Deprecated (16384): The ArrayAccess methods will be removed in 4.0.0.Use getParam(), getData() and getQuery() instead. - /home/brlfuser/public_html/src/Controller/ArtileDetailController.php, line: 150
You can disable deprecation warnings by setting `Error.errorLevel` to `E_ALL & ~E_USER_DEPRECATED` in your config/app.php. [CORE/src/Core/functions.php, line 311]
deprecationWarning - CORE/src/Core/functions.php, line 311
Cake\Http\ServerRequest::offsetGet() - CORE/src/Http/ServerRequest.php, line 2421
App\Controller\ArtileDetailController::index() - APP/Controller/ArtileDetailController.php, line 150
Cake\Controller\Controller::invokeAction() - CORE/src/Controller/Controller.php, line 610
Cake\Http\ActionDispatcher::_invoke() - CORE/src/Http/ActionDispatcher.php, line 120
Cake\Http\ActionDispatcher::dispatch() - CORE/src/Http/ActionDispatcher.php, line 94
Cake\Http\BaseApplication::__invoke() - CORE/src/Http/BaseApplication.php, line 235
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Routing\Middleware\RoutingMiddleware::__invoke() - CORE/src/Routing/Middleware/RoutingMiddleware.php, line 162
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Routing\Middleware\AssetMiddleware::__invoke() - CORE/src/Routing/Middleware/AssetMiddleware.php, line 97
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Error\Middleware\ErrorHandlerMiddleware::__invoke() - CORE/src/Error/Middleware/ErrorHandlerMiddleware.php, line 96
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Http\Runner::run() - CORE/src/Http/Runner.php, line 51
Cake\Http\Server::run() - CORE/src/Http/Server.php, line 98
Deprecated (16384): The ArrayAccess methods will be removed in 4.0.0.Use getParam(), getData() and getQuery() instead. - /home/brlfuser/public_html/src/Controller/ArtileDetailController.php, line: 151
You can disable deprecation warnings by setting `Error.errorLevel` to `E_ALL & ~E_USER_DEPRECATED` in your config/app.php. [CORE/src/Core/functions.php, line 311]
deprecationWarning - CORE/src/Core/functions.php, line 311
Cake\Http\ServerRequest::offsetGet() - CORE/src/Http/ServerRequest.php, line 2421
App\Controller\ArtileDetailController::index() - APP/Controller/ArtileDetailController.php, line 151
Cake\Controller\Controller::invokeAction() - CORE/src/Controller/Controller.php, line 610
Cake\Http\ActionDispatcher::_invoke() - CORE/src/Http/ActionDispatcher.php, line 120
Cake\Http\ActionDispatcher::dispatch() - CORE/src/Http/ActionDispatcher.php, line 94
Cake\Http\BaseApplication::__invoke() - CORE/src/Http/BaseApplication.php, line 235
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Routing\Middleware\RoutingMiddleware::__invoke() - CORE/src/Routing/Middleware/RoutingMiddleware.php, line 162
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Routing\Middleware\AssetMiddleware::__invoke() - CORE/src/Routing/Middleware/AssetMiddleware.php, line 97
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Error\Middleware\ErrorHandlerMiddleware::__invoke() - CORE/src/Error/Middleware/ErrorHandlerMiddleware.php, line 96
Cake\Http\Runner::__invoke() - CORE/src/Http/Runner.php, line 65
Cake\Http\Runner::run() - CORE/src/Http/Runner.php, line 51
Cake\Http\Server::run() - CORE/src/Http/Server.php, line 98
Warning (512): Unable to emit headers. Headers sent in file=/home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php line=853 [CORE/src/Http/ResponseEmitter.php, line 48]
if (Configure::read('debug')) {
trigger_error($message, E_USER_WARNING);
} else {
$response = object(Cake\Http\Response) {
'status' => (int) 200,
'contentType' => 'text/html',
'headers' => [
'Content-Type' => [
[maximum depth reached]
]
],
'file' => null,
'fileRange' => [],
'cookies' => object(Cake\Http\Cookie\CookieCollection) {},
'cacheDirectives' => [],
'body' => '<!DOCTYPE html>
<!--[if lt IE 7 ]>
<html class="ie ie6" lang='en'> <![endif]-->
<!--[if IE 7 ]>
<html class="ie ie7" lang='en'> <![endif]-->
<!--[if IE 8 ]>
<html class="ie ie8" lang='en'> <![endif]-->
<!--[if (gte IE 9)|!(IE)]><!-->
<html lang='en'>
<!--<![endif]-->
<head><meta http-equiv="Content-Type" content="text/html; charset=utf-8">
<title>
LATEST NEWS UPDATES | Steps to improve Healthcare in Rural India </title>
<meta name="description" content="
-Press Information Bureau (Ministry of Health and Family Welfare)
Healthcare for all, particularly for the rural areas has been a priority for the Government. The health indicators like Infant Mortality Rate (IMR), Total Fertility Rate (TFR), and nutritional status of children..."/>
<meta name="keywords" content="Public Health,Health,infant mortality"/>
<meta name="news_keywords" content="Public Health,Health,infant mortality">
<link rel="alternate" type="application/rss+xml" title="ROR" href="/ror.xml"/>
<link rel="alternate" type="application/rss+xml" title="RSS 2.0" href="/feeds/"/>
<link rel="stylesheet" href="/css/bootstrap.min.css?1697864993"/> <link rel="stylesheet" href="/css/style.css?v=1.1.2"/> <link rel="stylesheet" href="/css/style-inner.css?1577045210"/> <link rel="stylesheet" id="Oswald-css"
href="https://fonts.googleapis.com/css?family=Oswald%3Aregular%2C700&ver=3.8.1" type="text/css"
media="all">
<link rel="stylesheet" href="/css/jquery.modal.min.css?1578285302"/> <script src="/js/jquery-1.10.2.js?1575549704"></script> <script src="/js/jquery-migrate.min.js?1575549704"></script> <link rel="shortcut icon" href="/favicon.ico" title="Favicon">
<link rel="stylesheet" href="/css/jquery-ui.css?1580720609"/> <script src="/js/jquery-ui.js?1575549704"></script> <link rel="preload" as="style" href="https://www.im4change.org/css/custom.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery.modal.min.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery-ui.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/li-scroller.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<!-- <link rel="preload" as="style" href="https://www.im4change.org/css/style.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous"> -->
<link rel="preload" as="style" href="https://www.im4change.org/css/style-inner.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel='dns-prefetch' href="//im4change.org/css/custom.css" crossorigin >
<link rel="preload" as="script" href="https://www.im4change.org/js/bootstrap.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.li-scroller.1.0.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.modal.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.ui.totop.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-1.10.2.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-migrate.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-ui.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/setting.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/tie-scripts.js">
<!--[if IE]>
<script type="text/javascript">jQuery(document).ready(function () {
jQuery(".menu-item").has("ul").children("a").attr("aria-haspopup", "true");
});</script>
<![endif]-->
<!--[if lt IE 9]>
<script src="/js/html5.js"></script>
<script src="/js/selectivizr-min.js"></script>
<![endif]-->
<!--[if IE 8]>
<link rel="stylesheet" type="text/css" media="all" href="/css/ie8.css"/>
<![endif]-->
<meta property="og:title" content="LATEST NEWS UPDATES | Steps to improve Healthcare in Rural India" />
<meta property="og:url" content="https://im4change.in/latest-news-updates/steps-to-improve-healthcare-in-rural-india-24314.html" />
<meta property="og:type" content="article" />
<meta property="og:description" content="
-Press Information Bureau (Ministry of Health and Family Welfare)
Healthcare for all, particularly for the rural areas has been a priority for the Government. The health indicators like Infant Mortality Rate (IMR), Total Fertility Rate (TFR), and nutritional status of children..." />
<meta property="og:image" content="" />
<meta property="fb:app_id" content="0" />
<meta name="viewport" content="width=device-width, initial-scale=1, maximum-scale=1, user-scalable=no">
<link rel="apple-touch-icon-precomposed" sizes="144x144" href="https://im4change.in/images/apple1.png">
<link rel="apple-touch-icon-precomposed" sizes="120x120" href="https://im4change.in/images/apple2.png">
<link rel="apple-touch-icon-precomposed" sizes="72x72" href="https://im4change.in/images/apple3.png">
<link rel="apple-touch-icon-precomposed" href="https://im4change.in/images/apple4.png">
<style>
.gsc-results-wrapper-overlay{
top: 38% !important;
height: 50% !important;
}
.gsc-search-button-v2{
border-color: #035588 !important;
background-color: #035588 !important;
}
.gsib_a{
height: 30px !important;
padding: 2px 8px 1px 6px !important;
}
.gsc-search-button-v2{
height: 41px !important;
}
input.gsc-input{
background: none !important;
}
@media only screen and (max-width: 600px) {
.gsc-results-wrapper-overlay{
top: 11% !important;
width: 87% !important;
left: 9% !important;
height: 43% !important;
}
.gsc-search-button-v2{
padding: 10px 10px !important;
}
.gsc-input-box{
height: 28px !important;
}
/* .gsib_a {
padding: 0px 9px 4px 9px !important;
}*/
}
@media only screen and (min-width: 1200px) and (max-width: 1920px) {
table.gsc-search-box{
width: 15% !important;
float: right !important;
margin-top: -118px !important;
}
.gsc-search-button-v2 {
padding: 6px !important;
}
}
</style>
<script>
$(function () {
$("#accordion").accordion({
event: "click hoverintent"
});
});
/*
* hoverIntent | Copyright 2011 Brian Cherne
* http://cherne.net/brian/resources/jquery.hoverIntent.html
* modified by the jQuery UI team
*/
$.event.special.hoverintent = {
setup: function () {
$(this).bind("mouseover", jQuery.event.special.hoverintent.handler);
},
teardown: function () {
$(this).unbind("mouseover", jQuery.event.special.hoverintent.handler);
},
handler: function (event) {
var currentX, currentY, timeout,
args = arguments,
target = $(event.target),
previousX = event.pageX,
previousY = event.pageY;
function track(event) {
currentX = event.pageX;
currentY = event.pageY;
}
;
function clear() {
target
.unbind("mousemove", track)
.unbind("mouseout", clear);
clearTimeout(timeout);
}
function handler() {
var prop,
orig = event;
if ((Math.abs(previousX - currentX) +
Math.abs(previousY - currentY)) < 7) {
clear();
event = $.Event("hoverintent");
for (prop in orig) {
if (!(prop in event)) {
event[prop] = orig[prop];
}
}
// Prevent accessing the original event since the new event
// is fired asynchronously and the old event is no longer
// usable (#6028)
delete event.originalEvent;
target.trigger(event);
} else {
previousX = currentX;
previousY = currentY;
timeout = setTimeout(handler, 100);
}
}
timeout = setTimeout(handler, 100);
target.bind({
mousemove: track,
mouseout: clear
});
}
};
</script>
<script type="text/javascript">
var _gaq = _gaq || [];
_gaq.push(['_setAccount', 'UA-472075-3']);
_gaq.push(['_trackPageview']);
(function () {
var ga = document.createElement('script');
ga.type = 'text/javascript';
ga.async = true;
ga.src = ('https:' == document.location.protocol ? 'https://ssl' : 'http://www') + '.google-analytics.com/ga.js';
var s = document.getElementsByTagName('script')[0];
s.parentNode.insertBefore(ga, s);
})();
</script>
<link rel="stylesheet" href="/css/custom.css?v=1.16"/> <script src="/js/jquery.ui.totop.js?1575549704"></script> <script src="/js/setting.js?1575549704"></script> <link rel="manifest" href="/manifest.json">
<meta name="theme-color" content="#616163" />
<meta name="apple-mobile-web-app-capable" content="yes">
<meta name="apple-mobile-web-app-status-bar-style" content="black">
<meta name="apple-mobile-web-app-title" content="im4change">
<link rel="apple-touch-icon" href="/icons/logo-192x192.png">
</head>
<body id="top" class="home inner blog">
<div class="background-cover"></div>
<div class="wrapper animated">
<header id="theme-header" class="header_inner" style="position: relative;">
<div class="logo inner_logo" style="left:20px !important">
<a title="Home" href="https://im4change.in/">
<img src="https://im4change.in/images/logo2.jpg?1582080632" class="logo_image" alt="im4change"/> </a>
</div>
<div class="langhindi" style="color: #000;display:none;"
href="https://im4change.in/">
<a class="more-link" href="https://im4change.in/">Home</a>
<a href="https://im4change.in/hindi/" class="langbutton ">हिन्दी</a>
</div>
<nav class="fade-in animated2" id="main-nav">
<div class="container">
<div class="main-menu">
<ul class="menu" id="menu-main">
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
style="left: -40px;"><a
target="_blank" href="https://im4change.in/">Home</a>
</li>
<li class="menu-item mega-menu menu-item-type-taxonomy mega-menu menu-item-object-category mega-menu menu-item-has-children parent-list"
style=" margin-left: -40px;"><a href="#">KNOWLEDGE GATEWAY <span class="sub-indicator"></span>
</a>
<div class="mega-menu-block background_menu" style="padding-top:25px;">
<div class="container">
<div class="mega-menu-content">
<div class="mega-menu-item">
<h3><b>Farm Crisis</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/farmers039-suicides-14.html"
class="left postionrel">Farm Suicides </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/unemployment-30.html"
class="left postionrel">Unemployment </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/rural-distress-70.html"
class="left postionrel">Rural distress </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/migration-34.html"
class="left postionrel">Migration </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/key-facts-72.html"
class="left postionrel">Key Facts </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/debt-trap-15.html"
class="left postionrel">Debt Trap </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Empowerment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/union-budget-73.html"
class="left postionrel">Union Budget And Other Economic Policies </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/forest-and-tribal-rights-61.html"
class="left postionrel">Forest and Tribal Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-education-60.html"
class="left postionrel">Right to Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-food-59.html"
class="left postionrel">Right to Food </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/displacement-3279.html"
class="left postionrel">Displacement </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-work-mg-nrega-39.html"
class="left postionrel">Right to Work (MG-NREGA) </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/gender-3280.html"
class="left postionrel">GENDER </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-information-58.html"
class="left postionrel">Right to Information </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/social-audit-48.html"
class="left postionrel">Social Audit </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Hunger / HDI</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/poverty-and-inequality-20499.html"
class="left postionrel">Poverty and inequality </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/malnutrition-41.html"
class="left postionrel">Malnutrition </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/public-health-51.html"
class="left postionrel">Public Health </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/education-50.html"
class="left postionrel">Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hunger-overview-40.html"
class="left postionrel">Hunger Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hdi-overview-45.html"
class="left postionrel">HDI Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/pds-ration-food-security-42.html"
class="left postionrel">PDS/ Ration/ Food Security </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/sdgs-113.html"
class="left postionrel">SDGs </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/mid-day-meal-scheme-mdms-53.html"
class="left postionrel">Mid Day Meal Scheme (MDMS) </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Environment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/time-bomb-ticking-52.html"
class="left postionrel">Time Bomb Ticking </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/water-and-sanitation-55.html"
class="left postionrel">Water and Sanitation </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/impact-on-agriculture-54.html"
class="left postionrel">Impact on Agriculture </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Law & Justice</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/social-justice-20500.html"
class="left postionrel">Social Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/access-to-justice-47.html"
class="left postionrel">Access to Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/human-rights-56.html"
class="left postionrel">Human Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/corruption-35.html"
class="left postionrel">Corruption </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/general-insecurity-46.html"
class="left postionrel">General Insecurity </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/disaster-relief-49.html"
class="left postionrel">Disaster & Relief </a>
</p>
</div>
</div>
</div>
</div>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page "><a target="_blank" href="https://im4change.in/nceus_reports.php">NCEUS reports</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children parent-list ">
<a target="_blank" href="https://im4change.in/about-us-9.html">About Us <span
class="sub-indicator"></span></a>
<ul class="sub-menu aboutmenu">
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/objectives-8.html">Objectives</a>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/contactus.php">Contact
Us</a></li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/about-us-9.html">About
Us</a></li>
</ul>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children ">
<a target="_blank" href="https://im4change.in/fellowships.php" title="Fellowships">Fellowships</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/media-workshops.php">Workshops</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/research.php">Research</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/links-64">Partners</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
id="menu-item-539"><a target="_blank" href="https://im4change.in/hindi/"
class="langbutton langlinkfont17">हिन्दी</a></li>
</ul>
</div> </div>
<!-- <div style="float: right;">
<script async src="https://cse.google.com/cse.js?cx=18b4f2e0f11bed3dd"></script>
<div class="gcse-search"></div>
</div> -->
<div class="search-block" style=" margin-left: 8px; margin-right: 7px;">
<form method="get" id="searchform" name="searchform"
action="https://im4change.in/search"
onsubmit="return searchvalidate();">
<button class="search-button" type="submit" value="Search"></button>
<input type="text" id="s" name="qryStr" value=""
onfocus="if (this.value == 'Search...') {this.value = '';}"
onblur="if (this.value == '') {this.value = 'Search...';}">
</form>
</div>
</nav>
</header>
<div class="container">
<div id="main-content" class=" main1 container fade-in animated3 sidebar-narrow-left">
<div class="content-wrap">
<div class="content" style="width: 900px;min-height: 500px;">
<section class="cat-box recent-box innerCatRecent">
<h1 class="cat-box-title">Steps to improve Healthcare in Rural India</h1>
<a href="JavaScript:void(0);" onclick="return shareArticle(24141);">
<img src="https://im4change.in/images/email.png?1582080630" border="0" width="24" align="right" alt="Share this article"/> </a>
<a href="https://im4change.in/latest-news-updates/steps-to-improve-healthcare-in-rural-india-24314/print"
rel="nofollow">
<img src="https://im4change.in/images/icon-print.png?1582080630" border="0" width="24" align="right" alt="Share this article"/>
</a>
</section>
<section class="recent-box innerCatRecent">
<small class="pb-1"><span class="dateIcn">
<img src="https://im4change.in/images/published.svg?1582080666" alt="published"/>
Published on</span><span class="text-date"> Feb 21, 2014</span>
<span
class="dateIcn">
<img src="https://im4change.in/images/modified.svg?1582080666" alt="modified"/> Modified on </span><span class="text-date"> Feb 21, 2014</span>
</small>
</section>
<div class="clear"></div>
<div style="padding-top: 10px;">
<div class="innerLineHeight">
<div class="middleContent innerInput latest-news-updates">
<table>
<tr>
<td>
<div>
<div align="justify">-Press Information Bureau (Ministry of Health and Family Welfare)</div><p align="justify"><br />Healthcare for all, particularly for the rural areas has been a priority for the Government. The health indicators like Infant Mortality Rate (IMR), Total Fertility Rate (TFR), and nutritional status of children under 3 years including prevalence of anemia amongst them and pregnant women in rural area are considerably poor as compared to urban areas. The key health indicators are as under:</p><p align="justify"><img src="https://im4change.in/siteadmin/tinymce/uploaded/Health_2.JPG" alt="Health" width="602" height="187" /></p><p align="justify">Public Health is a state subject. However, Central Government launched NRHM in 2005 to provide financial support to the States/UTs to strengthen their health systems particularly to cater to the healthcare needs of rural areas. Key steps taken to improve health care in rural areas include the following:</p><p align="justify"> </p><p align="justify"> i. Support is provided to States/UTs under NRHM, to strengthen the health system including establishment/up-gradation/renovation of health infrastructure, engagement of Nurses, doctors and specialist on contractual basis based on the appraisal of requirements proposed by the States in their Programme Implementation Plans (PIP),</p><p align="justify"> ii. Support under NRHM is also provided by way of additional incentives to serve in remote underserved areas, so that health professionals find it attractive to join public health facilities in such areas. In order to encourage the States to fill up existing vacancies in remote rural areas, the states are being incentivized to ensure rational deployment of health human resource. Manpower deployment is also to be put on the web in public domain,</p><p align="justify"> iii. To increase the availability of doctors, several initiatives have been taken to rationalize the norms in medical education, such as, relaxation in land requirements, bed strength, increase in ceiling for maximum intake for undergraduates, enhancement of teacher-student ratio in Post Graduate Courses, etc., which has resulted in substantial increase in number of undergraduate and post graduate seats. Government has also approved setting up of ANM/GNM Schools in different States besides setting up of Institutes of Paramedical Sciences at National and regional levels,</p><p align="justify"> iv. States/UTs are being impressed upon from time to time to make available improved health facilities including free essential medicines in all public health facilities. Accordingly, financial support is being provided for ensuring uninterrupted supply of free essential medicines in public health facilities based on the requirement proposed by the States in their PIPs. An incentive of upto 5% of the NRHM outlay has also been introduced in 2012-13 for states for establishing policy framework and systems for providing free generic medicines to those who access public health facilities.</p><p align="justify"> v. States/UTs are being provided support for focused attention and greater resources per capita to high priority districts with relatively poor composite health index.</p><p align="justify"> vi. Financial assistance is provided to the States/UTs for selection and training of Accredited Social Health Activists (ASHA), who act as a link between community and healthcare facilities.</p><p align="justify"> vii. States/UTs are supported with Mobile Medical Units for improved service delivery especially in hard to reach areas. There are over 2000 MMUs that are being supported under NRHM. Support is also provided for Emergency Referral Transport services to ensure in-interrupted referral services. There are over 20000 ambulances that are being supported under NRHM.</p><p align="justify">viii. States/UTs are assisted to constitute Village Health, Sanitation and Nutrition Committees so as to ensure community participation and village level planning and monitoring of health activities.</p><p align="justify"> ix. New initiatives such as Janani Shishu Suraksha Karyakram (JSSK), Rashtriya Bal Swashthya Karyrakram (RBSK), Rashtriya Kishore Swashthya Karyakram (RKSK), ‘National Health Mission Free Drugs Service Initiative' etc., have also been introduced to inter-alia make health care affordable by reducing out of pocket expenditure.</p><p align="justify"> </p><p align="justify">Presently, there is no proposal to revise the existing National Health Policy (NHP) - 2002. The Twelfth Plan seeks to strengthen initiatives taken in the Eleventh Plan to expand the reach of health care and work towards the long term objective of establishing a system of Universal Health Coverage (UHC) in the country. This means that each individual would have assured access to a defined essential range of medicines and treatment at an affordable price, which should be entirely free for large percentage of the population. Inevitably, the list of assured services will have to be limited by budgetary constraints. Further, to ensure equitable health care to bring about sharper improvements in health outcomes, at least 25% of all districts in each state have been identified as high priority districts based on a composite health index. These also include all tribal and LWE affected districts which are below the State's average of composite health index. These districts would receive higher per capita funding, enhanced monitoring, focused supportive supervision and have differential planning norms. These measures would help reduce prevailing health inequalities in rural areas.</p><p align="justify"> </p><p align="justify">This was stated by Shri Ghulam Nabi Azad, Union Minister for Health and Family Welfare in a written reply to the Lok Sabha today.</p><p align="justify">*********</p><p align="justify">MV/GM</p><p align="justify">(Release ID :104096)</p>
</div>
</td>
</tr>
</table>
</div>
</div>
</div>
<div class="clear"></div>
<br><a href="http://www.pib.nic.in/newsite/erelease.aspx?relid=0" class="re" target="_blank">Press Information Bureau, 21 February, 2014, http://www.pib.nic.in/newsite/erelease.aspx?relid=0</a><div class="clear"></div>
<div style="padding-top: 18px;">
<p class="post-tag">Tagged with:
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Public Health"
title="Public Health">
Public Health </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Health"
title="Health">
Health </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=infant mortality"
title="infant mortality">
infant mortality </a>
</p>
</div>
<div class="clear"></div>
<br><br>
<div class="widget-top">
<h4>Related Articles</h4>
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<ul id="recentcomments">
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/fifth-report-from-gambia-implicates-indian-drug-maker-for-contaminated-syrups-banjot-kaur.html"
title="Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur">
Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-may-have-seen-steepest-dip-in-multidimensional-poverty-among-110-nations-as-per-undp-data-nikhil-rampal.html"
title="India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal">
India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/health-among-top-three-priorities-for-indian-voters-after-jobs-and-education-survey-shows-oliver-heath-jyoti-mishra-louise-tillin-sandhya-venkateswaran.html"
title="Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran">
Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/prevalence-of-zero-food-among-infants-and-young-children-in-india-patterns-of-change-across-the-states-and-union-territories-of-india-1993-2021-the-lancet.html"
title="Prevalence of Zero-Food among infants and young children in India - The Lancet ">
Prevalence of Zero-Food among infants and young children in India - The Lancet </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-s-sustainability-goals-at-risk-because-of-extreme-heatwaves-carbon-copy.html"
title="India's Sustainability Goals at Risk Because of Extreme Heatwaves - Carbon Copy">
India's Sustainability Goals at Risk Because of Extreme Heatwaves - Carbon Copy </a>
</li>
</ul>
</div>
<div class="comment-respond" id="respond">
<a name="commentbox"> </a>
<h3 class="comment-reply-title" id="reply-title">Write Comments</h3>
<form method="post" accept-charset="utf-8" role="form" action="/latest-news-updates/steps-to-improve-healthcare-in-rural-india-24314.html"><div style="display:none;"><input type="hidden" name="_method" value="POST"/></div> <form class="comment-form" id="commentform" method="post" action="#commentbox" onSubmit="return validate()"
name="cmtform">
<input type="hidden" name="cmttype" value="articlecmt"/>
<input type="hidden" name="article_id" value="24141"/>
<p class="comment-notes">Your email address will not be published. Required fields are marked <span
class="required">*</span></p>
<p class="comment-form-author">
<label for="commenterName">Name</label>
<span class="required">*</span>
<input type="text" aria-required="true" size="30"
value=""
name="commenterName" id="commenterName" required="true">
</p>
<p class="comment-form-email">
<label for="commenterEmail">Email</label> <span class="required">*</span>
<input aria-required="true" size="30" name="commenterEmail" id="commenterEmail" type="email"
value=""
required="true">
</p>
<p class="comment-form-contact">
<label for="commenterPh">Contact No.</label>
<input type="text" size="30"
value=""
name="commenterPh" id="commenterPh">
</p>
<p class="comment-form-comment">
<label for="comment">Comment</label>
<textarea aria-required="true" required="true" rows="8" cols="45" name="comment"
id="comment"></textarea>
</p>
<p class="comment-form-comment">
<label for="comment">Type the characters you see in the image below <span class="required">*</span><br><img
class="captchaImg"
src="https://im4change.in/securimage_show_art.php?tk=459709222" alt="captcha"/>
</label>
</p>
<input type="text" name="vrcode" required="true"/>
<p class="form-submit" style="width: 200px;">
<input type="submit" value="Post Comment" id="submit" name="submit">
</p></form>
</div>
<style>
.ui-widget-content {
height: auto !important;
}
</style>
<div id="share-modal"></div>
<style>
.middleContent a{
background-color: rgba(108,172,228,.2);
}
.middleContent a:hover{
background-color: #418fde;
border-color: #418fde;
color: #000;
}
</style>
<script>
function shareArticle(article_id) {
var options = {
modal: true,
height: 'auto',
width: 600 + 'px'
};
$('#share-modal').html("");
$('#share-modal').load('https://im4change.in/share_article?article_id=' + article_id).dialog(options).dialog('open');
}
function postShare() {
var param = 'article_id=' + $("#article_id").val();
param = param + '&y_name=' + $("#y_name").val();
param = param + '&y_email=' + $("#y_email").val();
param = param + '&f_name=' + $("#f_name").val();
param = param + '&f_email=' + $("#f_email").val();
param = param + '&y_msg=' + $("#y_msg").val();
$.ajax({
type: "POST",
url: 'https://im4change.in/post_share_article',
data: param,
success: function (response) {
$('#share-modal').html("Thank You, Your message posted to ");
}
});
return false;
}
</script> </div>
</div>
<!-- Right Side Section Start -->
<!-- MAP Section START -->
<aside class="sidebar indexMarg">
<div class="ad-cell">
<a href="https://im4change.in/statemap.php" title="">
<img src="https://im4change.in/images/map_new_version.png?1582080666" alt="India State Map" class="indiamap" width="232" height="252"/> </a>
<div class="rightmapbox">
<div id="sideOne" class="docltitle"><a href="https://im4change.in/state-report/india/36" target="_blank">DOCUMENTS/
REPORTS</a></div>
<div id="sideTwo" class="statetitle"><a href="https://im4change.in/states.php"target="_blank">STATE DATA/
HDRs.</a></div>
</div>
<div class="widget widgePadTop"></div>
</div>
</aside>
<!-- MAP Section END -->
<aside class="sidebar sidePadbottom">
<div class="rightsmlbox1" >
<a href="https://im4change.in/knowledge_gateway" target="_blank" style="color: #035588;
font-size: 17px;">
KNOWLEDGE GATEWAY
</a>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/newsletter" target="_blank">
NEWSLETTER
</a>
</p>
</div>
</div>
<div class="rightsmlbox1" style="height: 325px;">
<div>
<p class="rightsmlbox1_title">
Interview with Prof. Ravi Srivastava
</p>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/video/interview-with-prof-ravi-srivastava-on-current-economic-crisis">
<img width="250" height="200" src="/images/interview_video_home.jpg" alt="Interview with Prof. Ravi Srivastava"/>
</a>
<!--
<iframe width="250" height="200" src="https://www.youtube.com/embed/MmaTlntk-wc" frameborder="0" allow="accelerometer; autoplay; encrypted-media; gyroscope; picture-in-picture" allowfullscreen=""></iframe>-->
</p>
<a href="https://im4change.in/videogallery" class="more-link CatArchalAnch1" target="_blank">
More videos
</a>
</div>
</div>
<div class="rightsmlbox1">
<div>
<!--div id="sstory" class="rightboxicons"></div--->
<p class="rightsmlbox1_title"><a href="https://im4change.in/list-success-stories" target="_blank">Success Stories</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/interviews" target="_blank">Interviews</a>
</p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a href="https://www.commoncause.in/page.php?id=10" >Donate</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/marquee"
class="isf_link more-link" title="India Focus?" style="border: 4px solid #fdd922;width: 90%;background-color: #fdd922;text-align: center;color: #000000;font-size:18px" target="_blank">India Focus</a></p> </div>
</div>
<div class="rightsmlbox1" style="height: 104px !important;">
<a href="https://im4change.in/quarterly_reports.php" target="_blank">
Quarterly Reports on Effect of Economic Slowdown on Employment in India (2008 - 2015)
</a>
</div>
<!-- <div class="rightsmlbox1">
<a href="https://play.google.com/store/apps/details?id=com.im4.im4change" target="_blank">
</a></div> -->
<!-- <section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">Most Visited</h2>
</section> -->
<!-- accordion Starts here -->
<!-- <div id="accordion" class="accordMarg">
</div> -->
<!-- accordion ends here -->
<!-- Widget Tag Cloud Starts here -->
<div id="tag_cloud-2" class="widget widget_tag_cloud">
<section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">MOST VISITED TAGS</h2>
</section>
<div class="widget-top wiPdTp">
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<div class="tagcloud">
<a href="https://im4change.in/search?qryStr=Agriculture"
target="_blank" class="tag-link-4 font4">Agriculture</a>
<a href="https://im4change.in/search?qryStr=Food Security"
target="_blank" class="tag-link-4 font4">Food Security</a>
<a href="https://im4change.in/search?qryStr=Law and Justice"
target="_blank" class="tag-link-4 font4">Law and Justice</a>
<a href="https://im4change.in/search?qryStr=Health"
target="_blank" class="tag-link-4 font4">Health</a>
<a href="https://im4change.in/search?qryStr=Right to Food"
target="_blank" class="tag-link-4 font4">Right to Food</a>
<a href="https://im4change.in/search?qryStr=Corruption"
target="_blank" class="tag-link-4 font4">Corruption</a>
<a href="https://im4change.in/search?qryStr=farming"
target="_blank" class="tag-link-4 font4">farming</a>
<a href="https://im4change.in/search?qryStr=Environment"
target="_blank" class="tag-link-4 font4">Environment</a>
<a href="https://im4change.in/search?qryStr=Right to Information"
target="_blank" class="tag-link-4 font4">Right to Information</a>
<a href="https://im4change.in/search?qryStr=NREGS"
target="_blank" class="tag-link-4 font4">NREGS</a>
<a href="https://im4change.in/search?qryStr=Human Rights"
target="_blank" class="tag-link-4 font4">Human Rights</a>
<a href="https://im4change.in/search?qryStr=Governance"
target="_blank" class="tag-link-4 font4">Governance</a>
<a href="https://im4change.in/search?qryStr=PDS"
target="_blank" class="tag-link-4 font4">PDS</a>
<a href="https://im4change.in/search?qryStr=COVID-19"
target="_blank" class="tag-link-4 font4">COVID-19</a>
<a href="https://im4change.in/search?qryStr=Land Acquisition"
target="_blank" class="tag-link-4 font4">Land Acquisition</a>
<a href="https://im4change.in/search?qryStr=mgnrega"
target="_blank" class="tag-link-4 font4">mgnrega</a>
<a href="https://im4change.in/search?qryStr=Farmers"
target="_blank" class="tag-link-4 font4">Farmers</a>
<a href="https://im4change.in/search?qryStr=transparency"
target="_blank" class="tag-link-4 font4">transparency</a>
<a href="https://im4change.in/search?qryStr=Gender"
target="_blank" class="tag-link-4 font4">Gender</a>
<a href="https://im4change.in/search?qryStr=Poverty"
target="_blank" class="tag-link-4 font4">Poverty</a>
<a href="https://im4change.in/search?qryStr=Farm Laws" target="_blank" class="tag-link-4 font4">Farm Laws
</a>
<a href="https://im4change.in/search?qryStr=Citizenship Amendment Act" target="_blank" class="tag-link-4 font4">Citizenship Amendment Act
</a>
<a href="https://im4change.in/search?qryStr=CAA NPR NRIC" target="_blank" class="tag-link-4 font4">CAA NPR NRIC
</a>
<a href="https://im4change.in/search?qryStr=Job Losses" target="_blank" class="tag-link-4 font4">Job Losses
</a>
<a href="https://im4change.in/search?qryStr=Migrant Workers" target="_blank" class="tag-link-4 font4">Migrant Workers
</a>
<a href="https://im4change.in/search?qryStr=Unemployment" target="_blank" class="tag-link-4 font4">Unemployment
</a>
<a href="https://im4change.in/search?qryStr=PMGKAY" target="_blank" class="tag-link-4 font4">PMGKAY
</a>
<a href="https://im4change.in/search?qryStr=PM-KISAN" target="_blank" class="tag-link-4 font4">PM-KISAN
</a>
<a href="https://im4change.in/search?qryStr=PM-CARES" target="_blank" class="tag-link-4 font4">PM-CARES
</a>
<a href="https://im4change.in/search?qryStr=LFPR" target="_blank" class="tag-link-4 font4">LFPR
</a>
</div>
</div>
</div>
<!-- Widget Tag Cloud Ends here -->
</aside>
<!-- Right Side Section End -->
</div>
<section class="cat-box cats-review-box footerSec">
<h2 class="cat-box-title vSec CatArcha">Video
Archives</h2>
<h2 class="cat-box-title CatArchaTitle">Archives</h2>
<div class="cat-box-content">
<div class="reviews-cat">
<div class="CatArchaDiv1">
<div class="CatArchaDiv2">
<ul>
<li>
<a href="https://im4change.in/news-alerts-57/moving-upstream-luni-fellowship.html" target="_blank">
Moving Upstream: Luni – Fellowship </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/135-million-indians-exited-multidimensional-poverty-as-per-government-figures-is-that-the-same-as-poverty-reduction.html" target="_blank">
135 Million Indians Exited “Multidimensional" Poverty as per Government... </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/explainer-why-are-tomato-prices-on-fire.html" target="_blank">
Explainer: Why are Tomato Prices on Fire? </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/nsso-survey-only-39-1-of-all-households-have-drinking-water-within-dwelling-46-7-of-rural-households-use-firewood-for-cooking.html" target="_blank">
NSSO Survey: Only 39.1% of all Households have Drinking... </a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/news-alerts-57"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/I51LYnP8BOk/1.jpg"
alt=" Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Short-Video-on-im4change-Hindi-website-Inclusive-Media-for-Change" target="_blank">
Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/kNqha-SwfIY/1.jpg"
alt=" "Session 1: Scope of IDEA and AgriStack" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-1- Scope-of-IDEA-and-AgriStack-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 1: Scope of IDEA and AgriStack" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/6kIVjlgZItk/1.jpg"
alt=" "Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-2-Farmer-Centric-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/2BeHTu0y7xc/1.jpg"
alt=" "Session 3: Future of Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-3-Future-of-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 3: Future of Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="divWidth">
<ul class="divWidthMarg">
<li>
<a href="https://im4change.in/video/Public-Spending-on-Agriculture-in-India-Source-Foundation-for-Agrarian-Studies"
title="Public Spending on Agriculture in India (Source: Foundation for Agrarian Studies)" target="_blank">
Public Spending on Agriculture in India (Source: Foundation for...</a>
</li>
<li>
<a href="https://im4change.in/video/Agrarian-Change-Seminar-Protests-against-the-New-Farm-Laws-in-India-by-Prof-Vikas-Rawal-JNU-Source-Journal-Of-Agrarian-Change"
title="Agrarian Change Seminar: 'Protests against the New Farm Laws in India' by Prof. Vikas Rawal, JNU (Source: Journal Of Agrarian Change) " target="_blank">
Agrarian Change Seminar: 'Protests against the New Farm Laws...</a>
</li>
<li>
<a href="https://im4change.in/video/Webinar-Ramrao-The-Story-of-India-Farm-Crisis-Source-Azim-Premji-University"
title="Webinar: Ramrao - The Story of India's Farm Crisis (Source: Azim Premji University)" target="_blank">
Webinar: Ramrao - The Story of India's Farm Crisis...</a>
</li>
<li>
<a href="https://im4change.in/video/water-and-agricultural-transformation-in-India"
title="Water and Agricultural Transformation in India: A Symbiotic Relationship (Source: IGIDR)" target="_blank">
Water and Agricultural Transformation in India: A Symbiotic Relationship...</a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/videogallery"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
</div>
</div>
</div>
</section> </div>
<div class="clear"></div>
<!-- Footer option Starts here -->
<div class="footer-bottom fade-in animated4">
<div class="container">
<div class="social-icons icon_flat">
<p class="SocialMargTop"> Website Developed by <a target="_blank" title="Web Development"
class="wot right"
href="http://www.ravinderkhurana.com/" rel="nofollow">
RAVINDErkHURANA.com</a></p>
</div>
<div class="alignleft">
<a
target="_blank" href="https://im4change.in/objectives-8.html"
class="link"
title="Objectives">Objectives</a> | <a
target="_blank" href="https://im4change.in/about-us-9.html"
class="link" title="About Us">About Us</a> | <a
target="_blank" href="https://im4change.in/media-workshops.php"
class="ucwords">Workshops</a> | <a
target="_blank" href="https://im4change.in/disclaimer/disclaimer-149.html"
title="Disclaimer">Disclaimer</a> </div>
</div>
</div>
<!-- Footer option ends here -->
</div>
<div id="connect">
<a target="_blank"
href="http://www.facebook.com/sharer.php?u=https://im4change.in/latest-news-updates/steps-to-improve-healthcare-in-rural-india-24314.html"
title="Share on Facebook">
<img src="https://im4change.in/images/Facebook.png?1582080640" alt="share on Facebook" class="ImgBorder"/>
</a><br/>
<a target="_blank"
href="http://twitter.com/share?text=Im4change&url=https://im4change.in/latest-news-updates/steps-to-improve-healthcare-in-rural-india-24314.html"
title="Share on Twitter">
<img src="https://im4change.in/images/twitter.png?1582080632" alt="Twitter" class="ImgBorder"/> </a>
<br/>
<a href="/feeds" title="RSS Feed" target="_blank">
<img src="https://im4change.in/images/rss.png?1582080632" alt="RSS" class="ImgBorder"/>
</a>
<br/>
<a class="feedback-link" id="feedbackFormLink" href="#">
<img src="https://im4change.in/images/feedback.png?1582080630" alt="Feedback" class="ImgBorder"/>
</a> <br/>
<a href="javascript:function iprl5(){var d=document,z=d.createElement('scr'+'ipt'),b=d.body,l=d.location;try{if(!b)throw(0);d.title='(Saving...) '+d.title;z.setAttribute('src',l.protocol+'//www.instapaper.com/j/WKrH3R7ORD5p?u='+encodeURIComponent(l.href)+'&t='+(new Date().getTime()));b.appendChild(z);}catch(e){alert('Please wait until the page has loaded.');}}iprl5();void(0)"
class="bookmarklet" onclick="return explain_bookmarklet();">
<img src="https://im4change.in/images/read-it-later.png?1582080632" alt="Read Later" class="ImgBorder"/> </a>
</div>
<!-- Feedback form Starts here -->
<div id="feedbackForm" class="overlay_form" class="ImgBorder">
<h2>Contact Form</h2>
<div id="contactform1">
<div id="formleft">
<form id="submitform" action="/contactus.php" method="post">
<input type="hidden" name="submitform" value="submitform"/>
<input type="hidden" name="salt_key" value="a0e0f2c6a0644a70e57ad2c96829709a"/>
<input type="hidden" name="ref" value="feedback"/>
<fieldset>
<label>Name :</label>
<input type="text" name="name" class="tbox" required/>
</fieldset>
<fieldset>
<label>Email :</label>
<input type="text" name="email" class="tbox" required/>
</fieldset>
<fieldset>
<label>Message :</label>
<textarea rows="5" cols="20" name="message" required></textarea>
</fieldset>
<fieldset>
Please enter security code
<div class="clear"></div>
<input type="text" name="vrcode" class="tbox"/>
</fieldset>
<fieldset>
<input type="submit" class="button" value="Submit"/>
<a href="#" id="closefeedbakcformLink">Close</a>
</fieldset>
</form>
</div>
<div class="clearfix"></div>
</div>
</div>
<div id="donate_popup" class="modal" style="max-width: 800px;">
<table width="100%" border="1">
<tr>
<td colspan="2" align="center">
<b>Support im4change</b>
</td>
</tr>
<tr>
<td width="25%" valign="middle">
<img src="https://im4change.in/images/logo2.jpg?1582080632" alt="" width="100%"/> </td>
<td style="padding-left:10px;padding-top:10px;">
<form action="https://im4change.in/donate" method="get">
<table width="100%" cellpadding="2" cellspacing="2">
<tr>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
10
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
100
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
1000
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
50
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
500
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
<input type="text" name="price" placeholder="?" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td colspan="3" align="right">
<input type="button" name="Pay" value="Pay"
style="width: 200px;background-color: rgb(205, 35, 36);color: #ffffff;"/>
</td>
</tr>
</table>
</form>
</td>
</tr>
</table>
</div><script type='text/javascript'>
/* <![CDATA[ */
var tievar = {'go_to': 'Go to...'};
/* ]]> */
</script>
<script src="/js/tie-scripts.js?1575549704"></script><script src="/js/bootstrap.js?1575549704"></script><script src="/js/jquery.modal.min.js?1578284310"></script><script>
$(document).ready(function() {
// tell the autocomplete function to get its data from our php script
$('#s').autocomplete({
source: "/autocomplete"
});
});
</script>
<script src="/vj-main-sw-register.js" async></script>
<script>function init(){var imgDefer=document.getElementsByTagName('img');for(var i=0;i<imgDefer.length;i++){if(imgDefer[i].getAttribute('data-src')){imgDefer[i].setAttribute('src',imgDefer[i].getAttribute('data-src'))}}}
window.onload=init;</script>
</body>
</html>'
}
$maxBufferLength = (int) 8192
$file = '/home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php'
$line = (int) 853
$message = 'Unable to emit headers. Headers sent in file=/home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php line=853'
Cake\Http\ResponseEmitter::emit() - CORE/src/Http/ResponseEmitter.php, line 48
Cake\Http\Server::emit() - CORE/src/Http/Server.php, line 141
[main] - ROOT/webroot/index.php, line 39
Warning (2): Cannot modify header information - headers already sent by (output started at /home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php:853) [CORE/src/Http/ResponseEmitter.php, line 148]
$response = object(Cake\Http\Response) {
'status' => (int) 200,
'contentType' => 'text/html',
'headers' => [
'Content-Type' => [
[maximum depth reached]
]
],
'file' => null,
'fileRange' => [],
'cookies' => object(Cake\Http\Cookie\CookieCollection) {},
'cacheDirectives' => [],
'body' => '<!DOCTYPE html>
<!--[if lt IE 7 ]>
<html class="ie ie6" lang='en'> <![endif]-->
<!--[if IE 7 ]>
<html class="ie ie7" lang='en'> <![endif]-->
<!--[if IE 8 ]>
<html class="ie ie8" lang='en'> <![endif]-->
<!--[if (gte IE 9)|!(IE)]><!-->
<html lang='en'>
<!--<![endif]-->
<head><meta http-equiv="Content-Type" content="text/html; charset=utf-8">
<title>
LATEST NEWS UPDATES | Steps to improve Healthcare in Rural India </title>
<meta name="description" content="
-Press Information Bureau (Ministry of Health and Family Welfare)
Healthcare for all, particularly for the rural areas has been a priority for the Government. The health indicators like Infant Mortality Rate (IMR), Total Fertility Rate (TFR), and nutritional status of children..."/>
<meta name="keywords" content="Public Health,Health,infant mortality"/>
<meta name="news_keywords" content="Public Health,Health,infant mortality">
<link rel="alternate" type="application/rss+xml" title="ROR" href="/ror.xml"/>
<link rel="alternate" type="application/rss+xml" title="RSS 2.0" href="/feeds/"/>
<link rel="stylesheet" href="/css/bootstrap.min.css?1697864993"/> <link rel="stylesheet" href="/css/style.css?v=1.1.2"/> <link rel="stylesheet" href="/css/style-inner.css?1577045210"/> <link rel="stylesheet" id="Oswald-css"
href="https://fonts.googleapis.com/css?family=Oswald%3Aregular%2C700&ver=3.8.1" type="text/css"
media="all">
<link rel="stylesheet" href="/css/jquery.modal.min.css?1578285302"/> <script src="/js/jquery-1.10.2.js?1575549704"></script> <script src="/js/jquery-migrate.min.js?1575549704"></script> <link rel="shortcut icon" href="/favicon.ico" title="Favicon">
<link rel="stylesheet" href="/css/jquery-ui.css?1580720609"/> <script src="/js/jquery-ui.js?1575549704"></script> <link rel="preload" as="style" href="https://www.im4change.org/css/custom.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery.modal.min.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery-ui.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/li-scroller.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<!-- <link rel="preload" as="style" href="https://www.im4change.org/css/style.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous"> -->
<link rel="preload" as="style" href="https://www.im4change.org/css/style-inner.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel='dns-prefetch' href="//im4change.org/css/custom.css" crossorigin >
<link rel="preload" as="script" href="https://www.im4change.org/js/bootstrap.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.li-scroller.1.0.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.modal.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.ui.totop.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-1.10.2.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-migrate.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-ui.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/setting.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/tie-scripts.js">
<!--[if IE]>
<script type="text/javascript">jQuery(document).ready(function () {
jQuery(".menu-item").has("ul").children("a").attr("aria-haspopup", "true");
});</script>
<![endif]-->
<!--[if lt IE 9]>
<script src="/js/html5.js"></script>
<script src="/js/selectivizr-min.js"></script>
<![endif]-->
<!--[if IE 8]>
<link rel="stylesheet" type="text/css" media="all" href="/css/ie8.css"/>
<![endif]-->
<meta property="og:title" content="LATEST NEWS UPDATES | Steps to improve Healthcare in Rural India" />
<meta property="og:url" content="https://im4change.in/latest-news-updates/steps-to-improve-healthcare-in-rural-india-24314.html" />
<meta property="og:type" content="article" />
<meta property="og:description" content="
-Press Information Bureau (Ministry of Health and Family Welfare)
Healthcare for all, particularly for the rural areas has been a priority for the Government. The health indicators like Infant Mortality Rate (IMR), Total Fertility Rate (TFR), and nutritional status of children..." />
<meta property="og:image" content="" />
<meta property="fb:app_id" content="0" />
<meta name="viewport" content="width=device-width, initial-scale=1, maximum-scale=1, user-scalable=no">
<link rel="apple-touch-icon-precomposed" sizes="144x144" href="https://im4change.in/images/apple1.png">
<link rel="apple-touch-icon-precomposed" sizes="120x120" href="https://im4change.in/images/apple2.png">
<link rel="apple-touch-icon-precomposed" sizes="72x72" href="https://im4change.in/images/apple3.png">
<link rel="apple-touch-icon-precomposed" href="https://im4change.in/images/apple4.png">
<style>
.gsc-results-wrapper-overlay{
top: 38% !important;
height: 50% !important;
}
.gsc-search-button-v2{
border-color: #035588 !important;
background-color: #035588 !important;
}
.gsib_a{
height: 30px !important;
padding: 2px 8px 1px 6px !important;
}
.gsc-search-button-v2{
height: 41px !important;
}
input.gsc-input{
background: none !important;
}
@media only screen and (max-width: 600px) {
.gsc-results-wrapper-overlay{
top: 11% !important;
width: 87% !important;
left: 9% !important;
height: 43% !important;
}
.gsc-search-button-v2{
padding: 10px 10px !important;
}
.gsc-input-box{
height: 28px !important;
}
/* .gsib_a {
padding: 0px 9px 4px 9px !important;
}*/
}
@media only screen and (min-width: 1200px) and (max-width: 1920px) {
table.gsc-search-box{
width: 15% !important;
float: right !important;
margin-top: -118px !important;
}
.gsc-search-button-v2 {
padding: 6px !important;
}
}
</style>
<script>
$(function () {
$("#accordion").accordion({
event: "click hoverintent"
});
});
/*
* hoverIntent | Copyright 2011 Brian Cherne
* http://cherne.net/brian/resources/jquery.hoverIntent.html
* modified by the jQuery UI team
*/
$.event.special.hoverintent = {
setup: function () {
$(this).bind("mouseover", jQuery.event.special.hoverintent.handler);
},
teardown: function () {
$(this).unbind("mouseover", jQuery.event.special.hoverintent.handler);
},
handler: function (event) {
var currentX, currentY, timeout,
args = arguments,
target = $(event.target),
previousX = event.pageX,
previousY = event.pageY;
function track(event) {
currentX = event.pageX;
currentY = event.pageY;
}
;
function clear() {
target
.unbind("mousemove", track)
.unbind("mouseout", clear);
clearTimeout(timeout);
}
function handler() {
var prop,
orig = event;
if ((Math.abs(previousX - currentX) +
Math.abs(previousY - currentY)) < 7) {
clear();
event = $.Event("hoverintent");
for (prop in orig) {
if (!(prop in event)) {
event[prop] = orig[prop];
}
}
// Prevent accessing the original event since the new event
// is fired asynchronously and the old event is no longer
// usable (#6028)
delete event.originalEvent;
target.trigger(event);
} else {
previousX = currentX;
previousY = currentY;
timeout = setTimeout(handler, 100);
}
}
timeout = setTimeout(handler, 100);
target.bind({
mousemove: track,
mouseout: clear
});
}
};
</script>
<script type="text/javascript">
var _gaq = _gaq || [];
_gaq.push(['_setAccount', 'UA-472075-3']);
_gaq.push(['_trackPageview']);
(function () {
var ga = document.createElement('script');
ga.type = 'text/javascript';
ga.async = true;
ga.src = ('https:' == document.location.protocol ? 'https://ssl' : 'http://www') + '.google-analytics.com/ga.js';
var s = document.getElementsByTagName('script')[0];
s.parentNode.insertBefore(ga, s);
})();
</script>
<link rel="stylesheet" href="/css/custom.css?v=1.16"/> <script src="/js/jquery.ui.totop.js?1575549704"></script> <script src="/js/setting.js?1575549704"></script> <link rel="manifest" href="/manifest.json">
<meta name="theme-color" content="#616163" />
<meta name="apple-mobile-web-app-capable" content="yes">
<meta name="apple-mobile-web-app-status-bar-style" content="black">
<meta name="apple-mobile-web-app-title" content="im4change">
<link rel="apple-touch-icon" href="/icons/logo-192x192.png">
</head>
<body id="top" class="home inner blog">
<div class="background-cover"></div>
<div class="wrapper animated">
<header id="theme-header" class="header_inner" style="position: relative;">
<div class="logo inner_logo" style="left:20px !important">
<a title="Home" href="https://im4change.in/">
<img src="https://im4change.in/images/logo2.jpg?1582080632" class="logo_image" alt="im4change"/> </a>
</div>
<div class="langhindi" style="color: #000;display:none;"
href="https://im4change.in/">
<a class="more-link" href="https://im4change.in/">Home</a>
<a href="https://im4change.in/hindi/" class="langbutton ">हिन्दी</a>
</div>
<nav class="fade-in animated2" id="main-nav">
<div class="container">
<div class="main-menu">
<ul class="menu" id="menu-main">
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
style="left: -40px;"><a
target="_blank" href="https://im4change.in/">Home</a>
</li>
<li class="menu-item mega-menu menu-item-type-taxonomy mega-menu menu-item-object-category mega-menu menu-item-has-children parent-list"
style=" margin-left: -40px;"><a href="#">KNOWLEDGE GATEWAY <span class="sub-indicator"></span>
</a>
<div class="mega-menu-block background_menu" style="padding-top:25px;">
<div class="container">
<div class="mega-menu-content">
<div class="mega-menu-item">
<h3><b>Farm Crisis</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/farmers039-suicides-14.html"
class="left postionrel">Farm Suicides </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/unemployment-30.html"
class="left postionrel">Unemployment </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/rural-distress-70.html"
class="left postionrel">Rural distress </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/migration-34.html"
class="left postionrel">Migration </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/key-facts-72.html"
class="left postionrel">Key Facts </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/debt-trap-15.html"
class="left postionrel">Debt Trap </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Empowerment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/union-budget-73.html"
class="left postionrel">Union Budget And Other Economic Policies </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/forest-and-tribal-rights-61.html"
class="left postionrel">Forest and Tribal Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-education-60.html"
class="left postionrel">Right to Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-food-59.html"
class="left postionrel">Right to Food </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/displacement-3279.html"
class="left postionrel">Displacement </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-work-mg-nrega-39.html"
class="left postionrel">Right to Work (MG-NREGA) </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/gender-3280.html"
class="left postionrel">GENDER </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-information-58.html"
class="left postionrel">Right to Information </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/social-audit-48.html"
class="left postionrel">Social Audit </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Hunger / HDI</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/poverty-and-inequality-20499.html"
class="left postionrel">Poverty and inequality </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/malnutrition-41.html"
class="left postionrel">Malnutrition </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/public-health-51.html"
class="left postionrel">Public Health </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/education-50.html"
class="left postionrel">Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hunger-overview-40.html"
class="left postionrel">Hunger Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hdi-overview-45.html"
class="left postionrel">HDI Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/pds-ration-food-security-42.html"
class="left postionrel">PDS/ Ration/ Food Security </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/sdgs-113.html"
class="left postionrel">SDGs </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/mid-day-meal-scheme-mdms-53.html"
class="left postionrel">Mid Day Meal Scheme (MDMS) </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Environment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/time-bomb-ticking-52.html"
class="left postionrel">Time Bomb Ticking </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/water-and-sanitation-55.html"
class="left postionrel">Water and Sanitation </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/impact-on-agriculture-54.html"
class="left postionrel">Impact on Agriculture </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Law & Justice</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/social-justice-20500.html"
class="left postionrel">Social Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/access-to-justice-47.html"
class="left postionrel">Access to Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/human-rights-56.html"
class="left postionrel">Human Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/corruption-35.html"
class="left postionrel">Corruption </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/general-insecurity-46.html"
class="left postionrel">General Insecurity </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/disaster-relief-49.html"
class="left postionrel">Disaster & Relief </a>
</p>
</div>
</div>
</div>
</div>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page "><a target="_blank" href="https://im4change.in/nceus_reports.php">NCEUS reports</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children parent-list ">
<a target="_blank" href="https://im4change.in/about-us-9.html">About Us <span
class="sub-indicator"></span></a>
<ul class="sub-menu aboutmenu">
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/objectives-8.html">Objectives</a>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/contactus.php">Contact
Us</a></li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/about-us-9.html">About
Us</a></li>
</ul>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children ">
<a target="_blank" href="https://im4change.in/fellowships.php" title="Fellowships">Fellowships</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/media-workshops.php">Workshops</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/research.php">Research</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/links-64">Partners</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
id="menu-item-539"><a target="_blank" href="https://im4change.in/hindi/"
class="langbutton langlinkfont17">हिन्दी</a></li>
</ul>
</div> </div>
<!-- <div style="float: right;">
<script async src="https://cse.google.com/cse.js?cx=18b4f2e0f11bed3dd"></script>
<div class="gcse-search"></div>
</div> -->
<div class="search-block" style=" margin-left: 8px; margin-right: 7px;">
<form method="get" id="searchform" name="searchform"
action="https://im4change.in/search"
onsubmit="return searchvalidate();">
<button class="search-button" type="submit" value="Search"></button>
<input type="text" id="s" name="qryStr" value=""
onfocus="if (this.value == 'Search...') {this.value = '';}"
onblur="if (this.value == '') {this.value = 'Search...';}">
</form>
</div>
</nav>
</header>
<div class="container">
<div id="main-content" class=" main1 container fade-in animated3 sidebar-narrow-left">
<div class="content-wrap">
<div class="content" style="width: 900px;min-height: 500px;">
<section class="cat-box recent-box innerCatRecent">
<h1 class="cat-box-title">Steps to improve Healthcare in Rural India</h1>
<a href="JavaScript:void(0);" onclick="return shareArticle(24141);">
<img src="https://im4change.in/images/email.png?1582080630" border="0" width="24" align="right" alt="Share this article"/> </a>
<a href="https://im4change.in/latest-news-updates/steps-to-improve-healthcare-in-rural-india-24314/print"
rel="nofollow">
<img src="https://im4change.in/images/icon-print.png?1582080630" border="0" width="24" align="right" alt="Share this article"/>
</a>
</section>
<section class="recent-box innerCatRecent">
<small class="pb-1"><span class="dateIcn">
<img src="https://im4change.in/images/published.svg?1582080666" alt="published"/>
Published on</span><span class="text-date"> Feb 21, 2014</span>
<span
class="dateIcn">
<img src="https://im4change.in/images/modified.svg?1582080666" alt="modified"/> Modified on </span><span class="text-date"> Feb 21, 2014</span>
</small>
</section>
<div class="clear"></div>
<div style="padding-top: 10px;">
<div class="innerLineHeight">
<div class="middleContent innerInput latest-news-updates">
<table>
<tr>
<td>
<div>
<div align="justify">-Press Information Bureau (Ministry of Health and Family Welfare)</div><p align="justify"><br />Healthcare for all, particularly for the rural areas has been a priority for the Government. The health indicators like Infant Mortality Rate (IMR), Total Fertility Rate (TFR), and nutritional status of children under 3 years including prevalence of anemia amongst them and pregnant women in rural area are considerably poor as compared to urban areas. The key health indicators are as under:</p><p align="justify"><img src="https://im4change.in/siteadmin/tinymce/uploaded/Health_2.JPG" alt="Health" width="602" height="187" /></p><p align="justify">Public Health is a state subject. However, Central Government launched NRHM in 2005 to provide financial support to the States/UTs to strengthen their health systems particularly to cater to the healthcare needs of rural areas. Key steps taken to improve health care in rural areas include the following:</p><p align="justify"> </p><p align="justify"> i. Support is provided to States/UTs under NRHM, to strengthen the health system including establishment/up-gradation/renovation of health infrastructure, engagement of Nurses, doctors and specialist on contractual basis based on the appraisal of requirements proposed by the States in their Programme Implementation Plans (PIP),</p><p align="justify"> ii. Support under NRHM is also provided by way of additional incentives to serve in remote underserved areas, so that health professionals find it attractive to join public health facilities in such areas. In order to encourage the States to fill up existing vacancies in remote rural areas, the states are being incentivized to ensure rational deployment of health human resource. Manpower deployment is also to be put on the web in public domain,</p><p align="justify"> iii. To increase the availability of doctors, several initiatives have been taken to rationalize the norms in medical education, such as, relaxation in land requirements, bed strength, increase in ceiling for maximum intake for undergraduates, enhancement of teacher-student ratio in Post Graduate Courses, etc., which has resulted in substantial increase in number of undergraduate and post graduate seats. Government has also approved setting up of ANM/GNM Schools in different States besides setting up of Institutes of Paramedical Sciences at National and regional levels,</p><p align="justify"> iv. States/UTs are being impressed upon from time to time to make available improved health facilities including free essential medicines in all public health facilities. Accordingly, financial support is being provided for ensuring uninterrupted supply of free essential medicines in public health facilities based on the requirement proposed by the States in their PIPs. An incentive of upto 5% of the NRHM outlay has also been introduced in 2012-13 for states for establishing policy framework and systems for providing free generic medicines to those who access public health facilities.</p><p align="justify"> v. States/UTs are being provided support for focused attention and greater resources per capita to high priority districts with relatively poor composite health index.</p><p align="justify"> vi. Financial assistance is provided to the States/UTs for selection and training of Accredited Social Health Activists (ASHA), who act as a link between community and healthcare facilities.</p><p align="justify"> vii. States/UTs are supported with Mobile Medical Units for improved service delivery especially in hard to reach areas. There are over 2000 MMUs that are being supported under NRHM. Support is also provided for Emergency Referral Transport services to ensure in-interrupted referral services. There are over 20000 ambulances that are being supported under NRHM.</p><p align="justify">viii. States/UTs are assisted to constitute Village Health, Sanitation and Nutrition Committees so as to ensure community participation and village level planning and monitoring of health activities.</p><p align="justify"> ix. New initiatives such as Janani Shishu Suraksha Karyakram (JSSK), Rashtriya Bal Swashthya Karyrakram (RBSK), Rashtriya Kishore Swashthya Karyakram (RKSK), ‘National Health Mission Free Drugs Service Initiative' etc., have also been introduced to inter-alia make health care affordable by reducing out of pocket expenditure.</p><p align="justify"> </p><p align="justify">Presently, there is no proposal to revise the existing National Health Policy (NHP) - 2002. The Twelfth Plan seeks to strengthen initiatives taken in the Eleventh Plan to expand the reach of health care and work towards the long term objective of establishing a system of Universal Health Coverage (UHC) in the country. This means that each individual would have assured access to a defined essential range of medicines and treatment at an affordable price, which should be entirely free for large percentage of the population. Inevitably, the list of assured services will have to be limited by budgetary constraints. Further, to ensure equitable health care to bring about sharper improvements in health outcomes, at least 25% of all districts in each state have been identified as high priority districts based on a composite health index. These also include all tribal and LWE affected districts which are below the State's average of composite health index. These districts would receive higher per capita funding, enhanced monitoring, focused supportive supervision and have differential planning norms. These measures would help reduce prevailing health inequalities in rural areas.</p><p align="justify"> </p><p align="justify">This was stated by Shri Ghulam Nabi Azad, Union Minister for Health and Family Welfare in a written reply to the Lok Sabha today.</p><p align="justify">*********</p><p align="justify">MV/GM</p><p align="justify">(Release ID :104096)</p>
</div>
</td>
</tr>
</table>
</div>
</div>
</div>
<div class="clear"></div>
<br><a href="http://www.pib.nic.in/newsite/erelease.aspx?relid=0" class="re" target="_blank">Press Information Bureau, 21 February, 2014, http://www.pib.nic.in/newsite/erelease.aspx?relid=0</a><div class="clear"></div>
<div style="padding-top: 18px;">
<p class="post-tag">Tagged with:
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Public Health"
title="Public Health">
Public Health </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Health"
title="Health">
Health </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=infant mortality"
title="infant mortality">
infant mortality </a>
</p>
</div>
<div class="clear"></div>
<br><br>
<div class="widget-top">
<h4>Related Articles</h4>
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<ul id="recentcomments">
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/fifth-report-from-gambia-implicates-indian-drug-maker-for-contaminated-syrups-banjot-kaur.html"
title="Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur">
Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-may-have-seen-steepest-dip-in-multidimensional-poverty-among-110-nations-as-per-undp-data-nikhil-rampal.html"
title="India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal">
India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/health-among-top-three-priorities-for-indian-voters-after-jobs-and-education-survey-shows-oliver-heath-jyoti-mishra-louise-tillin-sandhya-venkateswaran.html"
title="Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran">
Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/prevalence-of-zero-food-among-infants-and-young-children-in-india-patterns-of-change-across-the-states-and-union-territories-of-india-1993-2021-the-lancet.html"
title="Prevalence of Zero-Food among infants and young children in India - The Lancet ">
Prevalence of Zero-Food among infants and young children in India - The Lancet </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-s-sustainability-goals-at-risk-because-of-extreme-heatwaves-carbon-copy.html"
title="India's Sustainability Goals at Risk Because of Extreme Heatwaves - Carbon Copy">
India's Sustainability Goals at Risk Because of Extreme Heatwaves - Carbon Copy </a>
</li>
</ul>
</div>
<div class="comment-respond" id="respond">
<a name="commentbox"> </a>
<h3 class="comment-reply-title" id="reply-title">Write Comments</h3>
<form method="post" accept-charset="utf-8" role="form" action="/latest-news-updates/steps-to-improve-healthcare-in-rural-india-24314.html"><div style="display:none;"><input type="hidden" name="_method" value="POST"/></div> <form class="comment-form" id="commentform" method="post" action="#commentbox" onSubmit="return validate()"
name="cmtform">
<input type="hidden" name="cmttype" value="articlecmt"/>
<input type="hidden" name="article_id" value="24141"/>
<p class="comment-notes">Your email address will not be published. Required fields are marked <span
class="required">*</span></p>
<p class="comment-form-author">
<label for="commenterName">Name</label>
<span class="required">*</span>
<input type="text" aria-required="true" size="30"
value=""
name="commenterName" id="commenterName" required="true">
</p>
<p class="comment-form-email">
<label for="commenterEmail">Email</label> <span class="required">*</span>
<input aria-required="true" size="30" name="commenterEmail" id="commenterEmail" type="email"
value=""
required="true">
</p>
<p class="comment-form-contact">
<label for="commenterPh">Contact No.</label>
<input type="text" size="30"
value=""
name="commenterPh" id="commenterPh">
</p>
<p class="comment-form-comment">
<label for="comment">Comment</label>
<textarea aria-required="true" required="true" rows="8" cols="45" name="comment"
id="comment"></textarea>
</p>
<p class="comment-form-comment">
<label for="comment">Type the characters you see in the image below <span class="required">*</span><br><img
class="captchaImg"
src="https://im4change.in/securimage_show_art.php?tk=459709222" alt="captcha"/>
</label>
</p>
<input type="text" name="vrcode" required="true"/>
<p class="form-submit" style="width: 200px;">
<input type="submit" value="Post Comment" id="submit" name="submit">
</p></form>
</div>
<style>
.ui-widget-content {
height: auto !important;
}
</style>
<div id="share-modal"></div>
<style>
.middleContent a{
background-color: rgba(108,172,228,.2);
}
.middleContent a:hover{
background-color: #418fde;
border-color: #418fde;
color: #000;
}
</style>
<script>
function shareArticle(article_id) {
var options = {
modal: true,
height: 'auto',
width: 600 + 'px'
};
$('#share-modal').html("");
$('#share-modal').load('https://im4change.in/share_article?article_id=' + article_id).dialog(options).dialog('open');
}
function postShare() {
var param = 'article_id=' + $("#article_id").val();
param = param + '&y_name=' + $("#y_name").val();
param = param + '&y_email=' + $("#y_email").val();
param = param + '&f_name=' + $("#f_name").val();
param = param + '&f_email=' + $("#f_email").val();
param = param + '&y_msg=' + $("#y_msg").val();
$.ajax({
type: "POST",
url: 'https://im4change.in/post_share_article',
data: param,
success: function (response) {
$('#share-modal').html("Thank You, Your message posted to ");
}
});
return false;
}
</script> </div>
</div>
<!-- Right Side Section Start -->
<!-- MAP Section START -->
<aside class="sidebar indexMarg">
<div class="ad-cell">
<a href="https://im4change.in/statemap.php" title="">
<img src="https://im4change.in/images/map_new_version.png?1582080666" alt="India State Map" class="indiamap" width="232" height="252"/> </a>
<div class="rightmapbox">
<div id="sideOne" class="docltitle"><a href="https://im4change.in/state-report/india/36" target="_blank">DOCUMENTS/
REPORTS</a></div>
<div id="sideTwo" class="statetitle"><a href="https://im4change.in/states.php"target="_blank">STATE DATA/
HDRs.</a></div>
</div>
<div class="widget widgePadTop"></div>
</div>
</aside>
<!-- MAP Section END -->
<aside class="sidebar sidePadbottom">
<div class="rightsmlbox1" >
<a href="https://im4change.in/knowledge_gateway" target="_blank" style="color: #035588;
font-size: 17px;">
KNOWLEDGE GATEWAY
</a>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/newsletter" target="_blank">
NEWSLETTER
</a>
</p>
</div>
</div>
<div class="rightsmlbox1" style="height: 325px;">
<div>
<p class="rightsmlbox1_title">
Interview with Prof. Ravi Srivastava
</p>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/video/interview-with-prof-ravi-srivastava-on-current-economic-crisis">
<img width="250" height="200" src="/images/interview_video_home.jpg" alt="Interview with Prof. Ravi Srivastava"/>
</a>
<!--
<iframe width="250" height="200" src="https://www.youtube.com/embed/MmaTlntk-wc" frameborder="0" allow="accelerometer; autoplay; encrypted-media; gyroscope; picture-in-picture" allowfullscreen=""></iframe>-->
</p>
<a href="https://im4change.in/videogallery" class="more-link CatArchalAnch1" target="_blank">
More videos
</a>
</div>
</div>
<div class="rightsmlbox1">
<div>
<!--div id="sstory" class="rightboxicons"></div--->
<p class="rightsmlbox1_title"><a href="https://im4change.in/list-success-stories" target="_blank">Success Stories</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/interviews" target="_blank">Interviews</a>
</p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a href="https://www.commoncause.in/page.php?id=10" >Donate</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/marquee"
class="isf_link more-link" title="India Focus?" style="border: 4px solid #fdd922;width: 90%;background-color: #fdd922;text-align: center;color: #000000;font-size:18px" target="_blank">India Focus</a></p> </div>
</div>
<div class="rightsmlbox1" style="height: 104px !important;">
<a href="https://im4change.in/quarterly_reports.php" target="_blank">
Quarterly Reports on Effect of Economic Slowdown on Employment in India (2008 - 2015)
</a>
</div>
<!-- <div class="rightsmlbox1">
<a href="https://play.google.com/store/apps/details?id=com.im4.im4change" target="_blank">
</a></div> -->
<!-- <section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">Most Visited</h2>
</section> -->
<!-- accordion Starts here -->
<!-- <div id="accordion" class="accordMarg">
</div> -->
<!-- accordion ends here -->
<!-- Widget Tag Cloud Starts here -->
<div id="tag_cloud-2" class="widget widget_tag_cloud">
<section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">MOST VISITED TAGS</h2>
</section>
<div class="widget-top wiPdTp">
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<div class="tagcloud">
<a href="https://im4change.in/search?qryStr=Agriculture"
target="_blank" class="tag-link-4 font4">Agriculture</a>
<a href="https://im4change.in/search?qryStr=Food Security"
target="_blank" class="tag-link-4 font4">Food Security</a>
<a href="https://im4change.in/search?qryStr=Law and Justice"
target="_blank" class="tag-link-4 font4">Law and Justice</a>
<a href="https://im4change.in/search?qryStr=Health"
target="_blank" class="tag-link-4 font4">Health</a>
<a href="https://im4change.in/search?qryStr=Right to Food"
target="_blank" class="tag-link-4 font4">Right to Food</a>
<a href="https://im4change.in/search?qryStr=Corruption"
target="_blank" class="tag-link-4 font4">Corruption</a>
<a href="https://im4change.in/search?qryStr=farming"
target="_blank" class="tag-link-4 font4">farming</a>
<a href="https://im4change.in/search?qryStr=Environment"
target="_blank" class="tag-link-4 font4">Environment</a>
<a href="https://im4change.in/search?qryStr=Right to Information"
target="_blank" class="tag-link-4 font4">Right to Information</a>
<a href="https://im4change.in/search?qryStr=NREGS"
target="_blank" class="tag-link-4 font4">NREGS</a>
<a href="https://im4change.in/search?qryStr=Human Rights"
target="_blank" class="tag-link-4 font4">Human Rights</a>
<a href="https://im4change.in/search?qryStr=Governance"
target="_blank" class="tag-link-4 font4">Governance</a>
<a href="https://im4change.in/search?qryStr=PDS"
target="_blank" class="tag-link-4 font4">PDS</a>
<a href="https://im4change.in/search?qryStr=COVID-19"
target="_blank" class="tag-link-4 font4">COVID-19</a>
<a href="https://im4change.in/search?qryStr=Land Acquisition"
target="_blank" class="tag-link-4 font4">Land Acquisition</a>
<a href="https://im4change.in/search?qryStr=mgnrega"
target="_blank" class="tag-link-4 font4">mgnrega</a>
<a href="https://im4change.in/search?qryStr=Farmers"
target="_blank" class="tag-link-4 font4">Farmers</a>
<a href="https://im4change.in/search?qryStr=transparency"
target="_blank" class="tag-link-4 font4">transparency</a>
<a href="https://im4change.in/search?qryStr=Gender"
target="_blank" class="tag-link-4 font4">Gender</a>
<a href="https://im4change.in/search?qryStr=Poverty"
target="_blank" class="tag-link-4 font4">Poverty</a>
<a href="https://im4change.in/search?qryStr=Farm Laws" target="_blank" class="tag-link-4 font4">Farm Laws
</a>
<a href="https://im4change.in/search?qryStr=Citizenship Amendment Act" target="_blank" class="tag-link-4 font4">Citizenship Amendment Act
</a>
<a href="https://im4change.in/search?qryStr=CAA NPR NRIC" target="_blank" class="tag-link-4 font4">CAA NPR NRIC
</a>
<a href="https://im4change.in/search?qryStr=Job Losses" target="_blank" class="tag-link-4 font4">Job Losses
</a>
<a href="https://im4change.in/search?qryStr=Migrant Workers" target="_blank" class="tag-link-4 font4">Migrant Workers
</a>
<a href="https://im4change.in/search?qryStr=Unemployment" target="_blank" class="tag-link-4 font4">Unemployment
</a>
<a href="https://im4change.in/search?qryStr=PMGKAY" target="_blank" class="tag-link-4 font4">PMGKAY
</a>
<a href="https://im4change.in/search?qryStr=PM-KISAN" target="_blank" class="tag-link-4 font4">PM-KISAN
</a>
<a href="https://im4change.in/search?qryStr=PM-CARES" target="_blank" class="tag-link-4 font4">PM-CARES
</a>
<a href="https://im4change.in/search?qryStr=LFPR" target="_blank" class="tag-link-4 font4">LFPR
</a>
</div>
</div>
</div>
<!-- Widget Tag Cloud Ends here -->
</aside>
<!-- Right Side Section End -->
</div>
<section class="cat-box cats-review-box footerSec">
<h2 class="cat-box-title vSec CatArcha">Video
Archives</h2>
<h2 class="cat-box-title CatArchaTitle">Archives</h2>
<div class="cat-box-content">
<div class="reviews-cat">
<div class="CatArchaDiv1">
<div class="CatArchaDiv2">
<ul>
<li>
<a href="https://im4change.in/news-alerts-57/moving-upstream-luni-fellowship.html" target="_blank">
Moving Upstream: Luni – Fellowship </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/135-million-indians-exited-multidimensional-poverty-as-per-government-figures-is-that-the-same-as-poverty-reduction.html" target="_blank">
135 Million Indians Exited “Multidimensional" Poverty as per Government... </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/explainer-why-are-tomato-prices-on-fire.html" target="_blank">
Explainer: Why are Tomato Prices on Fire? </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/nsso-survey-only-39-1-of-all-households-have-drinking-water-within-dwelling-46-7-of-rural-households-use-firewood-for-cooking.html" target="_blank">
NSSO Survey: Only 39.1% of all Households have Drinking... </a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/news-alerts-57"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/I51LYnP8BOk/1.jpg"
alt=" Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Short-Video-on-im4change-Hindi-website-Inclusive-Media-for-Change" target="_blank">
Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/kNqha-SwfIY/1.jpg"
alt=" "Session 1: Scope of IDEA and AgriStack" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-1- Scope-of-IDEA-and-AgriStack-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 1: Scope of IDEA and AgriStack" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/6kIVjlgZItk/1.jpg"
alt=" "Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-2-Farmer-Centric-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/2BeHTu0y7xc/1.jpg"
alt=" "Session 3: Future of Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-3-Future-of-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 3: Future of Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="divWidth">
<ul class="divWidthMarg">
<li>
<a href="https://im4change.in/video/Public-Spending-on-Agriculture-in-India-Source-Foundation-for-Agrarian-Studies"
title="Public Spending on Agriculture in India (Source: Foundation for Agrarian Studies)" target="_blank">
Public Spending on Agriculture in India (Source: Foundation for...</a>
</li>
<li>
<a href="https://im4change.in/video/Agrarian-Change-Seminar-Protests-against-the-New-Farm-Laws-in-India-by-Prof-Vikas-Rawal-JNU-Source-Journal-Of-Agrarian-Change"
title="Agrarian Change Seminar: 'Protests against the New Farm Laws in India' by Prof. Vikas Rawal, JNU (Source: Journal Of Agrarian Change) " target="_blank">
Agrarian Change Seminar: 'Protests against the New Farm Laws...</a>
</li>
<li>
<a href="https://im4change.in/video/Webinar-Ramrao-The-Story-of-India-Farm-Crisis-Source-Azim-Premji-University"
title="Webinar: Ramrao - The Story of India's Farm Crisis (Source: Azim Premji University)" target="_blank">
Webinar: Ramrao - The Story of India's Farm Crisis...</a>
</li>
<li>
<a href="https://im4change.in/video/water-and-agricultural-transformation-in-India"
title="Water and Agricultural Transformation in India: A Symbiotic Relationship (Source: IGIDR)" target="_blank">
Water and Agricultural Transformation in India: A Symbiotic Relationship...</a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/videogallery"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
</div>
</div>
</div>
</section> </div>
<div class="clear"></div>
<!-- Footer option Starts here -->
<div class="footer-bottom fade-in animated4">
<div class="container">
<div class="social-icons icon_flat">
<p class="SocialMargTop"> Website Developed by <a target="_blank" title="Web Development"
class="wot right"
href="http://www.ravinderkhurana.com/" rel="nofollow">
RAVINDErkHURANA.com</a></p>
</div>
<div class="alignleft">
<a
target="_blank" href="https://im4change.in/objectives-8.html"
class="link"
title="Objectives">Objectives</a> | <a
target="_blank" href="https://im4change.in/about-us-9.html"
class="link" title="About Us">About Us</a> | <a
target="_blank" href="https://im4change.in/media-workshops.php"
class="ucwords">Workshops</a> | <a
target="_blank" href="https://im4change.in/disclaimer/disclaimer-149.html"
title="Disclaimer">Disclaimer</a> </div>
</div>
</div>
<!-- Footer option ends here -->
</div>
<div id="connect">
<a target="_blank"
href="http://www.facebook.com/sharer.php?u=https://im4change.in/latest-news-updates/steps-to-improve-healthcare-in-rural-india-24314.html"
title="Share on Facebook">
<img src="https://im4change.in/images/Facebook.png?1582080640" alt="share on Facebook" class="ImgBorder"/>
</a><br/>
<a target="_blank"
href="http://twitter.com/share?text=Im4change&url=https://im4change.in/latest-news-updates/steps-to-improve-healthcare-in-rural-india-24314.html"
title="Share on Twitter">
<img src="https://im4change.in/images/twitter.png?1582080632" alt="Twitter" class="ImgBorder"/> </a>
<br/>
<a href="/feeds" title="RSS Feed" target="_blank">
<img src="https://im4change.in/images/rss.png?1582080632" alt="RSS" class="ImgBorder"/>
</a>
<br/>
<a class="feedback-link" id="feedbackFormLink" href="#">
<img src="https://im4change.in/images/feedback.png?1582080630" alt="Feedback" class="ImgBorder"/>
</a> <br/>
<a href="javascript:function iprl5(){var d=document,z=d.createElement('scr'+'ipt'),b=d.body,l=d.location;try{if(!b)throw(0);d.title='(Saving...) '+d.title;z.setAttribute('src',l.protocol+'//www.instapaper.com/j/WKrH3R7ORD5p?u='+encodeURIComponent(l.href)+'&t='+(new Date().getTime()));b.appendChild(z);}catch(e){alert('Please wait until the page has loaded.');}}iprl5();void(0)"
class="bookmarklet" onclick="return explain_bookmarklet();">
<img src="https://im4change.in/images/read-it-later.png?1582080632" alt="Read Later" class="ImgBorder"/> </a>
</div>
<!-- Feedback form Starts here -->
<div id="feedbackForm" class="overlay_form" class="ImgBorder">
<h2>Contact Form</h2>
<div id="contactform1">
<div id="formleft">
<form id="submitform" action="/contactus.php" method="post">
<input type="hidden" name="submitform" value="submitform"/>
<input type="hidden" name="salt_key" value="a0e0f2c6a0644a70e57ad2c96829709a"/>
<input type="hidden" name="ref" value="feedback"/>
<fieldset>
<label>Name :</label>
<input type="text" name="name" class="tbox" required/>
</fieldset>
<fieldset>
<label>Email :</label>
<input type="text" name="email" class="tbox" required/>
</fieldset>
<fieldset>
<label>Message :</label>
<textarea rows="5" cols="20" name="message" required></textarea>
</fieldset>
<fieldset>
Please enter security code
<div class="clear"></div>
<input type="text" name="vrcode" class="tbox"/>
</fieldset>
<fieldset>
<input type="submit" class="button" value="Submit"/>
<a href="#" id="closefeedbakcformLink">Close</a>
</fieldset>
</form>
</div>
<div class="clearfix"></div>
</div>
</div>
<div id="donate_popup" class="modal" style="max-width: 800px;">
<table width="100%" border="1">
<tr>
<td colspan="2" align="center">
<b>Support im4change</b>
</td>
</tr>
<tr>
<td width="25%" valign="middle">
<img src="https://im4change.in/images/logo2.jpg?1582080632" alt="" width="100%"/> </td>
<td style="padding-left:10px;padding-top:10px;">
<form action="https://im4change.in/donate" method="get">
<table width="100%" cellpadding="2" cellspacing="2">
<tr>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
10
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
100
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
1000
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
50
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
500
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
<input type="text" name="price" placeholder="?" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td colspan="3" align="right">
<input type="button" name="Pay" value="Pay"
style="width: 200px;background-color: rgb(205, 35, 36);color: #ffffff;"/>
</td>
</tr>
</table>
</form>
</td>
</tr>
</table>
</div><script type='text/javascript'>
/* <![CDATA[ */
var tievar = {'go_to': 'Go to...'};
/* ]]> */
</script>
<script src="/js/tie-scripts.js?1575549704"></script><script src="/js/bootstrap.js?1575549704"></script><script src="/js/jquery.modal.min.js?1578284310"></script><script>
$(document).ready(function() {
// tell the autocomplete function to get its data from our php script
$('#s').autocomplete({
source: "/autocomplete"
});
});
</script>
<script src="/vj-main-sw-register.js" async></script>
<script>function init(){var imgDefer=document.getElementsByTagName('img');for(var i=0;i<imgDefer.length;i++){if(imgDefer[i].getAttribute('data-src')){imgDefer[i].setAttribute('src',imgDefer[i].getAttribute('data-src'))}}}
window.onload=init;</script>
</body>
</html>'
}
$reasonPhrase = 'OK'
header - [internal], line ??
Cake\Http\ResponseEmitter::emitStatusLine() - CORE/src/Http/ResponseEmitter.php, line 148
Cake\Http\ResponseEmitter::emit() - CORE/src/Http/ResponseEmitter.php, line 54
Cake\Http\Server::emit() - CORE/src/Http/Server.php, line 141
[main] - ROOT/webroot/index.php, line 39
Warning (2): Cannot modify header information - headers already sent by (output started at /home/brlfuser/public_html/vendor/cakephp/cakephp/src/Error/Debugger.php:853) [CORE/src/Http/ResponseEmitter.php, line 181]
$response = object(Cake\Http\Response) {
'status' => (int) 200,
'contentType' => 'text/html',
'headers' => [
'Content-Type' => [
[maximum depth reached]
]
],
'file' => null,
'fileRange' => [],
'cookies' => object(Cake\Http\Cookie\CookieCollection) {},
'cacheDirectives' => [],
'body' => '<!DOCTYPE html>
<!--[if lt IE 7 ]>
<html class="ie ie6" lang='en'> <![endif]-->
<!--[if IE 7 ]>
<html class="ie ie7" lang='en'> <![endif]-->
<!--[if IE 8 ]>
<html class="ie ie8" lang='en'> <![endif]-->
<!--[if (gte IE 9)|!(IE)]><!-->
<html lang='en'>
<!--<![endif]-->
<head><meta http-equiv="Content-Type" content="text/html; charset=utf-8">
<title>
LATEST NEWS UPDATES | Steps to improve Healthcare in Rural India </title>
<meta name="description" content="
-Press Information Bureau (Ministry of Health and Family Welfare)
Healthcare for all, particularly for the rural areas has been a priority for the Government. The health indicators like Infant Mortality Rate (IMR), Total Fertility Rate (TFR), and nutritional status of children..."/>
<meta name="keywords" content="Public Health,Health,infant mortality"/>
<meta name="news_keywords" content="Public Health,Health,infant mortality">
<link rel="alternate" type="application/rss+xml" title="ROR" href="/ror.xml"/>
<link rel="alternate" type="application/rss+xml" title="RSS 2.0" href="/feeds/"/>
<link rel="stylesheet" href="/css/bootstrap.min.css?1697864993"/> <link rel="stylesheet" href="/css/style.css?v=1.1.2"/> <link rel="stylesheet" href="/css/style-inner.css?1577045210"/> <link rel="stylesheet" id="Oswald-css"
href="https://fonts.googleapis.com/css?family=Oswald%3Aregular%2C700&ver=3.8.1" type="text/css"
media="all">
<link rel="stylesheet" href="/css/jquery.modal.min.css?1578285302"/> <script src="/js/jquery-1.10.2.js?1575549704"></script> <script src="/js/jquery-migrate.min.js?1575549704"></script> <link rel="shortcut icon" href="/favicon.ico" title="Favicon">
<link rel="stylesheet" href="/css/jquery-ui.css?1580720609"/> <script src="/js/jquery-ui.js?1575549704"></script> <link rel="preload" as="style" href="https://www.im4change.org/css/custom.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery.modal.min.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/jquery-ui.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel="preload" as="style" href="https://www.im4change.org/css/li-scroller.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<!-- <link rel="preload" as="style" href="https://www.im4change.org/css/style.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous"> -->
<link rel="preload" as="style" href="https://www.im4change.org/css/style-inner.css" onload="this.rel='stylesheet'" media="all" crossorigin="anonymous">
<link rel='dns-prefetch' href="//im4change.org/css/custom.css" crossorigin >
<link rel="preload" as="script" href="https://www.im4change.org/js/bootstrap.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.li-scroller.1.0.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.modal.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery.ui.totop.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-1.10.2.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-migrate.min.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/jquery-ui.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/setting.js">
<link rel="preload" as="script" href="https://www.im4change.org/js/tie-scripts.js">
<!--[if IE]>
<script type="text/javascript">jQuery(document).ready(function () {
jQuery(".menu-item").has("ul").children("a").attr("aria-haspopup", "true");
});</script>
<![endif]-->
<!--[if lt IE 9]>
<script src="/js/html5.js"></script>
<script src="/js/selectivizr-min.js"></script>
<![endif]-->
<!--[if IE 8]>
<link rel="stylesheet" type="text/css" media="all" href="/css/ie8.css"/>
<![endif]-->
<meta property="og:title" content="LATEST NEWS UPDATES | Steps to improve Healthcare in Rural India" />
<meta property="og:url" content="https://im4change.in/latest-news-updates/steps-to-improve-healthcare-in-rural-india-24314.html" />
<meta property="og:type" content="article" />
<meta property="og:description" content="
-Press Information Bureau (Ministry of Health and Family Welfare)
Healthcare for all, particularly for the rural areas has been a priority for the Government. The health indicators like Infant Mortality Rate (IMR), Total Fertility Rate (TFR), and nutritional status of children..." />
<meta property="og:image" content="" />
<meta property="fb:app_id" content="0" />
<meta name="viewport" content="width=device-width, initial-scale=1, maximum-scale=1, user-scalable=no">
<link rel="apple-touch-icon-precomposed" sizes="144x144" href="https://im4change.in/images/apple1.png">
<link rel="apple-touch-icon-precomposed" sizes="120x120" href="https://im4change.in/images/apple2.png">
<link rel="apple-touch-icon-precomposed" sizes="72x72" href="https://im4change.in/images/apple3.png">
<link rel="apple-touch-icon-precomposed" href="https://im4change.in/images/apple4.png">
<style>
.gsc-results-wrapper-overlay{
top: 38% !important;
height: 50% !important;
}
.gsc-search-button-v2{
border-color: #035588 !important;
background-color: #035588 !important;
}
.gsib_a{
height: 30px !important;
padding: 2px 8px 1px 6px !important;
}
.gsc-search-button-v2{
height: 41px !important;
}
input.gsc-input{
background: none !important;
}
@media only screen and (max-width: 600px) {
.gsc-results-wrapper-overlay{
top: 11% !important;
width: 87% !important;
left: 9% !important;
height: 43% !important;
}
.gsc-search-button-v2{
padding: 10px 10px !important;
}
.gsc-input-box{
height: 28px !important;
}
/* .gsib_a {
padding: 0px 9px 4px 9px !important;
}*/
}
@media only screen and (min-width: 1200px) and (max-width: 1920px) {
table.gsc-search-box{
width: 15% !important;
float: right !important;
margin-top: -118px !important;
}
.gsc-search-button-v2 {
padding: 6px !important;
}
}
</style>
<script>
$(function () {
$("#accordion").accordion({
event: "click hoverintent"
});
});
/*
* hoverIntent | Copyright 2011 Brian Cherne
* http://cherne.net/brian/resources/jquery.hoverIntent.html
* modified by the jQuery UI team
*/
$.event.special.hoverintent = {
setup: function () {
$(this).bind("mouseover", jQuery.event.special.hoverintent.handler);
},
teardown: function () {
$(this).unbind("mouseover", jQuery.event.special.hoverintent.handler);
},
handler: function (event) {
var currentX, currentY, timeout,
args = arguments,
target = $(event.target),
previousX = event.pageX,
previousY = event.pageY;
function track(event) {
currentX = event.pageX;
currentY = event.pageY;
}
;
function clear() {
target
.unbind("mousemove", track)
.unbind("mouseout", clear);
clearTimeout(timeout);
}
function handler() {
var prop,
orig = event;
if ((Math.abs(previousX - currentX) +
Math.abs(previousY - currentY)) < 7) {
clear();
event = $.Event("hoverintent");
for (prop in orig) {
if (!(prop in event)) {
event[prop] = orig[prop];
}
}
// Prevent accessing the original event since the new event
// is fired asynchronously and the old event is no longer
// usable (#6028)
delete event.originalEvent;
target.trigger(event);
} else {
previousX = currentX;
previousY = currentY;
timeout = setTimeout(handler, 100);
}
}
timeout = setTimeout(handler, 100);
target.bind({
mousemove: track,
mouseout: clear
});
}
};
</script>
<script type="text/javascript">
var _gaq = _gaq || [];
_gaq.push(['_setAccount', 'UA-472075-3']);
_gaq.push(['_trackPageview']);
(function () {
var ga = document.createElement('script');
ga.type = 'text/javascript';
ga.async = true;
ga.src = ('https:' == document.location.protocol ? 'https://ssl' : 'http://www') + '.google-analytics.com/ga.js';
var s = document.getElementsByTagName('script')[0];
s.parentNode.insertBefore(ga, s);
})();
</script>
<link rel="stylesheet" href="/css/custom.css?v=1.16"/> <script src="/js/jquery.ui.totop.js?1575549704"></script> <script src="/js/setting.js?1575549704"></script> <link rel="manifest" href="/manifest.json">
<meta name="theme-color" content="#616163" />
<meta name="apple-mobile-web-app-capable" content="yes">
<meta name="apple-mobile-web-app-status-bar-style" content="black">
<meta name="apple-mobile-web-app-title" content="im4change">
<link rel="apple-touch-icon" href="/icons/logo-192x192.png">
</head>
<body id="top" class="home inner blog">
<div class="background-cover"></div>
<div class="wrapper animated">
<header id="theme-header" class="header_inner" style="position: relative;">
<div class="logo inner_logo" style="left:20px !important">
<a title="Home" href="https://im4change.in/">
<img src="https://im4change.in/images/logo2.jpg?1582080632" class="logo_image" alt="im4change"/> </a>
</div>
<div class="langhindi" style="color: #000;display:none;"
href="https://im4change.in/">
<a class="more-link" href="https://im4change.in/">Home</a>
<a href="https://im4change.in/hindi/" class="langbutton ">हिन्दी</a>
</div>
<nav class="fade-in animated2" id="main-nav">
<div class="container">
<div class="main-menu">
<ul class="menu" id="menu-main">
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
style="left: -40px;"><a
target="_blank" href="https://im4change.in/">Home</a>
</li>
<li class="menu-item mega-menu menu-item-type-taxonomy mega-menu menu-item-object-category mega-menu menu-item-has-children parent-list"
style=" margin-left: -40px;"><a href="#">KNOWLEDGE GATEWAY <span class="sub-indicator"></span>
</a>
<div class="mega-menu-block background_menu" style="padding-top:25px;">
<div class="container">
<div class="mega-menu-content">
<div class="mega-menu-item">
<h3><b>Farm Crisis</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/farmers039-suicides-14.html"
class="left postionrel">Farm Suicides </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/unemployment-30.html"
class="left postionrel">Unemployment </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/rural-distress-70.html"
class="left postionrel">Rural distress </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/migration-34.html"
class="left postionrel">Migration </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/key-facts-72.html"
class="left postionrel">Key Facts </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/farm-crisis/debt-trap-15.html"
class="left postionrel">Debt Trap </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Empowerment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/union-budget-73.html"
class="left postionrel">Union Budget And Other Economic Policies </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/forest-and-tribal-rights-61.html"
class="left postionrel">Forest and Tribal Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-education-60.html"
class="left postionrel">Right to Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-food-59.html"
class="left postionrel">Right to Food </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/displacement-3279.html"
class="left postionrel">Displacement </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-work-mg-nrega-39.html"
class="left postionrel">Right to Work (MG-NREGA) </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/gender-3280.html"
class="left postionrel">GENDER </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/right-to-information-58.html"
class="left postionrel">Right to Information </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/empowerment/social-audit-48.html"
class="left postionrel">Social Audit </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Hunger / HDI</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/poverty-and-inequality-20499.html"
class="left postionrel">Poverty and inequality </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/malnutrition-41.html"
class="left postionrel">Malnutrition </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/public-health-51.html"
class="left postionrel">Public Health </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/education-50.html"
class="left postionrel">Education </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hunger-overview-40.html"
class="left postionrel">Hunger Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/hdi-overview-45.html"
class="left postionrel">HDI Overview </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/pds-ration-food-security-42.html"
class="left postionrel">PDS/ Ration/ Food Security </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/sdgs-113.html"
class="left postionrel">SDGs </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/hunger-hdi/mid-day-meal-scheme-mdms-53.html"
class="left postionrel">Mid Day Meal Scheme (MDMS) </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Environment</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/time-bomb-ticking-52.html"
class="left postionrel">Time Bomb Ticking </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/water-and-sanitation-55.html"
class="left postionrel">Water and Sanitation </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/environment/impact-on-agriculture-54.html"
class="left postionrel">Impact on Agriculture </a>
</p>
</div>
<div class="mega-menu-item">
<h3><b>Law & Justice</b></h3>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/social-justice-20500.html"
class="left postionrel">Social Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/access-to-justice-47.html"
class="left postionrel">Access to Justice </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/human-rights-56.html"
class="left postionrel">Human Rights </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/corruption-35.html"
class="left postionrel">Corruption </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/general-insecurity-46.html"
class="left postionrel">General Insecurity </a>
</p>
<p style="padding-left:5px;">
<a target="_blank" href="https://im4change.in/law-justice/disaster-relief-49.html"
class="left postionrel">Disaster & Relief </a>
</p>
</div>
</div>
</div>
</div>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page "><a target="_blank" href="https://im4change.in/nceus_reports.php">NCEUS reports</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children parent-list ">
<a target="_blank" href="https://im4change.in/about-us-9.html">About Us <span
class="sub-indicator"></span></a>
<ul class="sub-menu aboutmenu">
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/objectives-8.html">Objectives</a>
</li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/contactus.php">Contact
Us</a></li>
<li class="menu-item menu-item-type-post_type menu-item-object-page"><a
target="_blank" href="https://im4change.in/about-us-9.html">About
Us</a></li>
</ul>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children ">
<a target="_blank" href="https://im4change.in/fellowships.php" title="Fellowships">Fellowships</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/media-workshops.php">Workshops</a>
</li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/research.php">Research</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children "><a
target="_blank" href="https://im4change.in/links-64">Partners</a></li>
<li class="menu-item menu-item-type-custom menu-item-object-custom menu-item-has-children"
id="menu-item-539"><a target="_blank" href="https://im4change.in/hindi/"
class="langbutton langlinkfont17">हिन्दी</a></li>
</ul>
</div> </div>
<!-- <div style="float: right;">
<script async src="https://cse.google.com/cse.js?cx=18b4f2e0f11bed3dd"></script>
<div class="gcse-search"></div>
</div> -->
<div class="search-block" style=" margin-left: 8px; margin-right: 7px;">
<form method="get" id="searchform" name="searchform"
action="https://im4change.in/search"
onsubmit="return searchvalidate();">
<button class="search-button" type="submit" value="Search"></button>
<input type="text" id="s" name="qryStr" value=""
onfocus="if (this.value == 'Search...') {this.value = '';}"
onblur="if (this.value == '') {this.value = 'Search...';}">
</form>
</div>
</nav>
</header>
<div class="container">
<div id="main-content" class=" main1 container fade-in animated3 sidebar-narrow-left">
<div class="content-wrap">
<div class="content" style="width: 900px;min-height: 500px;">
<section class="cat-box recent-box innerCatRecent">
<h1 class="cat-box-title">Steps to improve Healthcare in Rural India</h1>
<a href="JavaScript:void(0);" onclick="return shareArticle(24141);">
<img src="https://im4change.in/images/email.png?1582080630" border="0" width="24" align="right" alt="Share this article"/> </a>
<a href="https://im4change.in/latest-news-updates/steps-to-improve-healthcare-in-rural-india-24314/print"
rel="nofollow">
<img src="https://im4change.in/images/icon-print.png?1582080630" border="0" width="24" align="right" alt="Share this article"/>
</a>
</section>
<section class="recent-box innerCatRecent">
<small class="pb-1"><span class="dateIcn">
<img src="https://im4change.in/images/published.svg?1582080666" alt="published"/>
Published on</span><span class="text-date"> Feb 21, 2014</span>
<span
class="dateIcn">
<img src="https://im4change.in/images/modified.svg?1582080666" alt="modified"/> Modified on </span><span class="text-date"> Feb 21, 2014</span>
</small>
</section>
<div class="clear"></div>
<div style="padding-top: 10px;">
<div class="innerLineHeight">
<div class="middleContent innerInput latest-news-updates">
<table>
<tr>
<td>
<div>
<div align="justify">-Press Information Bureau (Ministry of Health and Family Welfare)</div><p align="justify"><br />Healthcare for all, particularly for the rural areas has been a priority for the Government. The health indicators like Infant Mortality Rate (IMR), Total Fertility Rate (TFR), and nutritional status of children under 3 years including prevalence of anemia amongst them and pregnant women in rural area are considerably poor as compared to urban areas. The key health indicators are as under:</p><p align="justify"><img src="https://im4change.in/siteadmin/tinymce/uploaded/Health_2.JPG" alt="Health" width="602" height="187" /></p><p align="justify">Public Health is a state subject. However, Central Government launched NRHM in 2005 to provide financial support to the States/UTs to strengthen their health systems particularly to cater to the healthcare needs of rural areas. Key steps taken to improve health care in rural areas include the following:</p><p align="justify"> </p><p align="justify"> i. Support is provided to States/UTs under NRHM, to strengthen the health system including establishment/up-gradation/renovation of health infrastructure, engagement of Nurses, doctors and specialist on contractual basis based on the appraisal of requirements proposed by the States in their Programme Implementation Plans (PIP),</p><p align="justify"> ii. Support under NRHM is also provided by way of additional incentives to serve in remote underserved areas, so that health professionals find it attractive to join public health facilities in such areas. In order to encourage the States to fill up existing vacancies in remote rural areas, the states are being incentivized to ensure rational deployment of health human resource. Manpower deployment is also to be put on the web in public domain,</p><p align="justify"> iii. To increase the availability of doctors, several initiatives have been taken to rationalize the norms in medical education, such as, relaxation in land requirements, bed strength, increase in ceiling for maximum intake for undergraduates, enhancement of teacher-student ratio in Post Graduate Courses, etc., which has resulted in substantial increase in number of undergraduate and post graduate seats. Government has also approved setting up of ANM/GNM Schools in different States besides setting up of Institutes of Paramedical Sciences at National and regional levels,</p><p align="justify"> iv. States/UTs are being impressed upon from time to time to make available improved health facilities including free essential medicines in all public health facilities. Accordingly, financial support is being provided for ensuring uninterrupted supply of free essential medicines in public health facilities based on the requirement proposed by the States in their PIPs. An incentive of upto 5% of the NRHM outlay has also been introduced in 2012-13 for states for establishing policy framework and systems for providing free generic medicines to those who access public health facilities.</p><p align="justify"> v. States/UTs are being provided support for focused attention and greater resources per capita to high priority districts with relatively poor composite health index.</p><p align="justify"> vi. Financial assistance is provided to the States/UTs for selection and training of Accredited Social Health Activists (ASHA), who act as a link between community and healthcare facilities.</p><p align="justify"> vii. States/UTs are supported with Mobile Medical Units for improved service delivery especially in hard to reach areas. There are over 2000 MMUs that are being supported under NRHM. Support is also provided for Emergency Referral Transport services to ensure in-interrupted referral services. There are over 20000 ambulances that are being supported under NRHM.</p><p align="justify">viii. States/UTs are assisted to constitute Village Health, Sanitation and Nutrition Committees so as to ensure community participation and village level planning and monitoring of health activities.</p><p align="justify"> ix. New initiatives such as Janani Shishu Suraksha Karyakram (JSSK), Rashtriya Bal Swashthya Karyrakram (RBSK), Rashtriya Kishore Swashthya Karyakram (RKSK), ‘National Health Mission Free Drugs Service Initiative' etc., have also been introduced to inter-alia make health care affordable by reducing out of pocket expenditure.</p><p align="justify"> </p><p align="justify">Presently, there is no proposal to revise the existing National Health Policy (NHP) - 2002. The Twelfth Plan seeks to strengthen initiatives taken in the Eleventh Plan to expand the reach of health care and work towards the long term objective of establishing a system of Universal Health Coverage (UHC) in the country. This means that each individual would have assured access to a defined essential range of medicines and treatment at an affordable price, which should be entirely free for large percentage of the population. Inevitably, the list of assured services will have to be limited by budgetary constraints. Further, to ensure equitable health care to bring about sharper improvements in health outcomes, at least 25% of all districts in each state have been identified as high priority districts based on a composite health index. These also include all tribal and LWE affected districts which are below the State's average of composite health index. These districts would receive higher per capita funding, enhanced monitoring, focused supportive supervision and have differential planning norms. These measures would help reduce prevailing health inequalities in rural areas.</p><p align="justify"> </p><p align="justify">This was stated by Shri Ghulam Nabi Azad, Union Minister for Health and Family Welfare in a written reply to the Lok Sabha today.</p><p align="justify">*********</p><p align="justify">MV/GM</p><p align="justify">(Release ID :104096)</p>
</div>
</td>
</tr>
</table>
</div>
</div>
</div>
<div class="clear"></div>
<br><a href="http://www.pib.nic.in/newsite/erelease.aspx?relid=0" class="re" target="_blank">Press Information Bureau, 21 February, 2014, http://www.pib.nic.in/newsite/erelease.aspx?relid=0</a><div class="clear"></div>
<div style="padding-top: 18px;">
<p class="post-tag">Tagged with:
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Public Health"
title="Public Health">
Public Health </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=Health"
title="Health">
Health </a>
<a class="tagcloud5"
href="https://im4change.in/search?qryStr=infant mortality"
title="infant mortality">
infant mortality </a>
</p>
</div>
<div class="clear"></div>
<br><br>
<div class="widget-top">
<h4>Related Articles</h4>
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<ul id="recentcomments">
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/fifth-report-from-gambia-implicates-indian-drug-maker-for-contaminated-syrups-banjot-kaur.html"
title="Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur">
Fifth Report From Gambia Implicates Indian Drug Maker for Contaminated Syrups - Banjot Kaur </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-may-have-seen-steepest-dip-in-multidimensional-poverty-among-110-nations-as-per-undp-data-nikhil-rampal.html"
title="India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal">
India may have seen steepest dip in multidimensional poverty among 110 nations as per UNDP data - Nikhil Rampal </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/health-among-top-three-priorities-for-indian-voters-after-jobs-and-education-survey-shows-oliver-heath-jyoti-mishra-louise-tillin-sandhya-venkateswaran.html"
title="Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran">
Health among top three priorities for Indian voters after jobs and education, survey shows - Oliver Heath, Jyoti Mishra, Louise Tillin & Sandhya Venkateswaran </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/prevalence-of-zero-food-among-infants-and-young-children-in-india-patterns-of-change-across-the-states-and-union-territories-of-india-1993-2021-the-lancet.html"
title="Prevalence of Zero-Food among infants and young children in India - The Lancet ">
Prevalence of Zero-Food among infants and young children in India - The Lancet </a>
</li>
<li class="recentcomments">
<a href="https://im4change.in/latest-news-updates/india-s-sustainability-goals-at-risk-because-of-extreme-heatwaves-carbon-copy.html"
title="India's Sustainability Goals at Risk Because of Extreme Heatwaves - Carbon Copy">
India's Sustainability Goals at Risk Because of Extreme Heatwaves - Carbon Copy </a>
</li>
</ul>
</div>
<div class="comment-respond" id="respond">
<a name="commentbox"> </a>
<h3 class="comment-reply-title" id="reply-title">Write Comments</h3>
<form method="post" accept-charset="utf-8" role="form" action="/latest-news-updates/steps-to-improve-healthcare-in-rural-india-24314.html"><div style="display:none;"><input type="hidden" name="_method" value="POST"/></div> <form class="comment-form" id="commentform" method="post" action="#commentbox" onSubmit="return validate()"
name="cmtform">
<input type="hidden" name="cmttype" value="articlecmt"/>
<input type="hidden" name="article_id" value="24141"/>
<p class="comment-notes">Your email address will not be published. Required fields are marked <span
class="required">*</span></p>
<p class="comment-form-author">
<label for="commenterName">Name</label>
<span class="required">*</span>
<input type="text" aria-required="true" size="30"
value=""
name="commenterName" id="commenterName" required="true">
</p>
<p class="comment-form-email">
<label for="commenterEmail">Email</label> <span class="required">*</span>
<input aria-required="true" size="30" name="commenterEmail" id="commenterEmail" type="email"
value=""
required="true">
</p>
<p class="comment-form-contact">
<label for="commenterPh">Contact No.</label>
<input type="text" size="30"
value=""
name="commenterPh" id="commenterPh">
</p>
<p class="comment-form-comment">
<label for="comment">Comment</label>
<textarea aria-required="true" required="true" rows="8" cols="45" name="comment"
id="comment"></textarea>
</p>
<p class="comment-form-comment">
<label for="comment">Type the characters you see in the image below <span class="required">*</span><br><img
class="captchaImg"
src="https://im4change.in/securimage_show_art.php?tk=459709222" alt="captcha"/>
</label>
</p>
<input type="text" name="vrcode" required="true"/>
<p class="form-submit" style="width: 200px;">
<input type="submit" value="Post Comment" id="submit" name="submit">
</p></form>
</div>
<style>
.ui-widget-content {
height: auto !important;
}
</style>
<div id="share-modal"></div>
<style>
.middleContent a{
background-color: rgba(108,172,228,.2);
}
.middleContent a:hover{
background-color: #418fde;
border-color: #418fde;
color: #000;
}
</style>
<script>
function shareArticle(article_id) {
var options = {
modal: true,
height: 'auto',
width: 600 + 'px'
};
$('#share-modal').html("");
$('#share-modal').load('https://im4change.in/share_article?article_id=' + article_id).dialog(options).dialog('open');
}
function postShare() {
var param = 'article_id=' + $("#article_id").val();
param = param + '&y_name=' + $("#y_name").val();
param = param + '&y_email=' + $("#y_email").val();
param = param + '&f_name=' + $("#f_name").val();
param = param + '&f_email=' + $("#f_email").val();
param = param + '&y_msg=' + $("#y_msg").val();
$.ajax({
type: "POST",
url: 'https://im4change.in/post_share_article',
data: param,
success: function (response) {
$('#share-modal').html("Thank You, Your message posted to ");
}
});
return false;
}
</script> </div>
</div>
<!-- Right Side Section Start -->
<!-- MAP Section START -->
<aside class="sidebar indexMarg">
<div class="ad-cell">
<a href="https://im4change.in/statemap.php" title="">
<img src="https://im4change.in/images/map_new_version.png?1582080666" alt="India State Map" class="indiamap" width="232" height="252"/> </a>
<div class="rightmapbox">
<div id="sideOne" class="docltitle"><a href="https://im4change.in/state-report/india/36" target="_blank">DOCUMENTS/
REPORTS</a></div>
<div id="sideTwo" class="statetitle"><a href="https://im4change.in/states.php"target="_blank">STATE DATA/
HDRs.</a></div>
</div>
<div class="widget widgePadTop"></div>
</div>
</aside>
<!-- MAP Section END -->
<aside class="sidebar sidePadbottom">
<div class="rightsmlbox1" >
<a href="https://im4change.in/knowledge_gateway" target="_blank" style="color: #035588;
font-size: 17px;">
KNOWLEDGE GATEWAY
</a>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/newsletter" target="_blank">
NEWSLETTER
</a>
</p>
</div>
</div>
<div class="rightsmlbox1" style="height: 325px;">
<div>
<p class="rightsmlbox1_title">
Interview with Prof. Ravi Srivastava
</p>
<p class="rightsmlbox1_title">
<a href="https://im4change.in/video/interview-with-prof-ravi-srivastava-on-current-economic-crisis">
<img width="250" height="200" src="/images/interview_video_home.jpg" alt="Interview with Prof. Ravi Srivastava"/>
</a>
<!--
<iframe width="250" height="200" src="https://www.youtube.com/embed/MmaTlntk-wc" frameborder="0" allow="accelerometer; autoplay; encrypted-media; gyroscope; picture-in-picture" allowfullscreen=""></iframe>-->
</p>
<a href="https://im4change.in/videogallery" class="more-link CatArchalAnch1" target="_blank">
More videos
</a>
</div>
</div>
<div class="rightsmlbox1">
<div>
<!--div id="sstory" class="rightboxicons"></div--->
<p class="rightsmlbox1_title"><a href="https://im4change.in/list-success-stories" target="_blank">Success Stories</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/interviews" target="_blank">Interviews</a>
</p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a href="https://www.commoncause.in/page.php?id=10" >Donate</a></p>
</div>
</div>
<div class="rightsmlbox1">
<div>
<p class="rightsmlbox1_title"><a
href="https://im4change.in/marquee"
class="isf_link more-link" title="India Focus?" style="border: 4px solid #fdd922;width: 90%;background-color: #fdd922;text-align: center;color: #000000;font-size:18px" target="_blank">India Focus</a></p> </div>
</div>
<div class="rightsmlbox1" style="height: 104px !important;">
<a href="https://im4change.in/quarterly_reports.php" target="_blank">
Quarterly Reports on Effect of Economic Slowdown on Employment in India (2008 - 2015)
</a>
</div>
<!-- <div class="rightsmlbox1">
<a href="https://play.google.com/store/apps/details?id=com.im4.im4change" target="_blank">
</a></div> -->
<!-- <section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">Most Visited</h2>
</section> -->
<!-- accordion Starts here -->
<!-- <div id="accordion" class="accordMarg">
</div> -->
<!-- accordion ends here -->
<!-- Widget Tag Cloud Starts here -->
<div id="tag_cloud-2" class="widget widget_tag_cloud">
<section class="cat-box recent-box secMarg">
<h2 class="cat-box-title">MOST VISITED TAGS</h2>
</section>
<div class="widget-top wiPdTp">
<div class="stripe-line"></div>
</div>
<div class="widget-container">
<div class="tagcloud">
<a href="https://im4change.in/search?qryStr=Agriculture"
target="_blank" class="tag-link-4 font4">Agriculture</a>
<a href="https://im4change.in/search?qryStr=Food Security"
target="_blank" class="tag-link-4 font4">Food Security</a>
<a href="https://im4change.in/search?qryStr=Law and Justice"
target="_blank" class="tag-link-4 font4">Law and Justice</a>
<a href="https://im4change.in/search?qryStr=Health"
target="_blank" class="tag-link-4 font4">Health</a>
<a href="https://im4change.in/search?qryStr=Right to Food"
target="_blank" class="tag-link-4 font4">Right to Food</a>
<a href="https://im4change.in/search?qryStr=Corruption"
target="_blank" class="tag-link-4 font4">Corruption</a>
<a href="https://im4change.in/search?qryStr=farming"
target="_blank" class="tag-link-4 font4">farming</a>
<a href="https://im4change.in/search?qryStr=Environment"
target="_blank" class="tag-link-4 font4">Environment</a>
<a href="https://im4change.in/search?qryStr=Right to Information"
target="_blank" class="tag-link-4 font4">Right to Information</a>
<a href="https://im4change.in/search?qryStr=NREGS"
target="_blank" class="tag-link-4 font4">NREGS</a>
<a href="https://im4change.in/search?qryStr=Human Rights"
target="_blank" class="tag-link-4 font4">Human Rights</a>
<a href="https://im4change.in/search?qryStr=Governance"
target="_blank" class="tag-link-4 font4">Governance</a>
<a href="https://im4change.in/search?qryStr=PDS"
target="_blank" class="tag-link-4 font4">PDS</a>
<a href="https://im4change.in/search?qryStr=COVID-19"
target="_blank" class="tag-link-4 font4">COVID-19</a>
<a href="https://im4change.in/search?qryStr=Land Acquisition"
target="_blank" class="tag-link-4 font4">Land Acquisition</a>
<a href="https://im4change.in/search?qryStr=mgnrega"
target="_blank" class="tag-link-4 font4">mgnrega</a>
<a href="https://im4change.in/search?qryStr=Farmers"
target="_blank" class="tag-link-4 font4">Farmers</a>
<a href="https://im4change.in/search?qryStr=transparency"
target="_blank" class="tag-link-4 font4">transparency</a>
<a href="https://im4change.in/search?qryStr=Gender"
target="_blank" class="tag-link-4 font4">Gender</a>
<a href="https://im4change.in/search?qryStr=Poverty"
target="_blank" class="tag-link-4 font4">Poverty</a>
<a href="https://im4change.in/search?qryStr=Farm Laws" target="_blank" class="tag-link-4 font4">Farm Laws
</a>
<a href="https://im4change.in/search?qryStr=Citizenship Amendment Act" target="_blank" class="tag-link-4 font4">Citizenship Amendment Act
</a>
<a href="https://im4change.in/search?qryStr=CAA NPR NRIC" target="_blank" class="tag-link-4 font4">CAA NPR NRIC
</a>
<a href="https://im4change.in/search?qryStr=Job Losses" target="_blank" class="tag-link-4 font4">Job Losses
</a>
<a href="https://im4change.in/search?qryStr=Migrant Workers" target="_blank" class="tag-link-4 font4">Migrant Workers
</a>
<a href="https://im4change.in/search?qryStr=Unemployment" target="_blank" class="tag-link-4 font4">Unemployment
</a>
<a href="https://im4change.in/search?qryStr=PMGKAY" target="_blank" class="tag-link-4 font4">PMGKAY
</a>
<a href="https://im4change.in/search?qryStr=PM-KISAN" target="_blank" class="tag-link-4 font4">PM-KISAN
</a>
<a href="https://im4change.in/search?qryStr=PM-CARES" target="_blank" class="tag-link-4 font4">PM-CARES
</a>
<a href="https://im4change.in/search?qryStr=LFPR" target="_blank" class="tag-link-4 font4">LFPR
</a>
</div>
</div>
</div>
<!-- Widget Tag Cloud Ends here -->
</aside>
<!-- Right Side Section End -->
</div>
<section class="cat-box cats-review-box footerSec">
<h2 class="cat-box-title vSec CatArcha">Video
Archives</h2>
<h2 class="cat-box-title CatArchaTitle">Archives</h2>
<div class="cat-box-content">
<div class="reviews-cat">
<div class="CatArchaDiv1">
<div class="CatArchaDiv2">
<ul>
<li>
<a href="https://im4change.in/news-alerts-57/moving-upstream-luni-fellowship.html" target="_blank">
Moving Upstream: Luni – Fellowship </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/135-million-indians-exited-multidimensional-poverty-as-per-government-figures-is-that-the-same-as-poverty-reduction.html" target="_blank">
135 Million Indians Exited “Multidimensional" Poverty as per Government... </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/explainer-why-are-tomato-prices-on-fire.html" target="_blank">
Explainer: Why are Tomato Prices on Fire? </a>
</li>
<li>
<a href="https://im4change.in/news-alerts-57/nsso-survey-only-39-1-of-all-households-have-drinking-water-within-dwelling-46-7-of-rural-households-use-firewood-for-cooking.html" target="_blank">
NSSO Survey: Only 39.1% of all Households have Drinking... </a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/news-alerts-57"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/I51LYnP8BOk/1.jpg"
alt=" Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Short-Video-on-im4change-Hindi-website-Inclusive-Media-for-Change" target="_blank">
Im4Change.org हिंदी वेबसाइट का परिचय. Short Video on im4change.org... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/kNqha-SwfIY/1.jpg"
alt=" "Session 1: Scope of IDEA and AgriStack" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-1- Scope-of-IDEA-and-AgriStack-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 1: Scope of IDEA and AgriStack" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/6kIVjlgZItk/1.jpg"
alt=" "Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-2-Farmer-Centric-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 2: Farmer Centric Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="CatArchaWidth">
<img class="CatArchaImg"
src="https://img.youtube.com/vi/2BeHTu0y7xc/1.jpg"
alt=" "Session 3: Future of Digitalisation in Agriculture" in Exploring...">
<p class="CatArchaPPad">
<a href="https://im4change.in/video/Session-3-Future-of-Digitalisation-in-Agriculture-in-Exploring-Digitalisation-in-Agriculture-29-April-2022" target="_blank">
"Session 3: Future of Digitalisation in Agriculture" in Exploring... </a>
</p>
</div>
<div class="divWidth">
<ul class="divWidthMarg">
<li>
<a href="https://im4change.in/video/Public-Spending-on-Agriculture-in-India-Source-Foundation-for-Agrarian-Studies"
title="Public Spending on Agriculture in India (Source: Foundation for Agrarian Studies)" target="_blank">
Public Spending on Agriculture in India (Source: Foundation for...</a>
</li>
<li>
<a href="https://im4change.in/video/Agrarian-Change-Seminar-Protests-against-the-New-Farm-Laws-in-India-by-Prof-Vikas-Rawal-JNU-Source-Journal-Of-Agrarian-Change"
title="Agrarian Change Seminar: 'Protests against the New Farm Laws in India' by Prof. Vikas Rawal, JNU (Source: Journal Of Agrarian Change) " target="_blank">
Agrarian Change Seminar: 'Protests against the New Farm Laws...</a>
</li>
<li>
<a href="https://im4change.in/video/Webinar-Ramrao-The-Story-of-India-Farm-Crisis-Source-Azim-Premji-University"
title="Webinar: Ramrao - The Story of India's Farm Crisis (Source: Azim Premji University)" target="_blank">
Webinar: Ramrao - The Story of India's Farm Crisis...</a>
</li>
<li>
<a href="https://im4change.in/video/water-and-agricultural-transformation-in-India"
title="Water and Agricultural Transformation in India: A Symbiotic Relationship (Source: IGIDR)" target="_blank">
Water and Agricultural Transformation in India: A Symbiotic Relationship...</a>
</li>
<li class="CatArchalLi1">
<a href="https://im4change.in/videogallery"
class="more-link CatArchalAnch1" target="_blank">
More...
</a>
</li>
</ul>
</div>
</div>
</div>
</div>
</section> </div>
<div class="clear"></div>
<!-- Footer option Starts here -->
<div class="footer-bottom fade-in animated4">
<div class="container">
<div class="social-icons icon_flat">
<p class="SocialMargTop"> Website Developed by <a target="_blank" title="Web Development"
class="wot right"
href="http://www.ravinderkhurana.com/" rel="nofollow">
RAVINDErkHURANA.com</a></p>
</div>
<div class="alignleft">
<a
target="_blank" href="https://im4change.in/objectives-8.html"
class="link"
title="Objectives">Objectives</a> | <a
target="_blank" href="https://im4change.in/about-us-9.html"
class="link" title="About Us">About Us</a> | <a
target="_blank" href="https://im4change.in/media-workshops.php"
class="ucwords">Workshops</a> | <a
target="_blank" href="https://im4change.in/disclaimer/disclaimer-149.html"
title="Disclaimer">Disclaimer</a> </div>
</div>
</div>
<!-- Footer option ends here -->
</div>
<div id="connect">
<a target="_blank"
href="http://www.facebook.com/sharer.php?u=https://im4change.in/latest-news-updates/steps-to-improve-healthcare-in-rural-india-24314.html"
title="Share on Facebook">
<img src="https://im4change.in/images/Facebook.png?1582080640" alt="share on Facebook" class="ImgBorder"/>
</a><br/>
<a target="_blank"
href="http://twitter.com/share?text=Im4change&url=https://im4change.in/latest-news-updates/steps-to-improve-healthcare-in-rural-india-24314.html"
title="Share on Twitter">
<img src="https://im4change.in/images/twitter.png?1582080632" alt="Twitter" class="ImgBorder"/> </a>
<br/>
<a href="/feeds" title="RSS Feed" target="_blank">
<img src="https://im4change.in/images/rss.png?1582080632" alt="RSS" class="ImgBorder"/>
</a>
<br/>
<a class="feedback-link" id="feedbackFormLink" href="#">
<img src="https://im4change.in/images/feedback.png?1582080630" alt="Feedback" class="ImgBorder"/>
</a> <br/>
<a href="javascript:function iprl5(){var d=document,z=d.createElement('scr'+'ipt'),b=d.body,l=d.location;try{if(!b)throw(0);d.title='(Saving...) '+d.title;z.setAttribute('src',l.protocol+'//www.instapaper.com/j/WKrH3R7ORD5p?u='+encodeURIComponent(l.href)+'&t='+(new Date().getTime()));b.appendChild(z);}catch(e){alert('Please wait until the page has loaded.');}}iprl5();void(0)"
class="bookmarklet" onclick="return explain_bookmarklet();">
<img src="https://im4change.in/images/read-it-later.png?1582080632" alt="Read Later" class="ImgBorder"/> </a>
</div>
<!-- Feedback form Starts here -->
<div id="feedbackForm" class="overlay_form" class="ImgBorder">
<h2>Contact Form</h2>
<div id="contactform1">
<div id="formleft">
<form id="submitform" action="/contactus.php" method="post">
<input type="hidden" name="submitform" value="submitform"/>
<input type="hidden" name="salt_key" value="a0e0f2c6a0644a70e57ad2c96829709a"/>
<input type="hidden" name="ref" value="feedback"/>
<fieldset>
<label>Name :</label>
<input type="text" name="name" class="tbox" required/>
</fieldset>
<fieldset>
<label>Email :</label>
<input type="text" name="email" class="tbox" required/>
</fieldset>
<fieldset>
<label>Message :</label>
<textarea rows="5" cols="20" name="message" required></textarea>
</fieldset>
<fieldset>
Please enter security code
<div class="clear"></div>
<input type="text" name="vrcode" class="tbox"/>
</fieldset>
<fieldset>
<input type="submit" class="button" value="Submit"/>
<a href="#" id="closefeedbakcformLink">Close</a>
</fieldset>
</form>
</div>
<div class="clearfix"></div>
</div>
</div>
<div id="donate_popup" class="modal" style="max-width: 800px;">
<table width="100%" border="1">
<tr>
<td colspan="2" align="center">
<b>Support im4change</b>
</td>
</tr>
<tr>
<td width="25%" valign="middle">
<img src="https://im4change.in/images/logo2.jpg?1582080632" alt="" width="100%"/> </td>
<td style="padding-left:10px;padding-top:10px;">
<form action="https://im4change.in/donate" method="get">
<table width="100%" cellpadding="2" cellspacing="2">
<tr>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
10
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
100
</td>
<td width="33%" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
1000
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
50
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
500
</td>
<td style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
<input type="text" name="price" placeholder="?" style="font-family: 'Script Font', cursive, Arial;font-size: 20px;font-weight: 700;">
</td>
</tr>
<tr>
<td colspan="3">
</td>
</tr>
<tr>
<td colspan="3" align="right">
<input type="button" name="Pay" value="Pay"
style="width: 200px;background-color: rgb(205, 35, 36);color: #ffffff;"/>
</td>
</tr>
</table>
</form>
</td>
</tr>
</table>
</div><script type='text/javascript'>
/* <![CDATA[ */
var tievar = {'go_to': 'Go to...'};
/* ]]> */
</script>
<script src="/js/tie-scripts.js?1575549704"></script><script src="/js/bootstrap.js?1575549704"></script><script src="/js/jquery.modal.min.js?1578284310"></script><script>
$(document).ready(function() {
// tell the autocomplete function to get its data from our php script
$('#s').autocomplete({
source: "/autocomplete"
});
});
</script>
<script src="/vj-main-sw-register.js" async></script>
<script>function init(){var imgDefer=document.getElementsByTagName('img');for(var i=0;i<imgDefer.length;i++){if(imgDefer[i].getAttribute('data-src')){imgDefer[i].setAttribute('src',imgDefer[i].getAttribute('data-src'))}}}
window.onload=init;</script>
</body>
</html>'
}
$cookies = []
$values = [
(int) 0 => 'text/html; charset=UTF-8'
]
$name = 'Content-Type'
$first = true
$value = 'text/html; charset=UTF-8'
header - [internal], line ??
Cake\Http\ResponseEmitter::emitHeaders() - CORE/src/Http/ResponseEmitter.php, line 181
Cake\Http\ResponseEmitter::emit() - CORE/src/Http/ResponseEmitter.php, line 55
Cake\Http\Server::emit() - CORE/src/Http/Server.php, line 141
[main] - ROOT/webroot/index.php, line 39
LATEST NEWS UPDATES | Steps to improve Healthcare in Rural India
Published on Feb 21, 2014 Modified on Feb 21, 2014
-Press Information Bureau (Ministry of Health and Family Welfare)
Healthcare for all, particularly for the rural areas has been a priority for the Government. The health indicators like Infant Mortality Rate (IMR), Total Fertility Rate (TFR), and nutritional status of children under 3 years including prevalence of anemia amongst them and pregnant women in rural area are considerably poor as compared to urban areas. The key health indicators are as under:
Public Health is a state subject. However, Central Government launched NRHM in 2005 to provide financial support to the States/UTs to strengthen their health systems particularly to cater to the healthcare needs of rural areas. Key steps taken to improve health care in rural areas include the following:
i. Support is provided to States/UTs under NRHM, to strengthen the health system including establishment/up-gradation/renovation of health infrastructure, engagement of Nurses, doctors and specialist on contractual basis based on the appraisal of requirements proposed by the States in their Programme Implementation Plans (PIP),
ii. Support under NRHM is also provided by way of additional incentives to serve in remote underserved areas, so that health professionals find it attractive to join public health facilities in such areas. In order to encourage the States to fill up existing vacancies in remote rural areas, the states are being incentivized to ensure rational deployment of health human resource. Manpower deployment is also to be put on the web in public domain,
iii. To increase the availability of doctors, several initiatives have been taken to rationalize the norms in medical education, such as, relaxation in land requirements, bed strength, increase in ceiling for maximum intake for undergraduates, enhancement of teacher-student ratio in Post Graduate Courses, etc., which has resulted in substantial increase in number of undergraduate and post graduate seats. Government has also approved setting up of ANM/GNM Schools in different States besides setting up of Institutes of Paramedical Sciences at National and regional levels,
iv. States/UTs are being impressed upon from time to time to make available improved health facilities including free essential medicines in all public health facilities. Accordingly, financial support is being provided for ensuring uninterrupted supply of free essential medicines in public health facilities based on the requirement proposed by the States in their PIPs. An incentive of upto 5% of the NRHM outlay has also been introduced in 2012-13 for states for establishing policy framework and systems for providing free generic medicines to those who access public health facilities.
v. States/UTs are being provided support for focused attention and greater resources per capita to high priority districts with relatively poor composite health index.
vi. Financial assistance is provided to the States/UTs for selection and training of Accredited Social Health Activists (ASHA), who act as a link between community and healthcare facilities.
vii. States/UTs are supported with Mobile Medical Units for improved service delivery especially in hard to reach areas. There are over 2000 MMUs that are being supported under NRHM. Support is also provided for Emergency Referral Transport services to ensure in-interrupted referral services. There are over 20000 ambulances that are being supported under NRHM.
viii. States/UTs are assisted to constitute Village Health, Sanitation and Nutrition Committees so as to ensure community participation and village level planning and monitoring of health activities.
ix. New initiatives such as Janani Shishu Suraksha Karyakram (JSSK), Rashtriya Bal Swashthya Karyrakram (RBSK), Rashtriya Kishore Swashthya Karyakram (RKSK), ‘National Health Mission Free Drugs Service Initiative' etc., have also been introduced to inter-alia make health care affordable by reducing out of pocket expenditure.
Presently, there is no proposal to revise the existing National Health Policy (NHP) - 2002. The Twelfth Plan seeks to strengthen initiatives taken in the Eleventh Plan to expand the reach of health care and work towards the long term objective of establishing a system of Universal Health Coverage (UHC) in the country. This means that each individual would have assured access to a defined essential range of medicines and treatment at an affordable price, which should be entirely free for large percentage of the population. Inevitably, the list of assured services will have to be limited by budgetary constraints. Further, to ensure equitable health care to bring about sharper improvements in health outcomes, at least 25% of all districts in each state have been identified as high priority districts based on a composite health index. These also include all tribal and LWE affected districts which are below the State's average of composite health index. These districts would receive higher per capita funding, enhanced monitoring, focused supportive supervision and have differential planning norms. These measures would help reduce prevailing health inequalities in rural areas.
This was stated by Shri Ghulam Nabi Azad, Union Minister for Health and Family Welfare in a written reply to the Lok Sabha today.
 Published on Feb 21, 2014
Published on Feb 21, 2014
 Modified on Feb 21, 2014
Modified on Feb 21, 2014
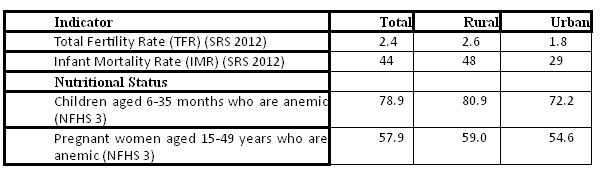









Write Comments