level that made it accessible and affordable but it was also unable to ensure that the medicine was available in sufficient and sustainable quantities within India. Bayer has time until mid-June to appeal against the order.<br /><br />Like many other giant drug companies, Bayer defended the inflated cost of sorafenib by specifying the high spending on research and development. However, what it did not highlight was that the United States National Institutes of Health had sponsored almost 70 per cent of the second phase of its clinical trials. Later, this drug was given an “orphan drug” designation by the U.S.' Food and Drug Administration (FDA) for the treatment of renal cell carcinoma, entitling Bayer to 50 per cent tax credits, which further lowered the company's costs for the third and most expensive phase of clinical trials.<br /><br />The CL is quickly being dubbed by pharmaceutical companies such as Novartis as a move that will stifle innovation. Indeed, pharmaceutical companies at present try to recover their investments by charging excessively high prices and protecting their drugs through patent monopolies. However, R&D costs are only a fraction of the profits thus made, and a large part of the profits are spent on brand-building and marketing. In 2011, Bayer spent nearly €9 billion on sales and advertising. In the same period, only €2.9 billion was spent on research.<br /><br />The patent system also has another drawback. Innovation currently fails to address the needs of patients in developing countries.<br /><br />The drug companies also repeatedly warn that measures such as the CL adversely affect the confidence of foreign investors. But a study published in Thailand in 2009 by the Health Intervention and Technology Assessment Program (HITAP) found little evidence of a link between the granting of CLs and the level of foreign direct investment (FDI) in the country.<br /><br />The recently granted CL actually highlights a potentially new patent model that routinely allows low-cost alternatives in lieu of royalty payments, not only helping originators to recoup their development costs but also ensuring that people in developing countries have access to medicines. It is in line with licensing decisions in other jurisdictions. Recently, a U.S. court decided not to prevent a competitor from marketing a medical device used for skin grafts, and instead put in place a system of royalties from the competitor to the patent owner. At the core of this decision was the idea that the public has a right to access innovative health products and this should not be blocked by excessive prices.<br /><br />The Novartis and Bayer cases highlight that the country is entering a new era in which disputes on the public's access to and the affordability of drugs will become more frequent.<br /><br /><em>Leena Menghaney is campaign coordinator of Medecins Sans Frontieres in India and is based in New Delhi. </em><br /></div>
</div>
</td>
</tr>
</table>
</div>
</div>
</div>
<div class="clear"></div>
<br><a href="http://www.frontlineonnet.com/stories/20120504290802200.htm" class="re" target="_blank">Frontline, Volume 29, Issue 08, 21 April-04 May, 2012, http://www.frontlineonnet.com/stories/20120504290802200.htm</a><div class="clear"></div>
<div style="padding-top: 18px;">
<p class="post-tag">Tagged with:
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Health"
title="Health">
Health </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=patents"
title="patents">
patents </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=medicines"
title="medicines">
medicines </a>
</p>
</div>
<div class="clear"></div>
<br><br>
<div class="widget-top">
<h4>Related Articles</h4>
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<ul id="recentcomments">
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/fifth-report-from-gambia-implicates-indian-drug-maker-for-contaminated-syrups-banjot-kaur.html"
title="Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur">
Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-may-have-seen-steepest-dip-in-multidimensional-poverty-among-110-nations-as-per-undp-data-nikhil-rampal.html"
title="India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal">
India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/health-among-top-three-priorities-for-indian-voters-after-jobs-and-education-survey-shows-oliver-heath-jyoti-mishra-louise-tillin-sandhya-venkateswaran.html"
title="Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran">
Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/prevalence-of-zero-food-among-infants-and-young-children-in-india-patterns-of-change-across-the-states-and-union-territories-of-india-1993-2021-the-lancet.html"
title="Prevalence of Zero-Food among infants and young children in India - The Lancet ">
Prevalence of Zero-Food among infants and young children in India - The Lancet </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-s-sustainability-goals-at-risk-because-of-extreme-heatwaves-carbon-copy.html"
title="India's Sustainability Goals at Risk Because of Extreme Heatwaves - Carbon Copy">
India's Sustainability Goals at Risk Because of Extreme Heatwaves - Carbon Copy </a>
</li>
</ul>
</div>
<div class="comment-respond" id="respond">
<a name="commentbox"> </a>
<h3 class="comment-reply-title" id="reply-title">Write Comments</h3>
<form method="post" accept-charset="utf-8" role="form" action="/latest-news-updates/question-of-efficacy-leena-menghaney-14576.html"><div style="display:none;"><input type="hidden" name="_method" value="POST"/></div> <form class="comment-form" id="commentform" method="post" action="#commentbox" onSubmit="return validate()"
name="cmtform">
<input type="hidden" name="cmttype" value="articlecmt"/>
<input type="hidden" name="article_id" value="14452"/>
<p class="comment-notes">Your email address will not be published. Required fields are marked <span
class="required">*</span></p>
<p class="comment-form-author">
<label for="commenterName">Name</label>
<span class="required">*</span>
<input type="text" aria-required="true" size="30"
value=""
name="commenterName" id="commenterName" required="true">
</p>
<p class="comment-form-email">
<label for="commenterEmail">Email</label> <span class="required">*</span>
<input aria-required="true" size="30" name="commenterEmail" id="commenterEmail" type="email"
value=""
required="true">
</p>
<p class="comment-form-contact">
<label for="commenterPh">Contact No.</label>
<input type="text" size="30"
value=""
name="commenterPh" id="commenterPh">
</p>
<p class="comment-form-comment">
<label for="comment">Comment</label>
<textarea aria-required="true" required="true" rows="8" cols="45" name="comment"
id="comment"></textarea>
</p>
<p class="comment-form-comment">
<label for="comment">Type the characters you see in the image below <span class="required">*</span><br><img
class="captchaImg"
src="https://im4change.in/securimage_show_art.php?tk=2001382256" alt="captcha"/>
</label>
</p>
<input type="text" name="vrcode" required="true"/>
<p class="form-submit" style="width: 200px;">
<input type="submit" value="Post Comment" id="submit" name="submit">
</p></form>
</div>
<style>
.ui-widget-content {
height: auto !important;
}
</style>
<div id="share-modal"></div>
<style>
.middleContent a{
background-color: rgba(108,172,228,.2);
}
.middleContent a:hover{
background-color: #418fde;
border-color: #418fde;
color: #000;
}
</style>
<script>
function shareArticle(article_id) {
var options = {
modal: true,
height: 'auto',
width: 600 + 'px'
};
$('#share-modal').html("");
$('#share-modal').load('https://im4change.in/share_article?article_id=' + article_id).dialog(options).dialog('open');
}
function postShare() {
var param = 'article_id=' + $("#article_id").val();
param = param + '&y_name=' + $("#y_name").val();
param = param + '&y_email=' + $("#y_email").val();
param = param + '&f_name=' + $("#f_name").val();
param = param + '&f_email=' + $("#f_email").val();
param = param + '&y_msg=' + $("#y_msg").val();
$.ajax({
type: "POST",
url: 'https://im4change.in/post_share_article',
data: param,
success: function (response) {
$('#share-modal').html("Thank You, Your message posted to ");
}
});
return false;
}
</script> </div>
</div>
<!-- Right Side Section Start -->
<!-- MAP Section START -->
<aside class="sidebar indexMarg">
<div class="ad-cell">
<a href="https://im4change.in/statemap.php" title="">
<img src="https://im4change.in/images/map_new_version.png?1582080666" alt="India State Map" class="indiamap" width="232" height="252"/> </a>
<div class="rightmapbox">
<div id="sideOne" class="docltitle"><a href="https://im4change.in/state-report/india/36" target="_blank">DOCUMENTS/
REPORTS</a></div>
<div id="sideTwo" class="statetitle"><a href="https://im4change.in/states.php"target="_blank">STATE DATA/
HDRs.</a></div>
</div>
<div class="widget widgePadTop"></div>
</div>
</aside>
<!-- MAP Section END -->
<aside class="sidebar sidePadbottom">
<div class="rightsmlbox1" >
<a href="https://im4change.in/knowledge_gateway" target="_blank" style="color: #035588;
font-size: 17px;">
KNOWLEDGE GATEWAY
</a>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/newsletter" target="_blank">
NEWSLETTER
</a>
</p>
</div>
</div>
<div class="rightsmlbox1" style="height: 325px;">
<div>
<p class="rightsmlbox1_title">
Interview with Prof. Ravi Srivastava
</p>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/video/interview-with-prof-ravi-srivastava-on-current-economic-crisis">
<img width="250" height="200" src="/images/interview_video_home.jpg" alt="Interview with Prof. Ravi Srivastava"/>
</a>
<!--
<iframe width="250" height="200" src="https://www.youtube.com/embed/MmaTlntk-wc" frameborder="0" allow="accelerometer; autoplay; encrypted-media; gyroscope; picture-in-picture" allowfullscreen=""></iframe>-->
</p>
<a href="https://im4change.in/videogallery" class="more-link CatArchalAnch1" target="_blank">
More videos
</a>
</div>
</div>
<div class="rightsmlbox1">
<div>
<!--div id="sstory" class="rightboxicons"></div--->
<p class="rightsmlbox1_title"><a href="https://im4change.in/list-success-stories" target="_blank">Success Stories</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/interviews" target="_blank">Interviews</a>
</p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a href="https://www.commoncause.in/page.php?id=10" >Donate</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/marquee"
class="isf_link more-link" title="India Focus?" style="border: 4px solid #fdd922;width: 90%;background-color: #fdd922;text-align: center;color: #000000;font-size:18px" target="_blank">India Focus</a></p> </div>
</div>
<div class="rightsmlbox1" style="height: 104px !important;">
<a href="https://im4change.in/quarterly_reports.php" target="_blank">
Quarterly Reports on Effect of Economic Slowdown on Employment in India (2008 - 2015)
</a>
</div>
<!-- <div class="rightsmlbox1">
<a href="https://play.google.com/store/apps/details?id=com.im4.im4change" target="_blank">
</a></div> -->
<!-- <section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">Most Visited</h2>
</section> -->
<!-- accordion Starts here -->
<!-- <div id="accordion" class="accordMarg">
</div> -->
<!-- accordion ends here -->
<!-- Widget Tag Cloud Starts here -->
<div id="tag_cloud-2" class="widget widget_tag_cloud">
<section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">MOST VISITED TAGS</h2>
</section>
<div class="widget-top wiPdTp">
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<div class="tagcloud">
<a href="https://im4change.in/search?qryStr=Agriculture"
target="_blank" class="tag-link-4 font4">Agriculture</a>
<a href="https://im4change.in/search?qryStr=Food Security"
target="_blank" class="tag-link-4 font4">Food Security</a>
<a href="https://im4change.in/search?qryStr=Law and Justice"
target="_blank" class="tag-link-4 font4">Law and Justice</a>
<a href="https://im4change.in/search?qryStr=Health"
target="_blank" class="tag-link-4 font4">Health</a>
<a href="https://im4change.in/search?qryStr=Right to Food"
target="_blank" class="tag-link-4 font4">Right to Food</a>
<a href="https://im4change.in/search?qryStr=Corruption"
target="_blank" class="tag-link-4 font4">Corruption</a>
<a href="https://im4change.in/search?qryStr=farming"
target="_blank" class="tag-link-4 font4">farming</a>
<a href="https://im4change.in/search?qryStr=Environment"
target="_blank" class="tag-link-4 font4">Environment</a>
<a href="https://im4change.in/search?qryStr=Right to Information"
target="_blank" class="tag-link-4 font4">Right to Information</a>
<a href="https://im4change.in/search?qryStr=NREGS"
target="_blank" class="tag-link-4 font4">NREGS</a>
<a href="https://im4change.in/search?qryStr=Human Rights"
target="_blank" class="tag-link-4 font4">Human Rights</a>
<a href="https://im4change.in/search?qryStr=Governance"
target="_blank" class="tag-link-4 font4">Governance</a>
<a href="https://im4change.in/search?qryStr=PDS"
target="_blank" class="tag-link-4 font4">PDS</a>
<a href="https://im4change.in/search?qryStr=COVID-19"
target="_blank" class="tag-link-4 font4">COVID-19</a>
<a href="https://im4change.in/search?qryStr=Land Acquisition"
target="_blank" class="tag-link-4 font4">Land Acquisition</a>
<a href="https://im4change.in/search?qryStr=mgnrega"
target="_blank" class="tag-link-4 font4">mgnrega</a>
<a href="https://im4change.in/search?qryStr=Farmers"
target="_blank" class="tag-link-4 font4">Farmers</a>
<a href="https://im4change.in/search?qryStr=transparency"
target="_blank" class="tag-link-4 font4">transparency</a>
<a href="https://im4change.in/search?qryStr=Gender"
target="_blank" class="tag-link-4 font4">Gender</a>
<a href="https://im4change.in/search?qryStr=Poverty"
target="_blank" class="tag-link-4 font4">Poverty</a>
<a href="https://im4change.in/search?qryStr=Farm Laws" target="_blank" class="tag-link-4 font4">Farm Laws
</a>
<a href="https://im4change.in/search?qryStr=Citizenship Amendment Act" target="_blank" class="tag-link-4 font4">Citizenship Amendment Act
</a>
<a href="https://im4change.in/search?qryStr=CAA NPR NRIC" target="_blank" class="tag-link-4 font4">CAA NPR NRIC
</a>
<a href="https://im4change.in/search?qryStr=Job Losses" target="_blank" class="tag-link-4 font4">Job Losses
</a>
<a href="https://im4change.in/search?qryStr=Migrant Workers" target="_blank" class="tag-link-4 font4">Migrant Workers
</a>
<a href="https://im4change.in/search?qryStr=Unemployment" target="_blank" class="tag-link-4 font4">Unemployment
</a>
<a href="https://im4change.in/search?qryStr=PMGKAY" target="_blank" class="tag-link-4 font4">PMGKAY
</a>
<a href="https://im4change.in/search?qryStr=PM-KISAN" target="_blank" class="tag-link-4 font4">PM-KISAN
</a>
<a href="https://im4change.in/search?qryStr=PM-CARES" target="_blank" class="tag-link-4 font4">PM-CARES
</a>
<a href="https://im4change.in/search?qryStr=LFPR" target="_blank" class="tag-link-4 font4">LFPR
</a>
</div>
</div>
</div>
<!-- Widget Tag Cloud Ends here -->
</aside>
<!-- Right Side Section End -->
</div>
<section class="cat-box cats-review-box footerSec">
<h2 class="cat-box-title vSec CatArcha">Video
Archives</h2>
<h2 class="cat-box-title CatArchaTitle">Archives</h2>
<div class="cat-box-content">
<div class="reviews-cat">
<div class="CatArchaDiv1">
<div class="CatArchaDiv2">
<ul>
<li>
<a href="https://im4change.in/news-alerts-57/moving-upstream-luni-fellowship.html" target="_blank">
Moving Upstream: Luni – Fellowship </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/135-million-indians-exited-multidimensional-poverty-as-per-government-figures-is-that-the-same-as-poverty-reduction.html" target="_blank">
135 Million Indians Exited “Multidimensional" Poverty as per Government... </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/explainer-why-are-tomato-prices-on-fire.html" target="_blank">
Explainer: Why are Tomato Prices on Fire? </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/nsso-survey-only-39-1-of-all-households-have-drinking-water-within-dwelling-46-7-of-rural-households-use-firewood-for-cooking.html" target="_blank">
NSSO Survey: Only 39.1% of all Households have Drinking... </a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/news-alerts-57"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/I51LYnP8BOk/1.jpg"
alt=" Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Short-Video-on-im4change-Hindi-website-Inclusive-Media-for-Change" target="_blank">
Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/kNqha-SwfIY/1.jpg"
alt=" "Session 1: Scope of IDEA and AgriStack" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-1- Scope-of-IDEA-and-AgriStack-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 1: Scope of IDEA and AgriStack" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/6kIVjlgZItk/1.jpg"
alt=" "Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-2-Farmer-Centric-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/2BeHTu0y7xc/1.jpg"
alt=" "Session 3: Future of Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-3-Future-of-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 3: Future of Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="divWidth">
<ul class="divWidthMarg">
<li>
<a href="https://im4change.in/video/Public-Spending-on-Agriculture-in-India-Source-Foundation-for-Agrarian-Studies"
title="Public Spending on Agriculture in India (Source: Foundation for Agrarian Studies)" target="_blank">
Public Spending on Agriculture in India (Source: Foundation for...</a>
</li>
<li>
<a href="https://im4change.in/video/Agrarian-Change-Seminar-Protests-against-the-New-Farm-Laws-in-India-by-Prof-Vikas-Rawal-JNU-Source-Journal-Of-Agrarian-Change"
title="Agrarian Change Seminar: 'Protests against the New Farm Laws in India' by Prof. Vikas Rawal, JNU (Source: Journal Of Agrarian Change) " target="_blank">
Agrarian Change Seminar: 'Protests against the New Farm Laws...</a>
</li>
<li>
<a href="https://im4change.in/video/Webinar-Ramrao-The-Story-of-India-Farm-Crisis-Source-Azim-Premji-University"
title="Webinar: Ramrao - The Story of India's Farm Crisis (Source: Azim Premji University)" target="_blank">
Webinar: Ramrao - The Story of India's Farm Crisis...</a>
</li>
<li>
<a href="https://im4change.in/video/water-and-agricultural-transformation-in-India"
title="Water and Agricultural Transformation in India: A Symbiotic Relationship (Source: IGIDR)" target="_blank">
Water and Agricultural Transformation in India: A Symbiotic Relationship...</a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/videogallery"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
</div>
</div>
</div>
</section> </div>
<div class="clear"></div>
<!-- Footer option Starts here -->
<div class="footer-bottom fade-in animated4">
<div class="container">
<div class="social-icons icon_flat">
<p class="SocialMargTop"> Website Developed by <a target="_blank" title="Web Development"
class="wot right"
href="http://www.ravinderkhurana.com/" rel="nofollow">
RAVINDErkHURANA.com</a></p>
</div>
<div class="alignleft">
<a
target="_blank" href="https://im4change.in/objectives-8.html"
class="link"
title="Objectives">Objectives</a> | <a
target="_blank" href="https://im4change.in/about-us-9.html"
class="link" title="About Us">About Us</a> | <a
target="_blank" href="https://im4change.in/media-workshops.php"
class="ucwords">Workshops</a> | <a
target="_blank" href="https://im4change.in/disclaimer/disclaimer-149.html"
title="Disclaimer">Disclaimer</a> </div>
</div>
</div>
<!-- Footer option ends here -->
</div>
<div id="connect">
<a target="_blank"
href="http://www.facebook.com/sharer.php?u=https://im4change.in/latest-news-updates/question-of-efficacy-leena-menghaney-14576.html"
title="Share on Facebook">
<img src="https://im4change.in/images/Facebook.png?1582080640" alt="share on Facebook" class="ImgBorder"/>
</a><br/>
<a target="_blank"
href="http://twitter.com/share?text=Im4change&url=https://im4change.in/latest-news-updates/question-of-efficacy-leena-menghaney-14576.html"
title="Share on Twitter">
<img src="https://im4change.in/images/twitter.png?1582080632" alt="Twitter" class="ImgBorder"/> </a>
<br/>
<a href="/feeds" title="RSS Feed" target="_blank">
<img src="https://im4change.in/images/rss.png?1582080632" alt="RSS" class="ImgBorder"/>
</a>
<br/>
<a class="feedback-link" id="feedbackFormLink" href="#">
<img src="https://im4change.in/images/feedback.png?1582080630" alt="Feedback" class="ImgBorder"/>
</a> <br/>
<a href="javascript:function iprl5(){var d=document,z=d.createElement('scr'+'ipt'),b=d.body,l=d.location;try{if(!b)throw(0);d.title='(Saving...) '+d.title;z.setAttribute('src',l.protocol+'//www.instapaper.com/j/WKrH3R7ORD5p?u='+encodeURIComponent(l.href)+'&t='+(new Date().getTime()));b.appendChild(z);}catch(e){alert('Please wait until the page has loaded.');}}iprl5();void(0)"
class="bookmarklet" onclick="return explain_bookmarklet();">
<img src="https://im4change.in/images/read-it-later.png?1582080632" alt="Read Later" class="ImgBorder"/> </a>
</div>
<!-- Feedback form Starts here -->
<div id="feedbackForm" class="overlay_form" class="ImgBorder">
<h2>Contact Form</h2>
<div id="contactform1">
<div id="formleft">
<form id="submitform" action="/contactus.php" method="post">
<input type="hidden" name="submitform" value="submitform"/>
<input type="hidden" name="salt_key" value="a0e0f2c6a0644a70e57ad2c96829709a"/>
<input type="hidden" name="ref" value="feedback"/>
<fieldset>
<label>Name :</label>
<input type="text" name="name" class="tbox" required/>
</fieldset>
<fieldset>
<label>Email :</label>
<input type="text" name="email" class="tbox" required/>
</fieldset>
<fieldset>
<label>Message :</label>
<textarea rows="5" cols="20" name="message" required></textarea>
</fieldset>
<fieldset>
Please enter security code
<div class="clear"></div>
<input type="text" name="vrcode" class="tbox"/>
</fieldset>
<fieldset>
<input type="submit" class="button" value="Submit"/>
<a href="#" id="closefeedbakcformLink">Close</a>
</fieldset>
</form>
</div>
<div class="clearfix"></div>
</div>
</div>
<div id="donate_popup" class="modal" style="max-width: 800px;">
<table width="100%" border="1">
<tr>
<td colspan="2" align="center">
<b>Support im4change</b>
</td>
</tr>
<tr>
<td width="25%" valign="middle">
<img src="https://im4change.in/images/logo2.jpg?1582080632" alt="" width="100%"/> </td>
<td style="padding-left:10px;padding-top:10px;">
<form action="https://im4change.in/donate" method="get">
<table width="100%" cellpadding="2" cellspacing="2">
<tr>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
10
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
100
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
1000
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
50
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
500
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
<input type="text" name="price" placeholder="?" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td colspan="3" align="right">
<input type="button" name="Pay" value="Pay"
style="width: 200px;background-color: rgb(205, 35, 36);color: #ffffff;"/>
</td>
</tr>
</table>
</form>
</td>
</tr>
</table>
</div><script type='text/javascript'>
/* <![CDATA[ */
var tievar = {'go_to': 'Go to...'};
/* ]]> */
</script>
<script src="/js/tie-scripts.js?1575549704"></script><script src="/js/bootstrap.js?1575549704"></script><script src="/js/jquery.modal.min.js?1578284310"></script><script>
$(document).ready(function() {
// tell the autocomplete function to get its data from our php script
$('#s').autocomplete({
source: "/autocomplete"
});
});
</script>
<script src="/vj-main-sw-register.js" async></script>
<script>function init(){var imgDefer=document.getElementsByTagName('img');for(var i=0;i<imgDefer.length;i++){if(imgDefer[i].getAttribute('data-src')){imgDefer[i].setAttribute('src',imgDefer[i].getAttribute('data-src'))}}}
window.onload=init;</script>
</body>
</html>'
}
$maxBufferLength = (int) 8192
$file = '/home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php'
$line = (int) 853
$message = 'Unable to emit headers. Headers sent in file=/home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php line=853'
Cake\Http\ResponseEmitter::emit() - CORE/src/Http/ResponseEmitter.php, line 48
Cake\Http\Server::emit() - CORE/src/Http/Server.php, line 141
[main] - ROOT/webroot/index.php, line 39
Warning (2): Cannot modify header information - headers already sent by (output started at /home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php:853) [CORE/src/Http/ResponseEmitter.php, line 148]
$response = object(Cake\Http\Response) {
'status' => (int) 200,
'contentType' => 'text/html',
'headers' => [
'Content-Type' => [
[maximum depth reached]
]
],
'file' => null,
'fileRange' => [],
'cookies' => object(Cake\Http\Cookie\CookieCollection) {},
'cacheDirectives' => [],
'body' => '<!DOCTYPE html>
<!--[if lt IE 7 ]>
<html class="ie ie6" lang='en'> <![endif]-->
<!--[if IE 7 ]>
<html class="ie ie7" lang='en'> <![endif]-->
<!--[if IE 8 ]>
<html class="ie ie8" lang='en'> <![endif]-->
<!--[if (gte IE 9)|!(IE)]><!-->
<html lang='en'>
<!--<![endif]-->
<head><meta http-equiv="Content-Type" content="text/html; charset=utf-8">
<title>
LATEST NEWS UPDATES | Question of efficacy -Leena Menghaney </title>
<meta name="description" content="
The country is clearly shaping its legislation to promote access to medicines by fostering generic production.
INDIA'S approach to the revision of its Patents Act in 2005 is a clear example of a country shaping its legislation to promote access..."/>
<meta name="keywords" content="Health,patents,medicines"/>
<meta name="news_keywords" content="Health,patents,medicines">
<link rel="alternate" type="application/rss+xml" title="ROR" href="/ror.xml"/>
<link rel="alternate" type="application/rss+xml" title="RSS 2.0" href="/feeds/"/>
<link rel="stylesheet" href="/css/bootstrap.min.css?1697864993"/> <link rel="stylesheet" href="/css/style.css?v=1.1.2"/> <link rel="stylesheet" href="/css/style-inner.css?1577045210"/> <link rel="stylesheet" id="Oswald-css"
href="https://fonts.googleapis.com/css?family=Oswald%3Aregular%2C700&ver=3.8.1" type="text/css"
media="all">
<link rel="stylesheet" href="/css/jquery.modal.min.css?1578285302"/> <script src="/js/jquery-1.10.2.js?1575549704"></script> <script src="/js/jquery-migrate.min.js?1575549704"></script> <link rel="shortcut icon" href="/favicon.ico" title="Favicon">
<link rel="stylesheet" href="/css/jquery-ui.css?1580720609"/> <script src="/js/jquery-ui.js?1575549704"></script> <link rel="preload" as="style" href="https://www.im4change.org/css/custom.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery.modal.min.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery-ui.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/li-scroller.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<!-- <link rel="preload" as="style" href="https://www.im4change.org/css/style.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous"> -->
<link rel="preload" as="style" href="https://www.im4change.org/css/style-inner.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel='dns-prefetch' href="//im4change.org/css/custom.css" crossorigin >
<link rel="preload" as="script" href="https://www.im4change.org/js/bootstrap.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.li-scroller.1.0.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.modal.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.ui.totop.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-1.10.2.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-migrate.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-ui.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/setting.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/tie-scripts.js">
<!--[if IE]>
<script type="text/javascript">jQuery(document).ready(function () {
jQuery(".menu-item").has("ul").children("a").attr("aria-haspopup", "true");
});</script>
<![endif]-->
<!--[if lt IE 9]>
<script src="/js/html5.js"></script>
<script src="/js/selectivizr-min.js"></script>
<![endif]-->
<!--[if IE 8]>
<link rel="stylesheet" type="text/css" media="all" href="/css/ie8.css"/>
<![endif]-->
<meta property="og:title" content="LATEST NEWS UPDATES | Question of efficacy -Leena Menghaney" />
<meta property="og:url" content="https://im4change.in/latest-news-updates/question-of-efficacy-leena-menghaney-14576.html" />
<meta property="og:type" content="article" />
<meta property="og:description" content="
The country is clearly shaping its legislation to promote access to medicines by fostering generic production.
INDIA'S approach to the revision of its Patents Act in 2005 is a clear example of a country shaping its legislation to promote access..." />
<meta property="og:image" content="" />
<meta property="fb:app_id" content="0" />
<meta name="viewport" content="width=device-width, initial-scale=1, maximum-scale=1, user-scalable=no">
<link rel="apple-touch-icon-precomposed" sizes="144x144" href="https://im4change.in/images/apple1.png">
<link rel="apple-touch-icon-precomposed" sizes="120x120" href="https://im4change.in/images/apple2.png">
<link rel="apple-touch-icon-precomposed" sizes="72x72" href="https://im4change.in/images/apple3.png">
<link rel="apple-touch-icon-precomposed" href="https://im4change.in/images/apple4.png">
<style>
.gsc-results-wrapper-overlay{
top: 38% !important;
height: 50% !important;
}
.gsc-search-button-v2{
border-color: #035588 !important;
background-color: #035588 !important;
}
.gsib_a{
height: 30px !important;
padding: 2px 8px 1px 6px !important;
}
.gsc-search-button-v2{
height: 41px !important;
}
input.gsc-input{
background: none !important;
}
@media only screen and (max-width: 600px) {
.gsc-results-wrapper-overlay{
top: 11% !important;
width: 87% !important;
left: 9% !important;
height: 43% !important;
}
.gsc-search-button-v2{
padding: 10px 10px !important;
}
.gsc-input-box{
height: 28px !important;
}
/* .gsib_a {
padding: 0px 9px 4px 9px !important;
}*/
}
@media only screen and (min-width: 1200px) and (max-width: 1920px) {
table.gsc-search-box{
width: 15% !important;
float: right !important;
margin-top: -118px !important;
}
.gsc-search-button-v2 {
padding: 6px !important;
}
}
</style>
<script>
$(function () {
$("#accordion").accordion({
event: "click hoverintent"
});
});
/*
* hoverIntent | Copyright 2011 Brian Cherne
* http://cherne.net/brian/resources/jquery.hoverIntent.html
* modified by the jQuery UI team
*/
$.event.special.hoverintent = {
setup: function () {
$(this).bind("mouseover", jQuery.event.special.hoverintent.handler);
},
teardown: function () {
$(this).unbind("mouseover", jQuery.event.special.hoverintent.handler);
},
handler: function (event) {
var currentX, currentY, timeout,
args = arguments,
target = $(event.target),
previousX = event.pageX,
previousY = event.pageY;
function track(event) {
currentX = event.pageX;
currentY = event.pageY;
}
;
function clear() {
target
.unbind("mousemove", track)
.unbind("mouseout", clear);
clearTimeout(timeout);
}
function handler() {
var prop,
orig = event;
if ((Math.abs(previousX - currentX) +
Math.abs(previousY - currentY)) < 7) {
clear();
event = $.Event("hoverintent");
for (prop in orig) {
if (!(prop in event)) {
event[prop] = orig[prop];
}
}
// Prevent accessing the original event since the new event
// is fired asynchronously and the old event is no longer
// usable (#6028)
delete event.originalEvent;
target.trigger(event);
} else {
previousX = currentX;
previousY = currentY;
timeout = setTimeout(handler, 100);
}
}
timeout = setTimeout(handler, 100);
target.bind({
mousemove: track,
mouseout: clear
});
}
};
</script>
<script type="text/javascript">
var _gaq = _gaq || [];
_gaq.push(['_setAccount', 'UA-472075-3']);
_gaq.push(['_trackPageview']);
(function () {
var ga = document.createElement('script');
ga.type = 'text/javascript';
ga.async = true;
ga.src = ('https:' == document.location.protocol ? 'https://ssl' : 'http://www') + '.google-analytics.com/ga.js';
var s = document.getElementsByTagName('script')[0];
s.parentNode.insertBefore(ga, s);
})();
</script>
<link rel="stylesheet" href="/css/custom.css?v=1.16"/> <script src="/js/jquery.ui.totop.js?1575549704"></script> <script src="/js/setting.js?1575549704"></script> <link rel="manifest" href="/manifest.json">
<meta name="theme-color" content="#616163" />
<meta name="apple-mobile-web-app-capable" content="yes">
<meta name="apple-mobile-web-app-status-bar-style" content="black">
<meta name="apple-mobile-web-app-title" content="im4change">
<link rel="apple-touch-icon" href="/icons/logo-192x192.png">
</head>
<body id="top" class="home inner blog">
<div class="background-cover"></div>
<div class="wrapper animated">
<header id="theme-header" class="header_inner" style="position: relative;">
<div class="logo inner_logo" style="left:20px !important">
<a title="Home" href="https://im4change.in/">
<img src="https://im4change.in/images/logo2.jpg?1582080632" class="logo_image" alt="im4change"/> </a>
</div>
<div class="langhindi" style="color: #000;display:none;"
href="https://im4change.in/">
<a class="more-link" href="https://im4change.in/">Home</a>
<a href="https://im4change.in/hindi/" class="langbutton ">हिन्दी</a>
</div>
<nav class="fade-in animated2" id="main-nav">
<div class="container">
<div class="main-menu">
<ul class="menu" id="menu-main">
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
style="left: -40px;"><a
target="_blank" href="https://im4change.in/">Home</a>
</li>
<li class="menu-item mega-menu menu-item-type-taxonomy mega-menu menu-item-object-category mega-menu menu-item-has-children parent-list"
style=" margin-left: -40px;"><a href="#">KNOWLEDGE GATEWAY <span class="sub-indicator"></span>
</a>
<div class="mega-menu-block background_menu" style="padding-top:25px;">
<div class="container">
<div class="mega-menu-content">
<div class="mega-menu-item">
<h3><b>Farm Crisis</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/farmers039-suicides-14.html"
class="left postionrel">Farm Suicides </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/unemployment-30.html"
class="left postionrel">Unemployment </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/rural-distress-70.html"
class="left postionrel">Rural distress </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/migration-34.html"
class="left postionrel">Migration </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/key-facts-72.html"
class="left postionrel">Key Facts </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/debt-trap-15.html"
class="left postionrel">Debt Trap </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Empowerment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/union-budget-73.html"
class="left postionrel">Union Budget And Other Economic Policies </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/forest-and-tribal-rights-61.html"
class="left postionrel">Forest and Tribal Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-education-60.html"
class="left postionrel">Right to Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-food-59.html"
class="left postionrel">Right to Food </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/displacement-3279.html"
class="left postionrel">Displacement </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-work-mg-nrega-39.html"
class="left postionrel">Right to Work (MG-NREGA) </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/gender-3280.html"
class="left postionrel">GENDER </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-information-58.html"
class="left postionrel">Right to Information </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/social-audit-48.html"
class="left postionrel">Social Audit </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Hunger / HDI</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/poverty-and-inequality-20499.html"
class="left postionrel">Poverty and inequality </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/malnutrition-41.html"
class="left postionrel">Malnutrition </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/public-health-51.html"
class="left postionrel">Public Health </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/education-50.html"
class="left postionrel">Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hunger-overview-40.html"
class="left postionrel">Hunger Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hdi-overview-45.html"
class="left postionrel">HDI Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/pds-ration-food-security-42.html"
class="left postionrel">PDS/ Ration/ Food Security </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/sdgs-113.html"
class="left postionrel">SDGs </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/mid-day-meal-scheme-mdms-53.html"
class="left postionrel">Mid Day Meal Scheme (MDMS) </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Environment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/time-bomb-ticking-52.html"
class="left postionrel">Time Bomb Ticking </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/water-and-sanitation-55.html"
class="left postionrel">Water and Sanitation </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/impact-on-agriculture-54.html"
class="left postionrel">Impact on Agriculture </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Law & Justice</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/social-justice-20500.html"
class="left postionrel">Social Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/access-to-justice-47.html"
class="left postionrel">Access to Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/human-rights-56.html"
class="left postionrel">Human Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/corruption-35.html"
class="left postionrel">Corruption </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/general-insecurity-46.html"
class="left postionrel">General Insecurity </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/disaster-relief-49.html"
class="left postionrel">Disaster & Relief </a>
</p>
</div>
</div>
</div>
</div>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page "><a target="_blank" href="https://im4change.in/nceus_reports.php">NCEUS reports</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children parent-list ">
<a target="_blank" href="https://im4change.in/about-us-9.html">About Us <span
class="sub-indicator"></span></a>
<ul class="sub-menu aboutmenu">
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/objectives-8.html">Objectives</a>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/contactus.php">Contact
Us</a></li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/about-us-9.html">About
Us</a></li>
</ul>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children ">
<a target="_blank" href="https://im4change.in/fellowships.php" title="Fellowships">Fellowships</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/media-workshops.php">Workshops</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/research.php">Research</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/links-64">Partners</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
id="menu-item-539"><a target="_blank" href="https://im4change.in/hindi/"
class="langbutton langlinkfont17">हिन्दी</a></li>
</ul>
</div> </div>
<!-- <div style="float: right;">
<script async src="https://cse.google.com/cse.js?cx=18b4f2e0f11bed3dd"></script>
<div class="gcse-search"></div>
</div> -->
<div class="search-block" style=" margin-left: 8px; margin-right: 7px;">
<form method="get" id="searchform" name="searchform"
action="https://im4change.in/search"
onsubmit="return searchvalidate();">
<button class="search-button" type="submit" value="Search"></button>
<input type="text" id="s" name="qryStr" value=""
onfocus="if (this.value == 'Search...') {this.value = '';}"
onblur="if (this.value == '') {this.value = 'Search...';}">
</form>
</div>
</nav>
</header>
<div class="container">
<div id="main-content" class=" main1 container fade-in animated3 sidebar-narrow-left">
<div class="content-wrap">
<div class="content" style="width: 900px;min-height: 500px;">
<section class="cat-box recent-box innerCatRecent">
<h1 class="cat-box-title">Question of efficacy -Leena Menghaney</h1>
<a href="JavaScript:void(0);" onclick="return shareArticle(14452);">
<img src="https://im4change.in/images/email.png?1582080630" border="0" width="24" align="right" alt="Share this article"/> </a>
<a href="https://im4change.in/latest-news-updates/question-of-efficacy-leena-menghaney-14576/print"
rel="nofollow">
<img src="https://im4change.in/images/icon-print.png?1582080630" border="0" width="24" align="right" alt="Share this article"/>
</a>
</section>
<section class="recent-box innerCatRecent">
<small class="pb-1"><span class="dateIcn">
<img src="https://im4change.in/images/published.svg?1582080666" alt="published"/>
Published on</span><span class="text-date"> Apr 20, 2012</span>
<span
class="dateIcn">
<img src="https://im4change.in/images/modified.svg?1582080666" alt="modified"/> Modified on </span><span class="text-date"> Apr 20, 2012</span>
</small>
</section>
<div class="clear"></div>
<div style="padding-top: 10px;">
<div class="innerLineHeight">
<div class="middleContent innerInput latest-news-updates">
<table>
<tr>
<td>
<div>
<br /><div align="justify"><em>The country is clearly shaping its legislation to promote access to medicines by fostering generic production. <br /></em><img src="https://im4change.in/siteadmin/tinymce/uploaded/Patent 1.bmp" alt="Patent 1" /><br />INDIA'S approach to the revision of its Patents Act in 2005 is a clear example of a country shaping its legislation to promote access to medicines by fostering generic production. Although World Trade Organisation (WTO) rules made it mandatory for India to put in place a patent regime for medicines by 2005, nothing obliges developing countries such as India to replicate the patent system of wealthy countries, which involves charging the highest possible price and protecting that price through patent monopolies that extend way beyond 20 years.<br /><br />India has used important flexibilities under international law to include provisions in its domestic patent law not only to reduce the number of secondary patents but also to have a licensing mechanism that kicks in with excessive pricing of patented medicines. The application of these safeguards by the Indian patent office – benefiting patients in India and other developing countries – is increasingly inviting the ire of the multinational pharmaceutical industry and its associations.<br /><br />The Indian government is faced with court cases and the diplomatic offensive that the protectors of the pharmaceutical industry in the United States and the European Union are now launching.<br /><br />In India, the importance of generic (local) production of medicines in fostering competition and reducing prices was first recognised by lawmakers in the Patents Act of 1970, which brought in a legal regime that did not allow product patents on pharmaceuticals. In the following decades, India not only was successful in making drugs affordable but also significantly increased their availability by building domestic capacity to produce essential and life-saving drugs. It also went on to become the “pharmacy of the developing world”, supplying medicines to countries that lacked the capacity and resources to produce the drugs themselves or pay the high prices demanded by originator pharmaceutical companies.<br /><br />The production of more affordable generic medicines in India has been instrumental in driving down the price of AIDS (acquired immune deficiency syndrome) medicines by 99 per cent, and nearly six million people living with HIV have been put on treatment on Indian generic medicines in the past 10 years.<br /><br />In 2005, India was obliged to change its patent law in order to comply with its obligations as a member of the WTO, bringing into effect the TRIPS Agreement. The most significant change was the introduction of product patents for medicines. When framing the new patent legislation in 2005, Parliament sought to ensure that provisions to protect public health and access to medicines were incorporated into it. It, therefore, included explicit legal safeguards and guidance on how the patentability requirements should be applied.<br /><br />In particular, evergreening, a well-known abuse of the patent system where companies seek new monopolies or, alternatively, extend a monopoly by seeking to patent minor changes – such as new uses, new forms and other routine improvements of known medicines – was addressed. Section 3(d) of the Indian Patents Act explicitly allows the broad exclusion from patentability of new uses and new forms of known medicines. In sum, Section 3(d) gave explicit guidance to the Indian patent office on how to weed out patent claims on routine improvements of known medicines and protect the country's capacity to act as a factory for the production and supply of affordable generic medicines.<br /></div><div align="justify"> </div><div align="justify"><em>Legal challenge<br /></em><br />In 2006, in a landmark decision, the Indian patent office rejected Swiss pharmaceutical company Novartis' patent application for the life-saving anti-cancer drug imatinib mesylate. The application for a patent on a beta crystalline salt form of imatinib was rejected on the grounds that it lacked novelty, was obvious, and was un-patentable under Section 3(d) of the Patents Act. In retaliation, Novartis mounted a legal challenge to have Section 3(d) declared unconstitutional. Medecins Sans Frontieres (MSF) launched an international campaign calling on the company to drop the case, attracting close to half a million signatures. In 2007, the Madras High Court rejected Novartis' plea and in 2009 the Intellectual Property Appellate Board (IPAB) rejected its patent application on imatinib mesylate once again.<br /><img src="https://im4change.in/siteadmin/tinymce/uploaded/Patent 2.bmp" alt="Patent 2" /><br />But the company is not backing down. After failing to have Section 3(d) struck down, it is now again seeking to limit its effect. In 2009, Novartis filed a special leave petition in the Supreme Court against India in relation to the patentability criteria to be applied to imatinib mesylate.<br /><br />Under Section 3(d) of the Patents Act, new forms of already known substances cannot be patented if they fail to demonstrate the required degree of efficacy; it requires demonstration of increased efficacy for a medicine to deserve a patent. The interpretation of the definition of “efficacy” is therefore central to this case and to the future of India's role as the pharmacy of the developing world.<br /><br />In 2007, in its constitutional challenge against Section 3(d) before the Madras High Court, Novartis had argued that increased bioavailability of the salt form of imatinib meant increased efficacy, entitling it to a patent. But the High Court clarified that efficacy meant “therapeutic effect in healing a disease”.<br /><br />The IPAB, where appeals for unsuccessful patent applications are heard, subsequently applied this interpretation and held that the salt form of imatinib mesylate did not meet the test of therapeutic efficacy. It, therefore, confirmed the rejection of Novartis's patent application.<br /></div><div align="justify"> </div><div align="justify"><em>High standards crucial for tests in patent law<br /></em><br />Setting high standards for the various tests in the patent legislation, particularly the “efficacy” test of Section 3(d) and the inventive step requirement, leading to fewer patents on new forms of known medicines, is important to safeguard access to affordable generic medicines from India. Novartis has now taken its case to the Supreme Court to argue against the interpretation of “efficacy” in Section 3(d) by the Madras High Court and the IPAB. This case has the potential to severely affect access to affordable essential medicines for millions of people across the developing world. It will determine whether Section 3(d) will continue to ensure that patents are granted only on medicines that are truly new and inventive. Many developing countries rely on affordable medicines produced in India, and such medicines constitute over 80 per cent of the AIDS drugs used in the developing world. MSF is closely following the outcome of this case.<br /><br />Novartis is basing its claim for a patent on the salt of imatinib on the fact that there is a 30 per cent increase in the bioavailability of the drug in this new form. But, according to the guidelines for the examination of pharmaceutical patents developed by the World Health Organisation (WHO) and the International Centre for Trade and Sustainable Development (ICTSD), the selection of a salt of the active ingredient with the purpose to improve bioavailability is known in pharmaceutical science. It is common knowledge in the field that salts result in different solubility and, therefore, in different bioavailability.<br /><br />The final arguments in the case have started. The next date of hearing is set for July 10. If Novartis wins, many other medicines, even those that show no increased therapeutic efficacy, will be patentable in India, and the availability of affordable medicines will be threatened. If the substance is taken out of Section 3(d), abusive “evergreening” practices, where drug companies maintain artificially high prices on medicines well beyond the original patent period by securing fresh patents on minor modifications of existing drugs, will become rampant in the future.<br /><br />If, on the other hand, the high threshold for patentability is upheld, generic production will continue to drive the price of life-saving medicines down. Multinational pharmaceutical companies such as Novartis will find it difficult to argue that routine improvements – such as new forms of existing medicines that result in improved stability, enhanced bioavailability, increased solubility, improved flow properties and lower hygroscopicity – meet the efficacy requirements of Section 3(d). In addition, the improved therapeutic efficacy would have to be supported with actual clinical data that demonstrate this effect.<br /><br />The Supreme Court case is the final act in a legal battle that stretches back over six years between Novartis and the Indian government. The government, hopefully, will argue for a strict interpretation of “efficacy” so that patents on new forms of known medicines – such as the one on the cancer drug imatinib mesylate – are not granted as a matter of routine by the country's patent office. Novartis has lined up very senior and very expensive lawyers, including two former Solicitors General, to argue its case. But there appears to be no information on whether the government has appointed its own top lawyer, the Attorney General, in this case.<br /></div><div align="justify"> </div><div align="justify"><em>Opening the door for compulsory licensing<br /></em><br />In another test case on access to treatment, seven years after India revised its 1970 Patents Act, the Controller General of Patents issued the first-ever compulsory licence (CL) to the Hyderabad-based company Natco to produce an affordable version of a patented anti-cancer medicine (sorafenib tosylate) of the German pharmaceutical company Bayer Corporation, marketed under the brand name of Nexavar. The generic version produced by Natco, which will pay 6 per cent royalty on net sales to Bayer, will be 97 per cent cheaper.<br /><br />The decision was made on the basis of the fact that not only had the patentee, Bayer, failed to price sorafenib tosylate at a level that made it accessible and affordable but it was also unable to ensure that the medicine was available in sufficient and sustainable quantities within India. Bayer has time until mid-June to appeal against the order.<br /><br />Like many other giant drug companies, Bayer defended the inflated cost of sorafenib by specifying the high spending on research and development. However, what it did not highlight was that the United States National Institutes of Health had sponsored almost 70 per cent of the second phase of its clinical trials. Later, this drug was given an “orphan drug” designation by the U.S.' Food and Drug Administration (FDA) for the treatment of renal cell carcinoma, entitling Bayer to 50 per cent tax credits, which further lowered the company's costs for the third and most expensive phase of clinical trials.<br /><br />The CL is quickly being dubbed by pharmaceutical companies such as Novartis as a move that will stifle innovation. Indeed, pharmaceutical companies at present try to recover their investments by charging excessively high prices and protecting their drugs through patent monopolies. However, R&D costs are only a fraction of the profits thus made, and a large part of the profits are spent on brand-building and marketing. In 2011, Bayer spent nearly €9 billion on sales and advertising. In the same period, only €2.9 billion was spent on research.<br /><br />The patent system also has another drawback. Innovation currently fails to address the needs of patients in developing countries.<br /><br />The drug companies also repeatedly warn that measures such as the CL adversely affect the confidence of foreign investors. But a study published in Thailand in 2009 by the Health Intervention and Technology Assessment Program (HITAP) found little evidence of a link between the granting of CLs and the level of foreign direct investment (FDI) in the country.<br /><br />The recently granted CL actually highlights a potentially new patent model that routinely allows low-cost alternatives in lieu of royalty payments, not only helping originators to recoup their development costs but also ensuring that people in developing countries have access to medicines. It is in line with licensing decisions in other jurisdictions. Recently, a U.S. court decided not to prevent a competitor from marketing a medical device used for skin grafts, and instead put in place a system of royalties from the competitor to the patent owner. At the core of this decision was the idea that the public has a right to access innovative health products and this should not be blocked by excessive prices.<br /><br />The Novartis and Bayer cases highlight that the country is entering a new era in which disputes on the public's access to and the affordability of drugs will become more frequent.<br /><br /><em>Leena Menghaney is campaign coordinator of Medecins Sans Frontieres in India and is based in New Delhi. </em><br /></div>
</div>
</td>
</tr>
</table>
</div>
</div>
</div>
<div class="clear"></div>
<br><a href="http://www.frontlineonnet.com/stories/20120504290802200.htm" class="re" target="_blank">Frontline, Volume 29, Issue 08, 21 April-04 May, 2012, http://www.frontlineonnet.com/stories/20120504290802200.htm</a><div class="clear"></div>
<div style="padding-top: 18px;">
<p class="post-tag">Tagged with:
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Health"
title="Health">
Health </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=patents"
title="patents">
patents </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=medicines"
title="medicines">
medicines </a>
</p>
</div>
<div class="clear"></div>
<br><br>
<div class="widget-top">
<h4>Related Articles</h4>
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<ul id="recentcomments">
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/fifth-report-from-gambia-implicates-indian-drug-maker-for-contaminated-syrups-banjot-kaur.html"
title="Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur">
Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-may-have-seen-steepest-dip-in-multidimensional-poverty-among-110-nations-as-per-undp-data-nikhil-rampal.html"
title="India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal">
India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/health-among-top-three-priorities-for-indian-voters-after-jobs-and-education-survey-shows-oliver-heath-jyoti-mishra-louise-tillin-sandhya-venkateswaran.html"
title="Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran">
Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/prevalence-of-zero-food-among-infants-and-young-children-in-india-patterns-of-change-across-the-states-and-union-territories-of-india-1993-2021-the-lancet.html"
title="Prevalence of Zero-Food among infants and young children in India - The Lancet ">
Prevalence of Zero-Food among infants and young children in India - The Lancet </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-s-sustainability-goals-at-risk-because-of-extreme-heatwaves-carbon-copy.html"
title="India's Sustainability Goals at Risk Because of Extreme Heatwaves - Carbon Copy">
India's Sustainability Goals at Risk Because of Extreme Heatwaves - Carbon Copy </a>
</li>
</ul>
</div>
<div class="comment-respond" id="respond">
<a name="commentbox"> </a>
<h3 class="comment-reply-title" id="reply-title">Write Comments</h3>
<form method="post" accept-charset="utf-8" role="form" action="/latest-news-updates/question-of-efficacy-leena-menghaney-14576.html"><div style="display:none;"><input type="hidden" name="_method" value="POST"/></div> <form class="comment-form" id="commentform" method="post" action="#commentbox" onSubmit="return validate()"
name="cmtform">
<input type="hidden" name="cmttype" value="articlecmt"/>
<input type="hidden" name="article_id" value="14452"/>
<p class="comment-notes">Your email address will not be published. Required fields are marked <span
class="required">*</span></p>
<p class="comment-form-author">
<label for="commenterName">Name</label>
<span class="required">*</span>
<input type="text" aria-required="true" size="30"
value=""
name="commenterName" id="commenterName" required="true">
</p>
<p class="comment-form-email">
<label for="commenterEmail">Email</label> <span class="required">*</span>
<input aria-required="true" size="30" name="commenterEmail" id="commenterEmail" type="email"
value=""
required="true">
</p>
<p class="comment-form-contact">
<label for="commenterPh">Contact No.</label>
<input type="text" size="30"
value=""
name="commenterPh" id="commenterPh">
</p>
<p class="comment-form-comment">
<label for="comment">Comment</label>
<textarea aria-required="true" required="true" rows="8" cols="45" name="comment"
id="comment"></textarea>
</p>
<p class="comment-form-comment">
<label for="comment">Type the characters you see in the image below <span class="required">*</span><br><img
class="captchaImg"
src="https://im4change.in/securimage_show_art.php?tk=2001382256" alt="captcha"/>
</label>
</p>
<input type="text" name="vrcode" required="true"/>
<p class="form-submit" style="width: 200px;">
<input type="submit" value="Post Comment" id="submit" name="submit">
</p></form>
</div>
<style>
.ui-widget-content {
height: auto !important;
}
</style>
<div id="share-modal"></div>
<style>
.middleContent a{
background-color: rgba(108,172,228,.2);
}
.middleContent a:hover{
background-color: #418fde;
border-color: #418fde;
color: #000;
}
</style>
<script>
function shareArticle(article_id) {
var options = {
modal: true,
height: 'auto',
width: 600 + 'px'
};
$('#share-modal').html("");
$('#share-modal').load('https://im4change.in/share_article?article_id=' + article_id).dialog(options).dialog('open');
}
function postShare() {
var param = 'article_id=' + $("#article_id").val();
param = param + '&y_name=' + $("#y_name").val();
param = param + '&y_email=' + $("#y_email").val();
param = param + '&f_name=' + $("#f_name").val();
param = param + '&f_email=' + $("#f_email").val();
param = param + '&y_msg=' + $("#y_msg").val();
$.ajax({
type: "POST",
url: 'https://im4change.in/post_share_article',
data: param,
success: function (response) {
$('#share-modal').html("Thank You, Your message posted to ");
}
});
return false;
}
</script> </div>
</div>
<!-- Right Side Section Start -->
<!-- MAP Section START -->
<aside class="sidebar indexMarg">
<div class="ad-cell">
<a href="https://im4change.in/statemap.php" title="">
<img src="https://im4change.in/images/map_new_version.png?1582080666" alt="India State Map" class="indiamap" width="232" height="252"/> </a>
<div class="rightmapbox">
<div id="sideOne" class="docltitle"><a href="https://im4change.in/state-report/india/36" target="_blank">DOCUMENTS/
REPORTS</a></div>
<div id="sideTwo" class="statetitle"><a href="https://im4change.in/states.php"target="_blank">STATE DATA/
HDRs.</a></div>
</div>
<div class="widget widgePadTop"></div>
</div>
</aside>
<!-- MAP Section END -->
<aside class="sidebar sidePadbottom">
<div class="rightsmlbox1" >
<a href="https://im4change.in/knowledge_gateway" target="_blank" style="color: #035588;
font-size: 17px;">
KNOWLEDGE GATEWAY
</a>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/newsletter" target="_blank">
NEWSLETTER
</a>
</p>
</div>
</div>
<div class="rightsmlbox1" style="height: 325px;">
<div>
<p class="rightsmlbox1_title">
Interview with Prof. Ravi Srivastava
</p>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/video/interview-with-prof-ravi-srivastava-on-current-economic-crisis">
<img width="250" height="200" src="/images/interview_video_home.jpg" alt="Interview with Prof. Ravi Srivastava"/>
</a>
<!--
<iframe width="250" height="200" src="https://www.youtube.com/embed/MmaTlntk-wc" frameborder="0" allow="accelerometer; autoplay; encrypted-media; gyroscope; picture-in-picture" allowfullscreen=""></iframe>-->
</p>
<a href="https://im4change.in/videogallery" class="more-link CatArchalAnch1" target="_blank">
More videos
</a>
</div>
</div>
<div class="rightsmlbox1">
<div>
<!--div id="sstory" class="rightboxicons"></div--->
<p class="rightsmlbox1_title"><a href="https://im4change.in/list-success-stories" target="_blank">Success Stories</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/interviews" target="_blank">Interviews</a>
</p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a href="https://www.commoncause.in/page.php?id=10" >Donate</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/marquee"
class="isf_link more-link" title="India Focus?" style="border: 4px solid #fdd922;width: 90%;background-color: #fdd922;text-align: center;color: #000000;font-size:18px" target="_blank">India Focus</a></p> </div>
</div>
<div class="rightsmlbox1" style="height: 104px !important;">
<a href="https://im4change.in/quarterly_reports.php" target="_blank">
Quarterly Reports on Effect of Economic Slowdown on Employment in India (2008 - 2015)
</a>
</div>
<!-- <div class="rightsmlbox1">
<a href="https://play.google.com/store/apps/details?id=com.im4.im4change" target="_blank">
</a></div> -->
<!-- <section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">Most Visited</h2>
</section> -->
<!-- accordion Starts here -->
<!-- <div id="accordion" class="accordMarg">
</div> -->
<!-- accordion ends here -->
<!-- Widget Tag Cloud Starts here -->
<div id="tag_cloud-2" class="widget widget_tag_cloud">
<section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">MOST VISITED TAGS</h2>
</section>
<div class="widget-top wiPdTp">
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<div class="tagcloud">
<a href="https://im4change.in/search?qryStr=Agriculture"
target="_blank" class="tag-link-4 font4">Agriculture</a>
<a href="https://im4change.in/search?qryStr=Food Security"
target="_blank" class="tag-link-4 font4">Food Security</a>
<a href="https://im4change.in/search?qryStr=Law and Justice"
target="_blank" class="tag-link-4 font4">Law and Justice</a>
<a href="https://im4change.in/search?qryStr=Health"
target="_blank" class="tag-link-4 font4">Health</a>
<a href="https://im4change.in/search?qryStr=Right to Food"
target="_blank" class="tag-link-4 font4">Right to Food</a>
<a href="https://im4change.in/search?qryStr=Corruption"
target="_blank" class="tag-link-4 font4">Corruption</a>
<a href="https://im4change.in/search?qryStr=farming"
target="_blank" class="tag-link-4 font4">farming</a>
<a href="https://im4change.in/search?qryStr=Environment"
target="_blank" class="tag-link-4 font4">Environment</a>
<a href="https://im4change.in/search?qryStr=Right to Information"
target="_blank" class="tag-link-4 font4">Right to Information</a>
<a href="https://im4change.in/search?qryStr=NREGS"
target="_blank" class="tag-link-4 font4">NREGS</a>
<a href="https://im4change.in/search?qryStr=Human Rights"
target="_blank" class="tag-link-4 font4">Human Rights</a>
<a href="https://im4change.in/search?qryStr=Governance"
target="_blank" class="tag-link-4 font4">Governance</a>
<a href="https://im4change.in/search?qryStr=PDS"
target="_blank" class="tag-link-4 font4">PDS</a>
<a href="https://im4change.in/search?qryStr=COVID-19"
target="_blank" class="tag-link-4 font4">COVID-19</a>
<a href="https://im4change.in/search?qryStr=Land Acquisition"
target="_blank" class="tag-link-4 font4">Land Acquisition</a>
<a href="https://im4change.in/search?qryStr=mgnrega"
target="_blank" class="tag-link-4 font4">mgnrega</a>
<a href="https://im4change.in/search?qryStr=Farmers"
target="_blank" class="tag-link-4 font4">Farmers</a>
<a href="https://im4change.in/search?qryStr=transparency"
target="_blank" class="tag-link-4 font4">transparency</a>
<a href="https://im4change.in/search?qryStr=Gender"
target="_blank" class="tag-link-4 font4">Gender</a>
<a href="https://im4change.in/search?qryStr=Poverty"
target="_blank" class="tag-link-4 font4">Poverty</a>
<a href="https://im4change.in/search?qryStr=Farm Laws" target="_blank" class="tag-link-4 font4">Farm Laws
</a>
<a href="https://im4change.in/search?qryStr=Citizenship Amendment Act" target="_blank" class="tag-link-4 font4">Citizenship Amendment Act
</a>
<a href="https://im4change.in/search?qryStr=CAA NPR NRIC" target="_blank" class="tag-link-4 font4">CAA NPR NRIC
</a>
<a href="https://im4change.in/search?qryStr=Job Losses" target="_blank" class="tag-link-4 font4">Job Losses
</a>
<a href="https://im4change.in/search?qryStr=Migrant Workers" target="_blank" class="tag-link-4 font4">Migrant Workers
</a>
<a href="https://im4change.in/search?qryStr=Unemployment" target="_blank" class="tag-link-4 font4">Unemployment
</a>
<a href="https://im4change.in/search?qryStr=PMGKAY" target="_blank" class="tag-link-4 font4">PMGKAY
</a>
<a href="https://im4change.in/search?qryStr=PM-KISAN" target="_blank" class="tag-link-4 font4">PM-KISAN
</a>
<a href="https://im4change.in/search?qryStr=PM-CARES" target="_blank" class="tag-link-4 font4">PM-CARES
</a>
<a href="https://im4change.in/search?qryStr=LFPR" target="_blank" class="tag-link-4 font4">LFPR
</a>
</div>
</div>
</div>
<!-- Widget Tag Cloud Ends here -->
</aside>
<!-- Right Side Section End -->
</div>
<section class="cat-box cats-review-box footerSec">
<h2 class="cat-box-title vSec CatArcha">Video
Archives</h2>
<h2 class="cat-box-title CatArchaTitle">Archives</h2>
<div class="cat-box-content">
<div class="reviews-cat">
<div class="CatArchaDiv1">
<div class="CatArchaDiv2">
<ul>
<li>
<a href="https://im4change.in/news-alerts-57/moving-upstream-luni-fellowship.html" target="_blank">
Moving Upstream: Luni – Fellowship </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/135-million-indians-exited-multidimensional-poverty-as-per-government-figures-is-that-the-same-as-poverty-reduction.html" target="_blank">
135 Million Indians Exited “Multidimensional" Poverty as per Government... </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/explainer-why-are-tomato-prices-on-fire.html" target="_blank">
Explainer: Why are Tomato Prices on Fire? </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/nsso-survey-only-39-1-of-all-households-have-drinking-water-within-dwelling-46-7-of-rural-households-use-firewood-for-cooking.html" target="_blank">
NSSO Survey: Only 39.1% of all Households have Drinking... </a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/news-alerts-57"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/I51LYnP8BOk/1.jpg"
alt=" Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Short-Video-on-im4change-Hindi-website-Inclusive-Media-for-Change" target="_blank">
Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/kNqha-SwfIY/1.jpg"
alt=" "Session 1: Scope of IDEA and AgriStack" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-1- Scope-of-IDEA-and-AgriStack-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 1: Scope of IDEA and AgriStack" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/6kIVjlgZItk/1.jpg"
alt=" "Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-2-Farmer-Centric-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/2BeHTu0y7xc/1.jpg"
alt=" "Session 3: Future of Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-3-Future-of-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 3: Future of Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="divWidth">
<ul class="divWidthMarg">
<li>
<a href="https://im4change.in/video/Public-Spending-on-Agriculture-in-India-Source-Foundation-for-Agrarian-Studies"
title="Public Spending on Agriculture in India (Source: Foundation for Agrarian Studies)" target="_blank">
Public Spending on Agriculture in India (Source: Foundation for...</a>
</li>
<li>
<a href="https://im4change.in/video/Agrarian-Change-Seminar-Protests-against-the-New-Farm-Laws-in-India-by-Prof-Vikas-Rawal-JNU-Source-Journal-Of-Agrarian-Change"
title="Agrarian Change Seminar: 'Protests against the New Farm Laws in India' by Prof. Vikas Rawal, JNU (Source: Journal Of Agrarian Change) " target="_blank">
Agrarian Change Seminar: 'Protests against the New Farm Laws...</a>
</li>
<li>
<a href="https://im4change.in/video/Webinar-Ramrao-The-Story-of-India-Farm-Crisis-Source-Azim-Premji-University"
title="Webinar: Ramrao - The Story of India's Farm Crisis (Source: Azim Premji University)" target="_blank">
Webinar: Ramrao - The Story of India's Farm Crisis...</a>
</li>
<li>
<a href="https://im4change.in/video/water-and-agricultural-transformation-in-India"
title="Water and Agricultural Transformation in India: A Symbiotic Relationship (Source: IGIDR)" target="_blank">
Water and Agricultural Transformation in India: A Symbiotic Relationship...</a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/videogallery"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
</div>
</div>
</div>
</section> </div>
<div class="clear"></div>
<!-- Footer option Starts here -->
<div class="footer-bottom fade-in animated4">
<div class="container">
<div class="social-icons icon_flat">
<p class="SocialMargTop"> Website Developed by <a target="_blank" title="Web Development"
class="wot right"
href="http://www.ravinderkhurana.com/" rel="nofollow">
RAVINDErkHURANA.com</a></p>
</div>
<div class="alignleft">
<a
target="_blank" href="https://im4change.in/objectives-8.html"
class="link"
title="Objectives">Objectives</a> | <a
target="_blank" href="https://im4change.in/about-us-9.html"
class="link" title="About Us">About Us</a> | <a
target="_blank" href="https://im4change.in/media-workshops.php"
class="ucwords">Workshops</a> | <a
target="_blank" href="https://im4change.in/disclaimer/disclaimer-149.html"
title="Disclaimer">Disclaimer</a> </div>
</div>
</div>
<!-- Footer option ends here -->
</div>
<div id="connect">
<a target="_blank"
href="http://www.facebook.com/sharer.php?u=https://im4change.in/latest-news-updates/question-of-efficacy-leena-menghaney-14576.html"
title="Share on Facebook">
<img src="https://im4change.in/images/Facebook.png?1582080640" alt="share on Facebook" class="ImgBorder"/>
</a><br/>
<a target="_blank"
href="http://twitter.com/share?text=Im4change&url=https://im4change.in/latest-news-updates/question-of-efficacy-leena-menghaney-14576.html"
title="Share on Twitter">
<img src="https://im4change.in/images/twitter.png?1582080632" alt="Twitter" class="ImgBorder"/> </a>
<br/>
<a href="/feeds" title="RSS Feed" target="_blank">
<img src="https://im4change.in/images/rss.png?1582080632" alt="RSS" class="ImgBorder"/>
</a>
<br/>
<a class="feedback-link" id="feedbackFormLink" href="#">
<img src="https://im4change.in/images/feedback.png?1582080630" alt="Feedback" class="ImgBorder"/>
</a> <br/>
<a href="javascript:function iprl5(){var d=document,z=d.createElement('scr'+'ipt'),b=d.body,l=d.location;try{if(!b)throw(0);d.title='(Saving...) '+d.title;z.setAttribute('src',l.protocol+'//www.instapaper.com/j/WKrH3R7ORD5p?u='+encodeURIComponent(l.href)+'&t='+(new Date().getTime()));b.appendChild(z);}catch(e){alert('Please wait until the page has loaded.');}}iprl5();void(0)"
class="bookmarklet" onclick="return explain_bookmarklet();">
<img src="https://im4change.in/images/read-it-later.png?1582080632" alt="Read Later" class="ImgBorder"/> </a>
</div>
<!-- Feedback form Starts here -->
<div id="feedbackForm" class="overlay_form" class="ImgBorder">
<h2>Contact Form</h2>
<div id="contactform1">
<div id="formleft">
<form id="submitform" action="/contactus.php" method="post">
<input type="hidden" name="submitform" value="submitform"/>
<input type="hidden" name="salt_key" value="a0e0f2c6a0644a70e57ad2c96829709a"/>
<input type="hidden" name="ref" value="feedback"/>
<fieldset>
<label>Name :</label>
<input type="text" name="name" class="tbox" required/>
</fieldset>
<fieldset>
<label>Email :</label>
<input type="text" name="email" class="tbox" required/>
</fieldset>
<fieldset>
<label>Message :</label>
<textarea rows="5" cols="20" name="message" required></textarea>
</fieldset>
<fieldset>
Please enter security code
<div class="clear"></div>
<input type="text" name="vrcode" class="tbox"/>
</fieldset>
<fieldset>
<input type="submit" class="button" value="Submit"/>
<a href="#" id="closefeedbakcformLink">Close</a>
</fieldset>
</form>
</div>
<div class="clearfix"></div>
</div>
</div>
<div id="donate_popup" class="modal" style="max-width: 800px;">
<table width="100%" border="1">
<tr>
<td colspan="2" align="center">
<b>Support im4change</b>
</td>
</tr>
<tr>
<td width="25%" valign="middle">
<img src="https://im4change.in/images/logo2.jpg?1582080632" alt="" width="100%"/> </td>
<td style="padding-left:10px;padding-top:10px;">
<form action="https://im4change.in/donate" method="get">
<table width="100%" cellpadding="2" cellspacing="2">
<tr>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
10
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
100
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
1000
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
50
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
500
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
<input type="text" name="price" placeholder="?" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td colspan="3" align="right">
<input type="button" name="Pay" value="Pay"
style="width: 200px;background-color: rgb(205, 35, 36);color: #ffffff;"/>
</td>
</tr>
</table>
</form>
</td>
</tr>
</table>
</div><script type='text/javascript'>
/* <![CDATA[ */
var tievar = {'go_to': 'Go to...'};
/* ]]> */
</script>
<script src="/js/tie-scripts.js?1575549704"></script><script src="/js/bootstrap.js?1575549704"></script><script src="/js/jquery.modal.min.js?1578284310"></script><script>
$(document).ready(function() {
// tell the autocomplete function to get its data from our php script
$('#s').autocomplete({
source: "/autocomplete"
});
});
</script>
<script src="/vj-main-sw-register.js" async></script>
<script>function init(){var imgDefer=document.getElementsByTagName('img');for(var i=0;i<imgDefer.length;i++){if(imgDefer[i].getAttribute('data-src')){imgDefer[i].setAttribute('src',imgDefer[i].getAttribute('data-src'))}}}
window.onload=init;</script>
</body>
</html>'
}
$reasonPhrase = 'OK'
header - [internal], line ??
Cake\Http\ResponseEmitter::emitStatusLine() - CORE/src/Http/ResponseEmitter.php, line 148
Cake\Http\ResponseEmitter::emit() - CORE/src/Http/ResponseEmitter.php, line 54
Cake\Http\Server::emit() - CORE/src/Http/Server.php, line 141
[main] - ROOT/webroot/index.php, line 39
Warning (2): Cannot modify header information - headers already sent by (output started at /home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php:853) [CORE/src/Http/ResponseEmitter.php, line 181]
$response = object(Cake\Http\Response) {
'status' => (int) 200,
'contentType' => 'text/html',
'headers' => [
'Content-Type' => [
[maximum depth reached]
]
],
'file' => null,
'fileRange' => [],
'cookies' => object(Cake\Http\Cookie\CookieCollection) {},
'cacheDirectives' => [],
'body' => '<!DOCTYPE html>
<!--[if lt IE 7 ]>
<html class="ie ie6" lang='en'> <![endif]-->
<!--[if IE 7 ]>
<html class="ie ie7" lang='en'> <![endif]-->
<!--[if IE 8 ]>
<html class="ie ie8" lang='en'> <![endif]-->
<!--[if (gte IE 9)|!(IE)]><!-->
<html lang='en'>
<!--<![endif]-->
<head><meta http-equiv="Content-Type" content="text/html; charset=utf-8">
<title>
LATEST NEWS UPDATES | Question of efficacy -Leena Menghaney </title>
<meta name="description" content="
The country is clearly shaping its legislation to promote access to medicines by fostering generic production.
INDIA'S approach to the revision of its Patents Act in 2005 is a clear example of a country shaping its legislation to promote access..."/>
<meta name="keywords" content="Health,patents,medicines"/>
<meta name="news_keywords" content="Health,patents,medicines">
<link rel="alternate" type="application/rss+xml" title="ROR" href="/ror.xml"/>
<link rel="alternate" type="application/rss+xml" title="RSS 2.0" href="/feeds/"/>
<link rel="stylesheet" href="/css/bootstrap.min.css?1697864993"/> <link rel="stylesheet" href="/css/style.css?v=1.1.2"/> <link rel="stylesheet" href="/css/style-inner.css?1577045210"/> <link rel="stylesheet" id="Oswald-css"
href="https://fonts.googleapis.com/css?family=Oswald%3Aregular%2C700&ver=3.8.1" type="text/css"
media="all">
<link rel="stylesheet" href="/css/jquery.modal.min.css?1578285302"/> <script src="/js/jquery-1.10.2.js?1575549704"></script> <script src="/js/jquery-migrate.min.js?1575549704"></script> <link rel="shortcut icon" href="/favicon.ico" title="Favicon">
<link rel="stylesheet" href="/css/jquery-ui.css?1580720609"/> <script src="/js/jquery-ui.js?1575549704"></script> <link rel="preload" as="style" href="https://www.im4change.org/css/custom.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery.modal.min.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery-ui.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/li-scroller.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<!-- <link rel="preload" as="style" href="https://www.im4change.org/css/style.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous"> -->
<link rel="preload" as="style" href="https://www.im4change.org/css/style-inner.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel='dns-prefetch' href="//im4change.org/css/custom.css" crossorigin >
<link rel="preload" as="script" href="https://www.im4change.org/js/bootstrap.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.li-scroller.1.0.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.modal.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.ui.totop.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-1.10.2.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-migrate.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-ui.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/setting.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/tie-scripts.js">
<!--[if IE]>
<script type="text/javascript">jQuery(document).ready(function () {
jQuery(".menu-item").has("ul").children("a").attr("aria-haspopup", "true");
});</script>
<![endif]-->
<!--[if lt IE 9]>
<script src="/js/html5.js"></script>
<script src="/js/selectivizr-min.js"></script>
<![endif]-->
<!--[if IE 8]>
<link rel="stylesheet" type="text/css" media="all" href="/css/ie8.css"/>
<![endif]-->
<meta property="og:title" content="LATEST NEWS UPDATES | Question of efficacy -Leena Menghaney" />
<meta property="og:url" content="https://im4change.in/latest-news-updates/question-of-efficacy-leena-menghaney-14576.html" />
<meta property="og:type" content="article" />
<meta property="og:description" content="
The country is clearly shaping its legislation to promote access to medicines by fostering generic production.
INDIA'S approach to the revision of its Patents Act in 2005 is a clear example of a country shaping its legislation to promote access..." />
<meta property="og:image" content="" />
<meta property="fb:app_id" content="0" />
<meta name="viewport" content="width=device-width, initial-scale=1, maximum-scale=1, user-scalable=no">
<link rel="apple-touch-icon-precomposed" sizes="144x144" href="https://im4change.in/images/apple1.png">
<link rel="apple-touch-icon-precomposed" sizes="120x120" href="https://im4change.in/images/apple2.png">
<link rel="apple-touch-icon-precomposed" sizes="72x72" href="https://im4change.in/images/apple3.png">
<link rel="apple-touch-icon-precomposed" href="https://im4change.in/images/apple4.png">
<style>
.gsc-results-wrapper-overlay{
top: 38% !important;
height: 50% !important;
}
.gsc-search-button-v2{
border-color: #035588 !important;
background-color: #035588 !important;
}
.gsib_a{
height: 30px !important;
padding: 2px 8px 1px 6px !important;
}
.gsc-search-button-v2{
height: 41px !important;
}
input.gsc-input{
background: none !important;
}
@media only screen and (max-width: 600px) {
.gsc-results-wrapper-overlay{
top: 11% !important;
width: 87% !important;
left: 9% !important;
height: 43% !important;
}
.gsc-search-button-v2{
padding: 10px 10px !important;
}
.gsc-input-box{
height: 28px !important;
}
/* .gsib_a {
padding: 0px 9px 4px 9px !important;
}*/
}
@media only screen and (min-width: 1200px) and (max-width: 1920px) {
table.gsc-search-box{
width: 15% !important;
float: right !important;
margin-top: -118px !important;
}
.gsc-search-button-v2 {
padding: 6px !important;
}
}
</style>
<script>
$(function () {
$("#accordion").accordion({
event: "click hoverintent"
});
});
/*
* hoverIntent | Copyright 2011 Brian Cherne
* http://cherne.net/brian/resources/jquery.hoverIntent.html
* modified by the jQuery UI team
*/
$.event.special.hoverintent = {
setup: function () {
$(this).bind("mouseover", jQuery.event.special.hoverintent.handler);
},
teardown: function () {
$(this).unbind("mouseover", jQuery.event.special.hoverintent.handler);
},
handler: function (event) {
var currentX, currentY, timeout,
args = arguments,
target = $(event.target),
previousX = event.pageX,
previousY = event.pageY;
function track(event) {
currentX = event.pageX;
currentY = event.pageY;
}
;
function clear() {
target
.unbind("mousemove", track)
.unbind("mouseout", clear);
clearTimeout(timeout);
}
function handler() {
var prop,
orig = event;
if ((Math.abs(previousX - currentX) +
Math.abs(previousY - currentY)) < 7) {
clear();
event = $.Event("hoverintent");
for (prop in orig) {
if (!(prop in event)) {
event[prop] = orig[prop];
}
}
// Prevent accessing the original event since the new event
// is fired asynchronously and the old event is no longer
// usable (#6028)
delete event.originalEvent;
target.trigger(event);
} else {
previousX = currentX;
previousY = currentY;
timeout = setTimeout(handler, 100);
}
}
timeout = setTimeout(handler, 100);
target.bind({
mousemove: track,
mouseout: clear
});
}
};
</script>
<script type="text/javascript">
var _gaq = _gaq || [];
_gaq.push(['_setAccount', 'UA-472075-3']);
_gaq.push(['_trackPageview']);
(function () {
var ga = document.createElement('script');
ga.type = 'text/javascript';
ga.async = true;
ga.src = ('https:' == document.location.protocol ? 'https://ssl' : 'http://www') + '.google-analytics.com/ga.js';
var s = document.getElementsByTagName('script')[0];
s.parentNode.insertBefore(ga, s);
})();
</script>
<link rel="stylesheet" href="/css/custom.css?v=1.16"/> <script src="/js/jquery.ui.totop.js?1575549704"></script> <script src="/js/setting.js?1575549704"></script> <link rel="manifest" href="/manifest.json">
<meta name="theme-color" content="#616163" />
<meta name="apple-mobile-web-app-capable" content="yes">
<meta name="apple-mobile-web-app-status-bar-style" content="black">
<meta name="apple-mobile-web-app-title" content="im4change">
<link rel="apple-touch-icon" href="/icons/logo-192x192.png">
</head>
<body id="top" class="home inner blog">
<div class="background-cover"></div>
<div class="wrapper animated">
<header id="theme-header" class="header_inner" style="position: relative;">
<div class="logo inner_logo" style="left:20px !important">
<a title="Home" href="https://im4change.in/">
<img src="https://im4change.in/images/logo2.jpg?1582080632" class="logo_image" alt="im4change"/> </a>
</div>
<div class="langhindi" style="color: #000;display:none;"
href="https://im4change.in/">
<a class="more-link" href="https://im4change.in/">Home</a>
<a href="https://im4change.in/hindi/" class="langbutton ">हिन्दी</a>
</div>
<nav class="fade-in animated2" id="main-nav">
<div class="container">
<div class="main-menu">
<ul class="menu" id="menu-main">
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
style="left: -40px;"><a
target="_blank" href="https://im4change.in/">Home</a>
</li>
<li class="menu-item mega-menu menu-item-type-taxonomy mega-menu menu-item-object-category mega-menu menu-item-has-children parent-list"
style=" margin-left: -40px;"><a href="#">KNOWLEDGE GATEWAY <span class="sub-indicator"></span>
</a>
<div class="mega-menu-block background_menu" style="padding-top:25px;">
<div class="container">
<div class="mega-menu-content">
<div class="mega-menu-item">
<h3><b>Farm Crisis</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/farmers039-suicides-14.html"
class="left postionrel">Farm Suicides </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/unemployment-30.html"
class="left postionrel">Unemployment </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/rural-distress-70.html"
class="left postionrel">Rural distress </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/migration-34.html"
class="left postionrel">Migration </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/key-facts-72.html"
class="left postionrel">Key Facts </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/debt-trap-15.html"
class="left postionrel">Debt Trap </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Empowerment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/union-budget-73.html"
class="left postionrel">Union Budget And Other Economic Policies </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/forest-and-tribal-rights-61.html"
class="left postionrel">Forest and Tribal Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-education-60.html"
class="left postionrel">Right to Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-food-59.html"
class="left postionrel">Right to Food </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/displacement-3279.html"
class="left postionrel">Displacement </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-work-mg-nrega-39.html"
class="left postionrel">Right to Work (MG-NREGA) </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/gender-3280.html"
class="left postionrel">GENDER </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-information-58.html"
class="left postionrel">Right to Information </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/social-audit-48.html"
class="left postionrel">Social Audit </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Hunger / HDI</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/poverty-and-inequality-20499.html"
class="left postionrel">Poverty and inequality </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/malnutrition-41.html"
class="left postionrel">Malnutrition </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/public-health-51.html"
class="left postionrel">Public Health </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/education-50.html"
class="left postionrel">Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hunger-overview-40.html"
class="left postionrel">Hunger Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hdi-overview-45.html"
class="left postionrel">HDI Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/pds-ration-food-security-42.html"
class="left postionrel">PDS/ Ration/ Food Security </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/sdgs-113.html"
class="left postionrel">SDGs </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/mid-day-meal-scheme-mdms-53.html"
class="left postionrel">Mid Day Meal Scheme (MDMS) </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Environment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/time-bomb-ticking-52.html"
class="left postionrel">Time Bomb Ticking </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/water-and-sanitation-55.html"
class="left postionrel">Water and Sanitation </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/impact-on-agriculture-54.html"
class="left postionrel">Impact on Agriculture </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Law & Justice</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/social-justice-20500.html"
class="left postionrel">Social Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/access-to-justice-47.html"
class="left postionrel">Access to Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/human-rights-56.html"
class="left postionrel">Human Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/corruption-35.html"
class="left postionrel">Corruption </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/general-insecurity-46.html"
class="left postionrel">General Insecurity </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/disaster-relief-49.html"
class="left postionrel">Disaster & Relief </a>
</p>
</div>
</div>
</div>
</div>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page "><a target="_blank" href="https://im4change.in/nceus_reports.php">NCEUS reports</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children parent-list ">
<a target="_blank" href="https://im4change.in/about-us-9.html">About Us <span
class="sub-indicator"></span></a>
<ul class="sub-menu aboutmenu">
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/objectives-8.html">Objectives</a>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/contactus.php">Contact
Us</a></li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/about-us-9.html">About
Us</a></li>
</ul>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children ">
<a target="_blank" href="https://im4change.in/fellowships.php" title="Fellowships">Fellowships</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/media-workshops.php">Workshops</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/research.php">Research</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/links-64">Partners</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
id="menu-item-539"><a target="_blank" href="https://im4change.in/hindi/"
class="langbutton langlinkfont17">हिन्दी</a></li>
</ul>
</div> </div>
<!-- <div style="float: right;">
<script async src="https://cse.google.com/cse.js?cx=18b4f2e0f11bed3dd"></script>
<div class="gcse-search"></div>
</div> -->
<div class="search-block" style=" margin-left: 8px; margin-right: 7px;">
<form method="get" id="searchform" name="searchform"
action="https://im4change.in/search"
onsubmit="return searchvalidate();">
<button class="search-button" type="submit" value="Search"></button>
<input type="text" id="s" name="qryStr" value=""
onfocus="if (this.value == 'Search...') {this.value = '';}"
onblur="if (this.value == '') {this.value = 'Search...';}">
</form>
</div>
</nav>
</header>
<div class="container">
<div id="main-content" class=" main1 container fade-in animated3 sidebar-narrow-left">
<div class="content-wrap">
<div class="content" style="width: 900px;min-height: 500px;">
<section class="cat-box recent-box innerCatRecent">
<h1 class="cat-box-title">Question of efficacy -Leena Menghaney</h1>
<a href="JavaScript:void(0);" onclick="return shareArticle(14452);">
<img src="https://im4change.in/images/email.png?1582080630" border="0" width="24" align="right" alt="Share this article"/> </a>
<a href="https://im4change.in/latest-news-updates/question-of-efficacy-leena-menghaney-14576/print"
rel="nofollow">
<img src="https://im4change.in/images/icon-print.png?1582080630" border="0" width="24" align="right" alt="Share this article"/>
</a>
</section>
<section class="recent-box innerCatRecent">
<small class="pb-1"><span class="dateIcn">
<img src="https://im4change.in/images/published.svg?1582080666" alt="published"/>
Published on</span><span class="text-date"> Apr 20, 2012</span>
<span
class="dateIcn">
<img src="https://im4change.in/images/modified.svg?1582080666" alt="modified"/> Modified on </span><span class="text-date"> Apr 20, 2012</span>
</small>
</section>
<div class="clear"></div>
<div style="padding-top: 10px;">
<div class="innerLineHeight">
<div class="middleContent innerInput latest-news-updates">
<table>
<tr>
<td>
<div>
<br /><div align="justify"><em>The country is clearly shaping its legislation to promote access to medicines by fostering generic production. <br /></em><img src="https://im4change.in/siteadmin/tinymce/uploaded/Patent 1.bmp" alt="Patent 1" /><br />INDIA'S approach to the revision of its Patents Act in 2005 is a clear example of a country shaping its legislation to promote access to medicines by fostering generic production. Although World Trade Organisation (WTO) rules made it mandatory for India to put in place a patent regime for medicines by 2005, nothing obliges developing countries such as India to replicate the patent system of wealthy countries, which involves charging the highest possible price and protecting that price through patent monopolies that extend way beyond 20 years.<br /><br />India has used important flexibilities under international law to include provisions in its domestic patent law not only to reduce the number of secondary patents but also to have a licensing mechanism that kicks in with excessive pricing of patented medicines. The application of these safeguards by the Indian patent office – benefiting patients in India and other developing countries – is increasingly inviting the ire of the multinational pharmaceutical industry and its associations.<br /><br />The Indian government is faced with court cases and the diplomatic offensive that the protectors of the pharmaceutical industry in the United States and the European Union are now launching.<br /><br />In India, the importance of generic (local) production of medicines in fostering competition and reducing prices was first recognised by lawmakers in the Patents Act of 1970, which brought in a legal regime that did not allow product patents on pharmaceuticals. In the following decades, India not only was successful in making drugs affordable but also significantly increased their availability by building domestic capacity to produce essential and life-saving drugs. It also went on to become the “pharmacy of the developing world”, supplying medicines to countries that lacked the capacity and resources to produce the drugs themselves or pay the high prices demanded by originator pharmaceutical companies.<br /><br />The production of more affordable generic medicines in India has been instrumental in driving down the price of AIDS (acquired immune deficiency syndrome) medicines by 99 per cent, and nearly six million people living with HIV have been put on treatment on Indian generic medicines in the past 10 years.<br /><br />In 2005, India was obliged to change its patent law in order to comply with its obligations as a member of the WTO, bringing into effect the TRIPS Agreement. The most significant change was the introduction of product patents for medicines. When framing the new patent legislation in 2005, Parliament sought to ensure that provisions to protect public health and access to medicines were incorporated into it. It, therefore, included explicit legal safeguards and guidance on how the patentability requirements should be applied.<br /><br />In particular, evergreening, a well-known abuse of the patent system where companies seek new monopolies or, alternatively, extend a monopoly by seeking to patent minor changes – such as new uses, new forms and other routine improvements of known medicines – was addressed. Section 3(d) of the Indian Patents Act explicitly allows the broad exclusion from patentability of new uses and new forms of known medicines. In sum, Section 3(d) gave explicit guidance to the Indian patent office on how to weed out patent claims on routine improvements of known medicines and protect the country's capacity to act as a factory for the production and supply of affordable generic medicines.<br /></div><div align="justify"> </div><div align="justify"><em>Legal challenge<br /></em><br />In 2006, in a landmark decision, the Indian patent office rejected Swiss pharmaceutical company Novartis' patent application for the life-saving anti-cancer drug imatinib mesylate. The application for a patent on a beta crystalline salt form of imatinib was rejected on the grounds that it lacked novelty, was obvious, and was un-patentable under Section 3(d) of the Patents Act. In retaliation, Novartis mounted a legal challenge to have Section 3(d) declared unconstitutional. Medecins Sans Frontieres (MSF) launched an international campaign calling on the company to drop the case, attracting close to half a million signatures. In 2007, the Madras High Court rejected Novartis' plea and in 2009 the Intellectual Property Appellate Board (IPAB) rejected its patent application on imatinib mesylate once again.<br /><img src="https://im4change.in/siteadmin/tinymce/uploaded/Patent 2.bmp" alt="Patent 2" /><br />But the company is not backing down. After failing to have Section 3(d) struck down, it is now again seeking to limit its effect. In 2009, Novartis filed a special leave petition in the Supreme Court against India in relation to the patentability criteria to be applied to imatinib mesylate.<br /><br />Under Section 3(d) of the Patents Act, new forms of already known substances cannot be patented if they fail to demonstrate the required degree of efficacy; it requires demonstration of increased efficacy for a medicine to deserve a patent. The interpretation of the definition of “efficacy” is therefore central to this case and to the future of India's role as the pharmacy of the developing world.<br /><br />In 2007, in its constitutional challenge against Section 3(d) before the Madras High Court, Novartis had argued that increased bioavailability of the salt form of imatinib meant increased efficacy, entitling it to a patent. But the High Court clarified that efficacy meant “therapeutic effect in healing a disease”.<br /><br />The IPAB, where appeals for unsuccessful patent applications are heard, subsequently applied this interpretation and held that the salt form of imatinib mesylate did not meet the test of therapeutic efficacy. It, therefore, confirmed the rejection of Novartis's patent application.<br /></div><div align="justify"> </div><div align="justify"><em>High standards crucial for tests in patent law<br /></em><br />Setting high standards for the various tests in the patent legislation, particularly the “efficacy” test of Section 3(d) and the inventive step requirement, leading to fewer patents on new forms of known medicines, is important to safeguard access to affordable generic medicines from India. Novartis has now taken its case to the Supreme Court to argue against the interpretation of “efficacy” in Section 3(d) by the Madras High Court and the IPAB. This case has the potential to severely affect access to affordable essential medicines for millions of people across the developing world. It will determine whether Section 3(d) will continue to ensure that patents are granted only on medicines that are truly new and inventive. Many developing countries rely on affordable medicines produced in India, and such medicines constitute over 80 per cent of the AIDS drugs used in the developing world. MSF is closely following the outcome of this case.<br /><br />Novartis is basing its claim for a patent on the salt of imatinib on the fact that there is a 30 per cent increase in the bioavailability of the drug in this new form. But, according to the guidelines for the examination of pharmaceutical patents developed by the World Health Organisation (WHO) and the International Centre for Trade and Sustainable Development (ICTSD), the selection of a salt of the active ingredient with the purpose to improve bioavailability is known in pharmaceutical science. It is common knowledge in the field that salts result in different solubility and, therefore, in different bioavailability.<br /><br />The final arguments in the case have started. The next date of hearing is set for July 10. If Novartis wins, many other medicines, even those that show no increased therapeutic efficacy, will be patentable in India, and the availability of affordable medicines will be threatened. If the substance is taken out of Section 3(d), abusive “evergreening” practices, where drug companies maintain artificially high prices on medicines well beyond the original patent period by securing fresh patents on minor modifications of existing drugs, will become rampant in the future.<br /><br />If, on the other hand, the high threshold for patentability is upheld, generic production will continue to drive the price of life-saving medicines down. Multinational pharmaceutical companies such as Novartis will find it difficult to argue that routine improvements – such as new forms of existing medicines that result in improved stability, enhanced bioavailability, increased solubility, improved flow properties and lower hygroscopicity – meet the efficacy requirements of Section 3(d). In addition, the improved therapeutic efficacy would have to be supported with actual clinical data that demonstrate this effect.<br /><br />The Supreme Court case is the final act in a legal battle that stretches back over six years between Novartis and the Indian government. The government, hopefully, will argue for a strict interpretation of “efficacy” so that patents on new forms of known medicines – such as the one on the cancer drug imatinib mesylate – are not granted as a matter of routine by the country's patent office. Novartis has lined up very senior and very expensive lawyers, including two former Solicitors General, to argue its case. But there appears to be no information on whether the government has appointed its own top lawyer, the Attorney General, in this case.<br /></div><div align="justify"> </div><div align="justify"><em>Opening the door for compulsory licensing<br /></em><br />In another test case on access to treatment, seven years after India revised its 1970 Patents Act, the Controller General of Patents issued the first-ever compulsory licence (CL) to the Hyderabad-based company Natco to produce an affordable version of a patented anti-cancer medicine (sorafenib tosylate) of the German pharmaceutical company Bayer Corporation, marketed under the brand name of Nexavar. The generic version produced by Natco, which will pay 6 per cent royalty on net sales to Bayer, will be 97 per cent cheaper.<br /><br />The decision was made on the basis of the fact that not only had the patentee, Bayer, failed to price sorafenib tosylate at a level that made it accessible and affordable but it was also unable to ensure that the medicine was available in sufficient and sustainable quantities within India. Bayer has time until mid-June to appeal against the order.<br /><br />Like many other giant drug companies, Bayer defended the inflated cost of sorafenib by specifying the high spending on research and development. However, what it did not highlight was that the United States National Institutes of Health had sponsored almost 70 per cent of the second phase of its clinical trials. Later, this drug was given an “orphan drug” designation by the U.S.' Food and Drug Administration (FDA) for the treatment of renal cell carcinoma, entitling Bayer to 50 per cent tax credits, which further lowered the company's costs for the third and most expensive phase of clinical trials.<br /><br />The CL is quickly being dubbed by pharmaceutical companies such as Novartis as a move that will stifle innovation. Indeed, pharmaceutical companies at present try to recover their investments by charging excessively high prices and protecting their drugs through patent monopolies. However, R&D costs are only a fraction of the profits thus made, and a large part of the profits are spent on brand-building and marketing. In 2011, Bayer spent nearly €9 billion on sales and advertising. In the same period, only €2.9 billion was spent on research.<br /><br />The patent system also has another drawback. Innovation currently fails to address the needs of patients in developing countries.<br /><br />The drug companies also repeatedly warn that measures such as the CL adversely affect the confidence of foreign investors. But a study published in Thailand in 2009 by the Health Intervention and Technology Assessment Program (HITAP) found little evidence of a link between the granting of CLs and the level of foreign direct investment (FDI) in the country.<br /><br />The recently granted CL actually highlights a potentially new patent model that routinely allows low-cost alternatives in lieu of royalty payments, not only helping originators to recoup their development costs but also ensuring that people in developing countries have access to medicines. It is in line with licensing decisions in other jurisdictions. Recently, a U.S. court decided not to prevent a competitor from marketing a medical device used for skin grafts, and instead put in place a system of royalties from the competitor to the patent owner. At the core of this decision was the idea that the public has a right to access innovative health products and this should not be blocked by excessive prices.<br /><br />The Novartis and Bayer cases highlight that the country is entering a new era in which disputes on the public's access to and the affordability of drugs will become more frequent.<br /><br /><em>Leena Menghaney is campaign coordinator of Medecins Sans Frontieres in India and is based in New Delhi. </em><br /></div>
</div>
</td>
</tr>
</table>
</div>
</div>
</div>
<div class="clear"></div>
<br><a href="http://www.frontlineonnet.com/stories/20120504290802200.htm" class="re" target="_blank">Frontline, Volume 29, Issue 08, 21 April-04 May, 2012, http://www.frontlineonnet.com/stories/20120504290802200.htm</a><div class="clear"></div>
<div style="padding-top: 18px;">
<p class="post-tag">Tagged with:
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Health"
title="Health">
Health </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=patents"
title="patents">
patents </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=medicines"
title="medicines">
medicines </a>
</p>
</div>
<div class="clear"></div>
<br><br>
<div class="widget-top">
<h4>Related Articles</h4>
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<ul id="recentcomments">
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/fifth-report-from-gambia-implicates-indian-drug-maker-for-contaminated-syrups-banjot-kaur.html"
title="Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur">
Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-may-have-seen-steepest-dip-in-multidimensional-poverty-among-110-nations-as-per-undp-data-nikhil-rampal.html"
title="India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal">
India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/health-among-top-three-priorities-for-indian-voters-after-jobs-and-education-survey-shows-oliver-heath-jyoti-mishra-louise-tillin-sandhya-venkateswaran.html"
title="Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran">
Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/prevalence-of-zero-food-among-infants-and-young-children-in-india-patterns-of-change-across-the-states-and-union-territories-of-india-1993-2021-the-lancet.html"
title="Prevalence of Zero-Food among infants and young children in India - The Lancet ">
Prevalence of Zero-Food among infants and young children in India - The Lancet </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-s-sustainability-goals-at-risk-because-of-extreme-heatwaves-carbon-copy.html"
title="India's Sustainability Goals at Risk Because of Extreme Heatwaves - Carbon Copy">
India's Sustainability Goals at Risk Because of Extreme Heatwaves - Carbon Copy </a>
</li>
</ul>
</div>
<div class="comment-respond" id="respond">
<a name="commentbox"> </a>
<h3 class="comment-reply-title" id="reply-title">Write Comments</h3>
<form method="post" accept-charset="utf-8" role="form" action="/latest-news-updates/question-of-efficacy-leena-menghaney-14576.html"><div style="display:none;"><input type="hidden" name="_method" value="POST"/></div> <form class="comment-form" id="commentform" method="post" action="#commentbox" onSubmit="return validate()"
name="cmtform">
<input type="hidden" name="cmttype" value="articlecmt"/>
<input type="hidden" name="article_id" value="14452"/>
<p class="comment-notes">Your email address will not be published. Required fields are marked <span
class="required">*</span></p>
<p class="comment-form-author">
<label for="commenterName">Name</label>
<span class="required">*</span>
<input type="text" aria-required="true" size="30"
value=""
name="commenterName" id="commenterName" required="true">
</p>
<p class="comment-form-email">
<label for="commenterEmail">Email</label> <span class="required">*</span>
<input aria-required="true" size="30" name="commenterEmail" id="commenterEmail" type="email"
value=""
required="true">
</p>
<p class="comment-form-contact">
<label for="commenterPh">Contact No.</label>
<input type="text" size="30"
value=""
name="commenterPh" id="commenterPh">
</p>
<p class="comment-form-comment">
<label for="comment">Comment</label>
<textarea aria-required="true" required="true" rows="8" cols="45" name="comment"
id="comment"></textarea>
</p>
<p class="comment-form-comment">
<label for="comment">Type the characters you see in the image below <span class="required">*</span><br><img
class="captchaImg"
src="https://im4change.in/securimage_show_art.php?tk=2001382256" alt="captcha"/>
</label>
</p>
<input type="text" name="vrcode" required="true"/>
<p class="form-submit" style="width: 200px;">
<input type="submit" value="Post Comment" id="submit" name="submit">
</p></form>
</div>
<style>
.ui-widget-content {
height: auto !important;
}
</style>
<div id="share-modal"></div>
<style>
.middleContent a{
background-color: rgba(108,172,228,.2);
}
.middleContent a:hover{
background-color: #418fde;
border-color: #418fde;
color: #000;
}
</style>
<script>
function shareArticle(article_id) {
var options = {
modal: true,
height: 'auto',
width: 600 + 'px'
};
$('#share-modal').html("");
$('#share-modal').load('https://im4change.in/share_article?article_id=' + article_id).dialog(options).dialog('open');
}
function postShare() {
var param = 'article_id=' + $("#article_id").val();
param = param + '&y_name=' + $("#y_name").val();
param = param + '&y_email=' + $("#y_email").val();
param = param + '&f_name=' + $("#f_name").val();
param = param + '&f_email=' + $("#f_email").val();
param = param + '&y_msg=' + $("#y_msg").val();
$.ajax({
type: "POST",
url: 'https://im4change.in/post_share_article',
data: param,
success: function (response) {
$('#share-modal').html("Thank You, Your message posted to ");
}
});
return false;
}
</script> </div>
</div>
<!-- Right Side Section Start -->
<!-- MAP Section START -->
<aside class="sidebar indexMarg">
<div class="ad-cell">
<a href="https://im4change.in/statemap.php" title="">
<img src="https://im4change.in/images/map_new_version.png?1582080666" alt="India State Map" class="indiamap" width="232" height="252"/> </a>
<div class="rightmapbox">
<div id="sideOne" class="docltitle"><a href="https://im4change.in/state-report/india/36" target="_blank">DOCUMENTS/
REPORTS</a></div>
<div id="sideTwo" class="statetitle"><a href="https://im4change.in/states.php"target="_blank">STATE DATA/
HDRs.</a></div>
</div>
<div class="widget widgePadTop"></div>
</div>
</aside>
<!-- MAP Section END -->
<aside class="sidebar sidePadbottom">
<div class="rightsmlbox1" >
<a href="https://im4change.in/knowledge_gateway" target="_blank" style="color: #035588;
font-size: 17px;">
KNOWLEDGE GATEWAY
</a>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/newsletter" target="_blank">
NEWSLETTER
</a>
</p>
</div>
</div>
<div class="rightsmlbox1" style="height: 325px;">
<div>
<p class="rightsmlbox1_title">
Interview with Prof. Ravi Srivastava
</p>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/video/interview-with-prof-ravi-srivastava-on-current-economic-crisis">
<img width="250" height="200" src="/images/interview_video_home.jpg" alt="Interview with Prof. Ravi Srivastava"/>
</a>
<!--
<iframe width="250" height="200" src="https://www.youtube.com/embed/MmaTlntk-wc" frameborder="0" allow="accelerometer; autoplay; encrypted-media; gyroscope; picture-in-picture" allowfullscreen=""></iframe>-->
</p>
<a href="https://im4change.in/videogallery" class="more-link CatArchalAnch1" target="_blank">
More videos
</a>
</div>
</div>
<div class="rightsmlbox1">
<div>
<!--div id="sstory" class="rightboxicons"></div--->
<p class="rightsmlbox1_title"><a href="https://im4change.in/list-success-stories" target="_blank">Success Stories</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/interviews" target="_blank">Interviews</a>
</p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a href="https://www.commoncause.in/page.php?id=10" >Donate</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/marquee"
class="isf_link more-link" title="India Focus?" style="border: 4px solid #fdd922;width: 90%;background-color: #fdd922;text-align: center;color: #000000;font-size:18px" target="_blank">India Focus</a></p> </div>
</div>
<div class="rightsmlbox1" style="height: 104px !important;">
<a href="https://im4change.in/quarterly_reports.php" target="_blank">
Quarterly Reports on Effect of Economic Slowdown on Employment in India (2008 - 2015)
</a>
</div>
<!-- <div class="rightsmlbox1">
<a href="https://play.google.com/store/apps/details?id=com.im4.im4change" target="_blank">
</a></div> -->
<!-- <section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">Most Visited</h2>
</section> -->
<!-- accordion Starts here -->
<!-- <div id="accordion" class="accordMarg">
</div> -->
<!-- accordion ends here -->
<!-- Widget Tag Cloud Starts here -->
<div id="tag_cloud-2" class="widget widget_tag_cloud">
<section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">MOST VISITED TAGS</h2>
</section>
<div class="widget-top wiPdTp">
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<div class="tagcloud">
<a href="https://im4change.in/search?qryStr=Agriculture"
target="_blank" class="tag-link-4 font4">Agriculture</a>
<a href="https://im4change.in/search?qryStr=Food Security"
target="_blank" class="tag-link-4 font4">Food Security</a>
<a href="https://im4change.in/search?qryStr=Law and Justice"
target="_blank" class="tag-link-4 font4">Law and Justice</a>
<a href="https://im4change.in/search?qryStr=Health"
target="_blank" class="tag-link-4 font4">Health</a>
<a href="https://im4change.in/search?qryStr=Right to Food"
target="_blank" class="tag-link-4 font4">Right to Food</a>
<a href="https://im4change.in/search?qryStr=Corruption"
target="_blank" class="tag-link-4 font4">Corruption</a>
<a href="https://im4change.in/search?qryStr=farming"
target="_blank" class="tag-link-4 font4">farming</a>
<a href="https://im4change.in/search?qryStr=Environment"
target="_blank" class="tag-link-4 font4">Environment</a>
<a href="https://im4change.in/search?qryStr=Right to Information"
target="_blank" class="tag-link-4 font4">Right to Information</a>
<a href="https://im4change.in/search?qryStr=NREGS"
target="_blank" class="tag-link-4 font4">NREGS</a>
<a href="https://im4change.in/search?qryStr=Human Rights"
target="_blank" class="tag-link-4 font4">Human Rights</a>
<a href="https://im4change.in/search?qryStr=Governance"
target="_blank" class="tag-link-4 font4">Governance</a>
<a href="https://im4change.in/search?qryStr=PDS"
target="_blank" class="tag-link-4 font4">PDS</a>
<a href="https://im4change.in/search?qryStr=COVID-19"
target="_blank" class="tag-link-4 font4">COVID-19</a>
<a href="https://im4change.in/search?qryStr=Land Acquisition"
target="_blank" class="tag-link-4 font4">Land Acquisition</a>
<a href="https://im4change.in/search?qryStr=mgnrega"
target="_blank" class="tag-link-4 font4">mgnrega</a>
<a href="https://im4change.in/search?qryStr=Farmers"
target="_blank" class="tag-link-4 font4">Farmers</a>
<a href="https://im4change.in/search?qryStr=transparency"
target="_blank" class="tag-link-4 font4">transparency</a>
<a href="https://im4change.in/search?qryStr=Gender"
target="_blank" class="tag-link-4 font4">Gender</a>
<a href="https://im4change.in/search?qryStr=Poverty"
target="_blank" class="tag-link-4 font4">Poverty</a>
<a href="https://im4change.in/search?qryStr=Farm Laws" target="_blank" class="tag-link-4 font4">Farm Laws
</a>
<a href="https://im4change.in/search?qryStr=Citizenship Amendment Act" target="_blank" class="tag-link-4 font4">Citizenship Amendment Act
</a>
<a href="https://im4change.in/search?qryStr=CAA NPR NRIC" target="_blank" class="tag-link-4 font4">CAA NPR NRIC
</a>
<a href="https://im4change.in/search?qryStr=Job Losses" target="_blank" class="tag-link-4 font4">Job Losses
</a>
<a href="https://im4change.in/search?qryStr=Migrant Workers" target="_blank" class="tag-link-4 font4">Migrant Workers
</a>
<a href="https://im4change.in/search?qryStr=Unemployment" target="_blank" class="tag-link-4 font4">Unemployment
</a>
<a href="https://im4change.in/search?qryStr=PMGKAY" target="_blank" class="tag-link-4 font4">PMGKAY
</a>
<a href="https://im4change.in/search?qryStr=PM-KISAN" target="_blank" class="tag-link-4 font4">PM-KISAN
</a>
<a href="https://im4change.in/search?qryStr=PM-CARES" target="_blank" class="tag-link-4 font4">PM-CARES
</a>
<a href="https://im4change.in/search?qryStr=LFPR" target="_blank" class="tag-link-4 font4">LFPR
</a>
</div>
</div>
</div>
<!-- Widget Tag Cloud Ends here -->
</aside>
<!-- Right Side Section End -->
</div>
<section class="cat-box cats-review-box footerSec">
<h2 class="cat-box-title vSec CatArcha">Video
Archives</h2>
<h2 class="cat-box-title CatArchaTitle">Archives</h2>
<div class="cat-box-content">
<div class="reviews-cat">
<div class="CatArchaDiv1">
<div class="CatArchaDiv2">
<ul>
<li>
<a href="https://im4change.in/news-alerts-57/moving-upstream-luni-fellowship.html" target="_blank">
Moving Upstream: Luni – Fellowship </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/135-million-indians-exited-multidimensional-poverty-as-per-government-figures-is-that-the-same-as-poverty-reduction.html" target="_blank">
135 Million Indians Exited “Multidimensional" Poverty as per Government... </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/explainer-why-are-tomato-prices-on-fire.html" target="_blank">
Explainer: Why are Tomato Prices on Fire? </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/nsso-survey-only-39-1-of-all-households-have-drinking-water-within-dwelling-46-7-of-rural-households-use-firewood-for-cooking.html" target="_blank">
NSSO Survey: Only 39.1% of all Households have Drinking... </a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/news-alerts-57"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/I51LYnP8BOk/1.jpg"
alt=" Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Short-Video-on-im4change-Hindi-website-Inclusive-Media-for-Change" target="_blank">
Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/kNqha-SwfIY/1.jpg"
alt=" "Session 1: Scope of IDEA and AgriStack" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-1- Scope-of-IDEA-and-AgriStack-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 1: Scope of IDEA and AgriStack" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/6kIVjlgZItk/1.jpg"
alt=" "Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-2-Farmer-Centric-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/2BeHTu0y7xc/1.jpg"
alt=" "Session 3: Future of Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-3-Future-of-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 3: Future of Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="divWidth">
<ul class="divWidthMarg">
<li>
<a href="https://im4change.in/video/Public-Spending-on-Agriculture-in-India-Source-Foundation-for-Agrarian-Studies"
title="Public Spending on Agriculture in India (Source: Foundation for Agrarian Studies)" target="_blank">
Public Spending on Agriculture in India (Source: Foundation for...</a>
</li>
<li>
<a href="https://im4change.in/video/Agrarian-Change-Seminar-Protests-against-the-New-Farm-Laws-in-India-by-Prof-Vikas-Rawal-JNU-Source-Journal-Of-Agrarian-Change"
title="Agrarian Change Seminar: 'Protests against the New Farm Laws in India' by Prof. Vikas Rawal, JNU (Source: Journal Of Agrarian Change) " target="_blank">
Agrarian Change Seminar: 'Protests against the New Farm Laws...</a>
</li>
<li>
<a href="https://im4change.in/video/Webinar-Ramrao-The-Story-of-India-Farm-Crisis-Source-Azim-Premji-University"
title="Webinar: Ramrao - The Story of India's Farm Crisis (Source: Azim Premji University)" target="_blank">
Webinar: Ramrao - The Story of India's Farm Crisis...</a>
</li>
<li>
<a href="https://im4change.in/video/water-and-agricultural-transformation-in-India"
title="Water and Agricultural Transformation in India: A Symbiotic Relationship (Source: IGIDR)" target="_blank">
Water and Agricultural Transformation in India: A Symbiotic Relationship...</a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/videogallery"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
</div>
</div>
</div>
</section> </div>
<div class="clear"></div>
<!-- Footer option Starts here -->
<div class="footer-bottom fade-in animated4">
<div class="container">
<div class="social-icons icon_flat">
<p class="SocialMargTop"> Website Developed by <a target="_blank" title="Web Development"
class="wot right"
href="http://www.ravinderkhurana.com/" rel="nofollow">
RAVINDErkHURANA.com</a></p>
</div>
<div class="alignleft">
<a
target="_blank" href="https://im4change.in/objectives-8.html"
class="link"
title="Objectives">Objectives</a> | <a
target="_blank" href="https://im4change.in/about-us-9.html"
class="link" title="About Us">About Us</a> | <a
target="_blank" href="https://im4change.in/media-workshops.php"
class="ucwords">Workshops</a> | <a
target="_blank" href="https://im4change.in/disclaimer/disclaimer-149.html"
title="Disclaimer">Disclaimer</a> </div>
</div>
</div>
<!-- Footer option ends here -->
</div>
<div id="connect">
<a target="_blank"
href="http://www.facebook.com/sharer.php?u=https://im4change.in/latest-news-updates/question-of-efficacy-leena-menghaney-14576.html"
title="Share on Facebook">
<img src="https://im4change.in/images/Facebook.png?1582080640" alt="share on Facebook" class="ImgBorder"/>
</a><br/>
<a target="_blank"
href="http://twitter.com/share?text=Im4change&url=https://im4change.in/latest-news-updates/question-of-efficacy-leena-menghaney-14576.html"
title="Share on Twitter">
<img src="https://im4change.in/images/twitter.png?1582080632" alt="Twitter" class="ImgBorder"/> </a>
<br/>
<a href="/feeds" title="RSS Feed" target="_blank">
<img src="https://im4change.in/images/rss.png?1582080632" alt="RSS" class="ImgBorder"/>
</a>
<br/>
<a class="feedback-link" id="feedbackFormLink" href="#">
<img src="https://im4change.in/images/feedback.png?1582080630" alt="Feedback" class="ImgBorder"/>
</a> <br/>
<a href="javascript:function iprl5(){var d=document,z=d.createElement('scr'+'ipt'),b=d.body,l=d.location;try{if(!b)throw(0);d.title='(Saving...) '+d.title;z.setAttribute('src',l.protocol+'//www.instapaper.com/j/WKrH3R7ORD5p?u='+encodeURIComponent(l.href)+'&t='+(new Date().getTime()));b.appendChild(z);}catch(e){alert('Please wait until the page has loaded.');}}iprl5();void(0)"
class="bookmarklet" onclick="return explain_bookmarklet();">
<img src="https://im4change.in/images/read-it-later.png?1582080632" alt="Read Later" class="ImgBorder"/> </a>
</div>
<!-- Feedback form Starts here -->
<div id="feedbackForm" class="overlay_form" class="ImgBorder">
<h2>Contact Form</h2>
<div id="contactform1">
<div id="formleft">
<form id="submitform" action="/contactus.php" method="post">
<input type="hidden" name="submitform" value="submitform"/>
<input type="hidden" name="salt_key" value="a0e0f2c6a0644a70e57ad2c96829709a"/>
<input type="hidden" name="ref" value="feedback"/>
<fieldset>
<label>Name :</label>
<input type="text" name="name" class="tbox" required/>
</fieldset>
<fieldset>
<label>Email :</label>
<input type="text" name="email" class="tbox" required/>
</fieldset>
<fieldset>
<label>Message :</label>
<textarea rows="5" cols="20" name="message" required></textarea>
</fieldset>
<fieldset>
Please enter security code
<div class="clear"></div>
<input type="text" name="vrcode" class="tbox"/>
</fieldset>
<fieldset>
<input type="submit" class="button" value="Submit"/>
<a href="#" id="closefeedbakcformLink">Close</a>
</fieldset>
</form>
</div>
<div class="clearfix"></div>
</div>
</div>
<div id="donate_popup" class="modal" style="max-width: 800px;">
<table width="100%" border="1">
<tr>
<td colspan="2" align="center">
<b>Support im4change</b>
</td>
</tr>
<tr>
<td width="25%" valign="middle">
<img src="https://im4change.in/images/logo2.jpg?1582080632" alt="" width="100%"/> </td>
<td style="padding-left:10px;padding-top:10px;">
<form action="https://im4change.in/donate" method="get">
<table width="100%" cellpadding="2" cellspacing="2">
<tr>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
10
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
100
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
1000
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
50
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
500
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
<input type="text" name="price" placeholder="?" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td colspan="3" align="right">
<input type="button" name="Pay" value="Pay"
style="width: 200px;background-color: rgb(205, 35, 36);color: #ffffff;"/>
</td>
</tr>
</table>
</form>
</td>
</tr>
</table>
</div><script type='text/javascript'>
/* <![CDATA[ */
var tievar = {'go_to': 'Go to...'};
/* ]]> */
</script>
<script src="/js/tie-scripts.js?1575549704"></script><script src="/js/bootstrap.js?1575549704"></script><script src="/js/jquery.modal.min.js?1578284310"></script><script>
$(document).ready(function() {
// tell the autocomplete function to get its data from our php script
$('#s').autocomplete({
source: "/autocomplete"
});
});
</script>
<script src="/vj-main-sw-register.js" async></script>
<script>function init(){var imgDefer=document.getElementsByTagName('img');for(var i=0;i<imgDefer.length;i++){if(imgDefer[i].getAttribute('data-src')){imgDefer[i].setAttribute('src',imgDefer[i].getAttribute('data-src'))}}}
window.onload=init;</script>
</body>
</html>'
}
$cookies = []
$values = [
(int) 0 => 'text/html; charset=UTF-8'
]
$name = 'Content-Type'
$first = true
$value = 'text/html; charset=UTF-8'
header - [internal], line ??
Cake\Http\ResponseEmitter::emitHeaders() - CORE/src/Http/ResponseEmitter.php, line 181
Cake\Http\ResponseEmitter::emit() - CORE/src/Http/ResponseEmitter.php, line 55
Cake\Http\Server::emit() - CORE/src/Http/Server.php, line 141
[main] - ROOT/webroot/index.php, line 39
LATEST NEWS UPDATES | Question of efficacy -Leena Menghaney
Published on Apr 20, 2012 Modified on Apr 20, 2012
The country is clearly shaping its legislation to promote access to medicines by fostering generic production. INDIA'S approach to the revision of its Patents Act in 2005 is a clear example of a country shaping its legislation to promote access to medicines by fostering generic production. Although World Trade Organisation (WTO) rules made it mandatory for India to put in place a patent regime for medicines by 2005, nothing obliges developing countries such as India to replicate the patent system of wealthy countries, which involves charging the highest possible price and protecting that price through patent monopolies that extend way beyond 20 years.
India has used important flexibilities under international law to include provisions in its domestic patent law not only to reduce the number of secondary patents but also to have a licensing mechanism that kicks in with excessive pricing of patented medicines. The application of these safeguards by the Indian patent office – benefiting patients in India and other developing countries – is increasingly inviting the ire of the multinational pharmaceutical industry and its associations.
The Indian government is faced with court cases and the diplomatic offensive that the protectors of the pharmaceutical industry in the United States and the European Union are now launching.
In India, the importance of generic (local) production of medicines in fostering competition and reducing prices was first recognised by lawmakers in the Patents Act of 1970, which brought in a legal regime that did not allow product patents on pharmaceuticals. In the following decades, India not only was successful in making drugs affordable but also significantly increased their availability by building domestic capacity to produce essential and life-saving drugs. It also went on to become the “pharmacy of the developing world”, supplying medicines to countries that lacked the capacity and resources to produce the drugs themselves or pay the high prices demanded by originator pharmaceutical companies.
The production of more affordable generic medicines in India has been instrumental in driving down the price of AIDS (acquired immune deficiency syndrome) medicines by 99 per cent, and nearly six million people living with HIV have been put on treatment on Indian generic medicines in the past 10 years.
In 2005, India was obliged to change its patent law in order to comply with its obligations as a member of the WTO, bringing into effect the TRIPS Agreement. The most significant change was the introduction of product patents for medicines. When framing the new patent legislation in 2005, Parliament sought to ensure that provisions to protect public health and access to medicines were incorporated into it. It, therefore, included explicit legal safeguards and guidance on how the patentability requirements should be applied.
In particular, evergreening, a well-known abuse of the patent system where companies seek new monopolies or, alternatively, extend a monopoly by seeking to patent minor changes – such as new uses, new forms and other routine improvements of known medicines – was addressed. Section 3(d) of the Indian Patents Act explicitly allows the broad exclusion from patentability of new uses and new forms of known medicines. In sum, Section 3(d) gave explicit guidance to the Indian patent office on how to weed out patent claims on routine improvements of known medicines and protect the country's capacity to act as a factory for the production and supply of affordable generic medicines.
Legal challenge
In 2006, in a landmark decision, the Indian patent office rejected Swiss pharmaceutical company Novartis' patent application for the life-saving anti-cancer drug imatinib mesylate. The application for a patent on a beta crystalline salt form of imatinib was rejected on the grounds that it lacked novelty, was obvious, and was un-patentable under Section 3(d) of the Patents Act. In retaliation, Novartis mounted a legal challenge to have Section 3(d) declared unconstitutional. Medecins Sans Frontieres (MSF) launched an international campaign calling on the company to drop the case, attracting close to half a million signatures. In 2007, the Madras High Court rejected Novartis' plea and in 2009 the Intellectual Property Appellate Board (IPAB) rejected its patent application on imatinib mesylate once again. But the company is not backing down. After failing to have Section 3(d) struck down, it is now again seeking to limit its effect. In 2009, Novartis filed a special leave petition in the Supreme Court against India in relation to the patentability criteria to be applied to imatinib mesylate.
Under Section 3(d) of the Patents Act, new forms of already known substances cannot be patented if they fail to demonstrate the required degree of efficacy; it requires demonstration of increased efficacy for a medicine to deserve a patent. The interpretation of the definition of “efficacy” is therefore central to this case and to the future of India's role as the pharmacy of the developing world.
In 2007, in its constitutional challenge against Section 3(d) before the Madras High Court, Novartis had argued that increased bioavailability of the salt form of imatinib meant increased efficacy, entitling it to a patent. But the High Court clarified that efficacy meant “therapeutic effect in healing a disease”.
The IPAB, where appeals for unsuccessful patent applications are heard, subsequently applied this interpretation and held that the salt form of imatinib mesylate did not meet the test of therapeutic efficacy. It, therefore, confirmed the rejection of Novartis's patent application.
High standards crucial for tests in patent law
Setting high standards for the various tests in the patent legislation, particularly the “efficacy” test of Section 3(d) and the inventive step requirement, leading to fewer patents on new forms of known medicines, is important to safeguard access to affordable generic medicines from India. Novartis has now taken its case to the Supreme Court to argue against the interpretation of “efficacy” in Section 3(d) by the Madras High Court and the IPAB. This case has the potential to severely affect access to affordable essential medicines for millions of people across the developing world. It will determine whether Section 3(d) will continue to ensure that patents are granted only on medicines that are truly new and inventive. Many developing countries rely on affordable medicines produced in India, and such medicines constitute over 80 per cent of the AIDS drugs used in the developing world. MSF is closely following the outcome of this case.
Novartis is basing its claim for a patent on the salt of imatinib on the fact that there is a 30 per cent increase in the bioavailability of the drug in this new form. But, according to the guidelines for the examination of pharmaceutical patents developed by the World Health Organisation (WHO) and the International Centre for Trade and Sustainable Development (ICTSD), the selection of a salt of the active ingredient with the purpose to improve bioavailability is known in pharmaceutical science. It is common knowledge in the field that salts result in different solubility and, therefore, in different bioavailability.
The final arguments in the case have started. The next date of hearing is set for July 10. If Novartis wins, many other medicines, even those that show no increased therapeutic efficacy, will be patentable in India, and the availability of affordable medicines will be threatened. If the substance is taken out of Section 3(d), abusive “evergreening” practices, where drug companies maintain artificially high prices on medicines well beyond the original patent period by securing fresh patents on minor modifications of existing drugs, will become rampant in the future.
If, on the other hand, the high threshold for patentability is upheld, generic production will continue to drive the price of life-saving medicines down. Multinational pharmaceutical companies such as Novartis will find it difficult to argue that routine improvements – such as new forms of existing medicines that result in improved stability, enhanced bioavailability, increased solubility, improved flow properties and lower hygroscopicity – meet the efficacy requirements of Section 3(d). In addition, the improved therapeutic efficacy would have to be supported with actual clinical data that demonstrate this effect.
The Supreme Court case is the final act in a legal battle that stretches back over six years between Novartis and the Indian government. The government, hopefully, will argue for a strict interpretation of “efficacy” so that patents on new forms of known medicines – such as the one on the cancer drug imatinib mesylate – are not granted as a matter of routine by the country's patent office. Novartis has lined up very senior and very expensive lawyers, including two former Solicitors General, to argue its case. But there appears to be no information on whether the government has appointed its own top lawyer, the Attorney General, in this case.
Opening the door for compulsory licensing
In another test case on access to treatment, seven years after India revised its 1970 Patents Act, the Controller General of Patents issued the first-ever compulsory licence (CL) to the Hyderabad-based company Natco to produce an affordable version of a patented anti-cancer medicine (sorafenib tosylate) of the German pharmaceutical company Bayer Corporation, marketed under the brand name of Nexavar. The generic version produced by Natco, which will pay 6 per cent royalty on net sales to Bayer, will be 97 per cent cheaper.
The decision was made on the basis of the fact that not only had the patentee, Bayer, failed to price sorafenib tosylate at a level that made it accessible and affordable but it was also unable to ensure that the medicine was available in sufficient and sustainable quantities within India. Bayer has time until mid-June to appeal against the order.
Like many other giant drug companies, Bayer defended the inflated cost of sorafenib by specifying the high spending on research and development. However, what it did not highlight was that the United States National Institutes of Health had sponsored almost 70 per cent of the second phase of its clinical trials. Later, this drug was given an “orphan drug” designation by the U.S.' Food and Drug Administration (FDA) for the treatment of renal cell carcinoma, entitling Bayer to 50 per cent tax credits, which further lowered the company's costs for the third and most expensive phase of clinical trials.
The CL is quickly being dubbed by pharmaceutical companies such as Novartis as a move that will stifle innovation. Indeed, pharmaceutical companies at present try to recover their investments by charging excessively high prices and protecting their drugs through patent monopolies. However, R&D costs are only a fraction of the profits thus made, and a large part of the profits are spent on brand-building and marketing. In 2011, Bayer spent nearly €9 billion on sales and advertising. In the same period, only €2.9 billion was spent on research.
The patent system also has another drawback. Innovation currently fails to address the needs of patients in developing countries.
The drug companies also repeatedly warn that measures such as the CL adversely affect the confidence of foreign investors. But a study published in Thailand in 2009 by the Health Intervention and Technology Assessment Program (HITAP) found little evidence of a link between the granting of CLs and the level of foreign direct investment (FDI) in the country.
The recently granted CL actually highlights a potentially new patent model that routinely allows low-cost alternatives in lieu of royalty payments, not only helping originators to recoup their development costs but also ensuring that people in developing countries have access to medicines. It is in line with licensing decisions in other jurisdictions. Recently, a U.S. court decided not to prevent a competitor from marketing a medical device used for skin grafts, and instead put in place a system of royalties from the competitor to the patent owner. At the core of this decision was the idea that the public has a right to access innovative health products and this should not be blocked by excessive prices.
The Novartis and Bayer cases highlight that the country is entering a new era in which disputes on the public's access to and the affordability of drugs will become more frequent.
Leena Menghaney is campaign coordinator of Medecins Sans Frontieres in India and is based in New Delhi.
 Published on Apr 20, 2012
Published on Apr 20, 2012
 Modified on Apr 20, 2012
Modified on Apr 20, 2012
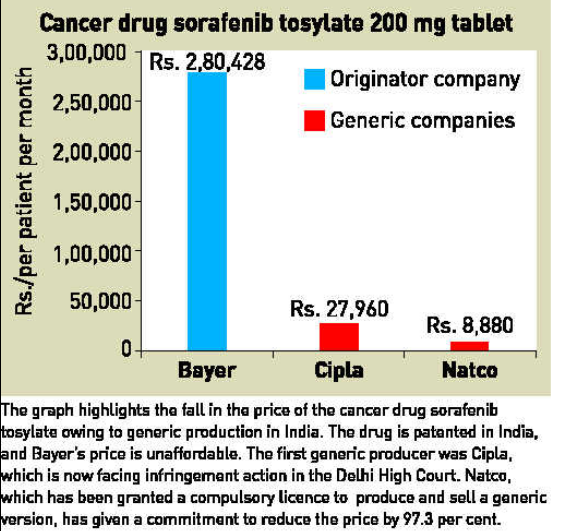
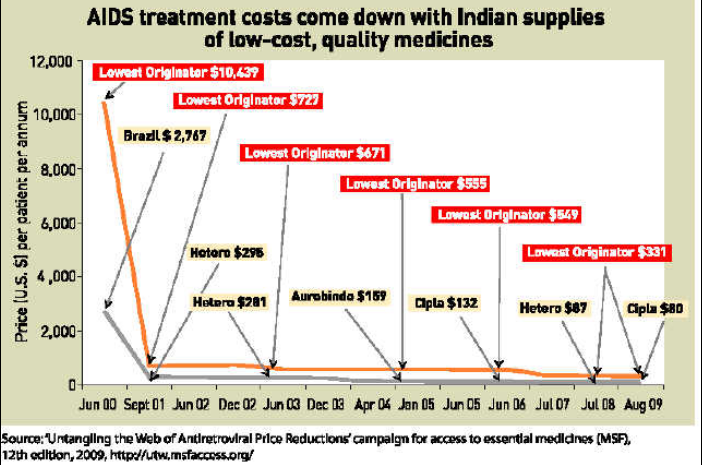









Write Comments